
The streptococci are a large heterogeneous group of gram-positive spherically shaped bacteria widely distributed in nature. They include some of the most important agents of human disease as well as members of the normal human flora. Some streptococci have been associated mainly with disease in animals, while others have been domesticated and used for the culture of buttermilk, yogurt, and certain cheeses. Those known to cause human disease comprise two broad categories: First are the pyogenic streptococci, including the familiar β-hemolytic streptococci and the pneumococcus. These organisms are not generally part of the normal flora but cause acute, often severe, infections in normal hosts. Second are the more diverse enteric and oral streptococci, which are nearly always part of the normal flora and which are more frequently associated with opportunistic infections.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
35.1 Introduction
The streptococci are a large heterogeneous group of gram-positive spherically shaped bacteria widely distributed in nature. They include some of the most important agents of human disease as well as members of the normal human flora. Some streptococci have been associated mainly with disease in animals, while others have been domesticated and used for the culture of buttermilk, yogurt, and certain cheeses. Those known to cause human disease comprise two broad categories: First are the pyogenic streptococci, including the familiar β-hemolytic streptococci and the pneumococcus. These organisms are not generally part of the normal flora but cause acute, often severe, infections in normal hosts. Second are the more diverse enteric and oral streptococci, which are nearly always part of the normal flora and which are more frequently associated with opportunistic infections.
Measured in terms of mortality, morbidity, and economic costs, five streptococcal species are of major importance in human disease. (1) The group A Streptococcus, Streptococcus pyogenes, produces a wide range of infections, from pharyngitis and impetigo to puerperal sepsis, erysipelas, necrotizing fasciitis, and toxic shock syndrome. Their nonsuppurative sequelae include acute rheumatic fever and acute glomerulonephritis. (2) The group B Streptococcus, Streptococcus agalactiae, is currently a leading cause of sepsis in newborn infants and a frequent cause of postpartum infections in mothers. (3) The pneumococcus, Streptococcus pneumoniae, remains the most frequent cause of bacterial pneumonia in all age groups and is a common agent in otitis media, bacteremia, and meningitis. A detailed account of the pneumococcus may be found in Chapter 29. (4) Among the oral streptococci, Streptococcus mutans is important as a principal agent of dental caries. (5) The Enterococcus is part of the normal bowel flora and has been increasingly isolated as an opportunistic invader, especially in nosocomial infections. Enterococcus is now a separate genus but will be considered an honorary Streptococcus in this chapter because of its similarities to enteric streptococci.
35.2 Historical Background
Streptococcal infections were recognized by Greek physicians by the third century BC. A description of erysipelas is recorded in Epidemicus and attributed to Hippocrates. In the Middle Ages, scarlet fever, or “scarlatina,” as it was called in Italy, was an eye-catching and notable disease. Sydenham’s description in 1676 clearly differentiated this disease from measles and other rashes, but it was not until 1924 that G.F. and G.H. Dick showed conclusively that streptococci were the causative agents. Until the advent of penicillin, childbed fever, or puerperal sepsis, remained one of the most frequent causes of death among otherwise healthy young women. The classic works of Holmes, in 1858, and Semmelweiss, in 1861, described the transmission of this disease and provided guidelines for effective infection control and preventive measures that are still applicable today. Rheumatic fever was first described by Wells in 1812, and Bouillaud described the association of acute rheumatism and heart disease in 1835. In 1836, Bright published his account of “renal disease accompanied with secretion of albuminous urine.”(1) Osler provided detailed descriptions of “malignant scarlet fever,” which remained common until the advent of antibiotics (see Figure 1). Severe invasive diseases, including necrotizing fasciitis, “hemolytic streptococcus gangrene,” and myositis were much less common and did not appear in the medical literature until the second and third decades of this century. During the mid-1970s to 1980s, cases of acute rheumatic fever and acute glomerulonephritis became exceedingly rare (see Figure 2), and streptococcal disease seemed to become only an inconvenience. By the late 1980s, however, rheumatic fever made dramatic reappearance at military posts and in Utah and other areas of the United States.(2,3) There was also a dramatic increase in severe invasive infections and the emergence of a streptococcal toxic shock syndrome.(4) Group A streptococci made the headlines in the popular press as “Killer Strep,” the “flesh-eating bacteria.”

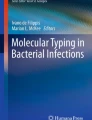
The number of deaths (left-hand scale) from scarlet fever (1900–1960) and from all streptococcal sore throat (1950–1975), with death rates (right-hand scale) per 100,000 population in the United States. Appropriate comparability ratios were applied beginning in 1940, and recorded data compiled according to the geographic locale where the event occurred without regard to residence (1900–1940); resident data were compiled according to the usual place of residence without regard to locale where the event occurred (1940–1975). The population used for determining rates was that of the registration area. Data were not available for streptococcal sore throat for 1900–1950. The number of states reporting for 1900–1905 was 10, gradually increasing to 48 in 1935 and to 50 states in 1960. After 1975, reporting was optional, and no accurate data are available. Sources of data: US Bureau of the Census,(234) National Office of Vital Statistics,(235) Centers for Disease Control.(236) Figure redrawn from Quinn.(1)

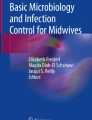
The number of positive throat cultures (left-hand scale) and number of confirmed cases of rheumatic fever and acute glomerulonephritis (right-hand scale) seen in private pediatric practices participating in streptococcal surveillance studies in Rochester, New York, 1967–1988. The data were kindly provided by Caroline Breese Hall, University of Rochester.
In the late 19th century, manyinvestigators contributed to the understanding of streptococci and their relation to human disease. By the 1880s many species had been given names such as Streptococcus epidemicus, Streptococcus erysipelatus, Streptococcus scarlatinae, and Streptococcus rheumaticus, which reflected different manifestations of streptococcal infection. The name S. pyogenes dates from this period but is probably of less descriptive value than the term “Streptococcus haemolyticus,” which was commonly used through the early part of this century. The formal classification of streptococci began when blood agar came into use and the hemolytic properties of various organisms were noted. In 1919, Brown used the term “beta” to describe streptococci that produced a 2- to 4-mm zone of clear hemolysis around colonies grown on blood agar. “Alpha” streptococci were those producing incomplete, greenish, hemolysis. Most of the isolates from severe human disease were β-hemolytic. It was not until 1928, when Lancefield introduced methods of serotyping streptococci based on immunologic reactions with cellular components, that groups and types within groups could be clearly distinguished. The group antigens were eventually shown to be specific cell wall carbohydrates. The group A streptococci were further differentiated by the M and T protein antigens. The β-hemolytic streptococci from most human infections proved to be those of group A. Armed with these new epidemiologic tools, Lancefield and Hare investigated cases of puerperal sepsis at Queen Charlotte’s Hospital in London, beginning in the early 1930s.(5) Of 46 cases of postpartum sepsis, all but oneisolate was group A, and the exception was identified as the prototype of a new serologic group, designated group G. A year earlier, Hare and Colebrook observed that hemolytic streptococci resembling those associated with sepsis were never found in vaginal cultures of healthy women, but that some women carried streptococci that resembled those isolated in bovine mastitis. The latter organisms proved to be members of Streptococcus group B.(5)
By the late 1930s the group B streptococci were recognized as important, if occasional, pathogens causing postpartum sepsis, amnionitis, endocarditis, and septic abortion. The advent of antibiotics, along with better methods for preventing nosocomial spread, resulted in a dramatic decline in streptococcal infections on obstetrical services. At Queen Charlotte’s Hospital there were very few maternal deaths due to either group A or group B streptococci from 1940 to the mid-1960s. In this same period there were few cases of neonatal sepsis or meningitis attributed to streptococci of any kind in large series published in the pediatric literature. It appears unlikely that group B streptococci went simply unrecognized as perinatal pathogens for over 20 years. Rather, there seems to have been a real increase in group B disease, beginning in the United States and Europe during the 1960s. By the mid-1970s, numerous reports of group B disease appeared in the literature, and the group B Streptococcus was said to have come of age.
The pneumococcus has an interesting and important history, beginning with its association with pneumonia in the 1880s and later with developments in immunology, antibiotics, and the discovery of DNA.(6)
The history of S. mutans began in 1924, when Clark first isolated the organism from human dental caries. It was another four decades, however, before Keyes established the “infectious and transmissible nature” of dental caries in animal models and later in human subjects.(7–9) Since dental caries are chronic rather than acute infections and are not directly life-threatening, the global significance of S. mutans has only recently been appreciated. Dental caries, a complex but diagnosable and treatable infection, is perhaps the most common bacterial infection in humans.
Streptococcus suis is an emerging zoonotic microbe contracted by humans having direct contact with pigs and pork products. The first human infections were reported in a series of meningitis cases beginning in 1968.(10) Over the past decade several large outbreaks and over 400 human cases have been reported mainly from Asia and Europe.(11)
The enterococci, as they were called by Thiercelin in 1899, were noted as a major aerobic component of feces. Extremely hardy, they grow in bile, at high or low temperatures, in salt, and at high pH. Although for many years grouped with the streptococci because of morphologic similarities, they were transferred to the genus Enterococcus in 1984 on the basis of genetic studies. These and several new Enterococcus species were clearly distinct from the “nonenterococcal” group D streptococci, Streptococcus bovis and Streptococcus equinus. Enterococci have long been known as an occasional cause of opportunistic infections, but in the early 1970s they began to appear with increasing frequency in reports of urinary tract infection, bacteremia, and pelvic, wound, and surgical infections. Vancomycin-resistant enterococci (VRE) are now among the most common organisms causing nosocomial infections and are difficult to eradicate because of resistance to an increasing number of antibiotics.(12)
35.3 Methodology
35.3.1 Sources of Mortality Data
Until the last decade there have been few reliable sources of mortality data for any of the streptococcal diseases. Cause-of-death coding classifications have been revised about every decade, usually without sufficient details regarding a particular etiologic agent. For example, patients may die of heart failure without rheumatic heart disease being specified; puerperal sepsis may be due to group A or group B streptococci as well as other organisms; pneumococcal pneumonia deaths are frequently counted with those attributed to influenza virus.
35.3.2 Sources of Morbidity Data
The most reliable data on morbidity from streptococcal diseases focus on severe invasive infections from national and regional survey areas in the United States, Canada, Europe, and Australia. The Centers for Disease Control and Prevention (CDC) began a passive nationwide surveillance for invasive group A streptococcal infections in 1993. This was expanded to include 10 large metropolitan and regional areas (about 30 million persons or 10% of the US population) as part of the Active Bacterial Core surveillance (ABCs) program of the Emerging Infections Programs Network.(13) Surveillance of group B streptococcal disease was subsequently added.(14) The ABCs have also facilitated tracking of pneumococcal disease incidence and of drug-resistant pneumococci.(15) In Europe, until recently, an informal questionnaire system has been used to track group B streptococcal disease rates(16) and pneumococcal disease has been assessed mainly by review of published reports from individual countries and localities. These efforts have now evolved into more integrated international programs, including strep-EURO(17) and Pcn-EURO.(18) Some national public health centers publish their own more detailed surveillance data. Of particular interest are reports on invasive groups A, B, C, and G streptococcal infections in Denmark 1999–2002(19) and a 10-year survey of invasive group A streptococcal infections in the Netherlands.(20) There has been little monitoring of enterococcal infections and vancomycin-resistant enterococci except in the United States from reports of hospitals participating in the National Nosocomial Infections Surveillance System.(21)
There are few accurate data on morbidity from noninvasive streptococcal infections. Since 1971, streptococcal sore throat, scarlet fever, and acute rheumatic fever have been reported only optionally to the CDC, which now relies primarily on selected hospital and population surveys. Monitoring of recent outbreaks of rheumatic fever by the CDC has been incomplete, and no mechanism for systematic nationwide reporting has been adopted. The best longitudinal incidence data on rheumatic fever are from Denmark, where meticulous records have been kept for over a 100 years.(22) The global burden of severe disease, including acute rheumatic fever, rheumatic heart disease, acute glomerulonephritis, and invasive disease is at least 18 million cases, with about 1.8 million new cases per year.(23)
35.3.3 Surveys
A considerable number of surveys have been published on diseases caused by various streptococcal species. The most informative have been prospective epidemiologic studies, certain family studies, and surveys of defined populations. These will be reviewed in the description of epidemiologic features of specific diseases in Section 5.1.
35.3.4 Laboratory Diagnosis
The major streptococcal species associated with human disease are listed in Tables 1 and 2, along with selected biological and clinical features. Our grouping of species is more for convenience than for taxonomic purposes, and various bacteriology textbooks will have different schemes, as well as more detailed information on laboratory methods. Recent changes in taxonomy and nomenclature have been reviewed by Facklam(24) and Kohler.(25) The laboratory procedures and the particular approach to identification will of course depend upon whether isolation is for clinical or research purposes and the degree of specificity required.
35.3.4.1 Isolation and Identification.
35.3.4.1.1 Media and Growth Conditions.
Most streptococci grow poorly on ordinary nutrient media but grow quite well on media enriched with blood, brain, or heart infusion, serum, or glucose. Todd–Hewitt broth is an enriched buffered medium that has become a standard liquid medium for most streptococci. In the United States most laboratories use 5% sheep blood agar, whereas in Britain horse blood is generally used. Both give good hemolysis, although with sheep blood it may be necessary to “stab” the agar in the area of inoculation to ensure subsurface growth for the action of oxygen-sensitive hemolysins. While most streptococci grow well in a normal atmosphere, some species, particularly the “Streptococcus milleri” group and the peptostreptococci, do not show good growth or hemolysis without a reduced oxygen atmosphere. Pneumococci prefer to grow in 5% CO2 or in a candle jar. Most streptococci grow best at 35–37°C, although the enterococci will also grow at 10 and 45°C.
Routine isolation of group A streptococci from throat cultures is adequately accomplished using plain sheep blood agar incubated in air at 37°C; cultures read as negative at 18–24 h should be incubated an additional 24 h for optimal sensitivity. Alternatively, throat cultures may be incubated anaerobically, although this may increase the recovery of nongroup A β-hemolytic streptococci. Selective media containing trimethoprim–sulfamethoxazole have also been evaluated and recommended for use in throat cultures.
Many laboratories now process vaginal or anorectal cultures to determine colonization by group B streptococci in pregnant women during the third trimester. A selective broth medium is generally required to minimize overgrowth of other organisms. A Todd–Hewitt broth containing nalidixic acid, polymyxin, and crystal violet has been used in large epidemiologic studies.(26,27) A similar medium is available with colistin plus nalidixic acid but without crystal violet (“Lim” broth).(28) A broth containing gentamicin plus nalidixic acid has also been widely used, although some group B strains may be inhibited by the gentamicin. A satisfactory commercial solid medium is Columbia CNA agar, which contains colistin and nalidixic acid. New Granada medium has the advantage of revealing the orange-pigmentation characteristic of group B streptococci grown in the presence of starch, but a liquid version of this medium has proved unsatisfactory.(29) For isolation of pneumococci from nasopharyngeal carriers a selective blood agar containing 4 mg/l of gentamicin sulfate, Columbia CNA agar, and plain blood agar are usually satisfactory. The enterococci grow on nearly all conventional media, including EMB (eosin–methylene blue) used for gram-negative enteric organisms.
35.3.4.1.2 Colony Morphology and Hemolysis.
The first step in identifying a Streptococcus is examining colonies grown on blood agar for characteristic morphology and hemolysis. A throat culture, for example, will have much extraneous growth, but the bacteriologist will be looking for group A streptococci that have small (0.5–1 mm) opaque white colonies surrounded by a wide zone of clear β-hemolysis. Stabs made into the medium in the area of inoculation will usually clear first because the streptolysin O is more active in the absence of air. Streptolysin S, which is active on the surface, does not always produce complete hemolysis in young cultures. Occasional strains produce large (>1 mm) mucoid colonies, due to the expression of hyaluronic acid capsules (especially M type 18).
Groups A, C, and G streptococci are similar in appearance, but group B streptococci are usually larger, more mucoid, and have a narrower zone of hemolysis that is often less distinct. About 1% of wild group B strains are nonhemolytic, but this depends to some degree on the media used. Some streptococci of the Streptococcus anginosis (“milleri”) group have very tiny colonies but comparatively large zones of β-hemolysis; these may include group F and the “minute colony” groups A, C, and G streptococci.(24) The α-hemolytic streptococci are quite heterogeneous and are difficult to distinguish even to the practiced eye. The pneumococci, however, are usually smooth and glossy with central craters formed by autolysis as the colonies grow beyond 18–24 h. Colonies of type 3 pneumococci are often very large and have a distinctive mucoid appearance. Enterococci have rather buttery colonies, compared to most of the streptococci, and usually produce no hemolysis or may be β-hemolytic on horse blood and α-hemolytic on sheep blood.
35.3.4.1.3 Presumptive Identification.
For practical purposes, group A streptococci can be identified presumptively by the bacitracin sensitivity test of Maxted in which a 0.04-unit bacitracin (TAXOR) disk is placed on a pure subculture of a β-hemolytic Streptococcus. Group A streptococci are extremely sensitive and uniformly show a zone of inhibition, whereas only 5–10% of group C or G strains may give a false-positive result. The simplest of several tests for group B streptococci is the CAMP test (described by Christie, Atkins, and Munch-Petersen in 1944). The test is performed by inoculating a streak of the group B streptococcus perpendicular to a streak of S. aureus on a sheep blood agar plate; an arrowhead-shaped area of complete hemolysis indicates the presence of CAMP factor, which enhances the effect of the staphylococcal β lysin. Streptococci reported simply as “not A or B” on the basis of presumptive tests usually prove to be group C or G. Pneumococci are distinguished from other α-hemolytic streptococci by sensitivity to optochin in a manner similar to that of the bacitracin test for group A streptococci. In addition, the bile solubility test of Neufeld remains useful for separating pneumococci from the occasional optochin-sensitive viridans Streptococcus. Enterococci are identified by growth on bile-esculin media and in 6.5% NaCl. Further identification of these and the viridans streptococci is done with various panels of biochemical tests.
35.3.4.1.4 Rapid Antigen Detection Tests (RADT).
A number of direct antigen detection tests are currently in use for diagnosis of streptococcal pharyngitis. These RADTs yield results in 10–60 min and permit the physician to appropriately treat streptococcal pharyngitis without the delay of conventional cultures. Older latex or particle agglutination tests have good specificity but poor sensitivity. Most newer methods are based upon the extraction of cell wall antigens from throat swabs followed by their detection by enzyme immunoassay (EIA). In general, these tests have excellent specificity (>95%), but the sensitivity is on the order of 80–90%, or even lower, compared to culture. Some optical immunoassays and chemiluminescent DNA probe tests may approach the accuracy of culture. However, there are conflicting results among studies and few that directly compare various methods. For this reason it is recommended that a throat culture be done when the rapid test is negative. Individual laboratories should verify their own test parameters to assess the need for back-up cultures and minimize the risk of false-negative results.(30)
Two problems continue to limit the usefulness of the RSDTs. One is that they detect only group A streptococci, whereas acute pharyngitis is sometimes caused by group C or G streptococci, and these may require antibiotic therapy. The other is cost: A blood agar plate currently costs about $0.25, whereas EIA tests cost about $2.00 each, and optical immunoassays cost somewhat more. Although some RADTs may be waived as “simple” laboratory tests, this may not exempt the physicians laboratory from compliance or certification under the US Federal regulations adopted in the Clinical Laboratory Improvement Act (CLIA).
Particle agglutination methodologies have been employed for detecting group B streptococcal antigens in CSF or urine. Testing of urine samples has been discouraged because the urine sample may be positive as the result of skin or genitourinary contamination, or possibly from intestinal absorption and urinary excretion of antigen.(31) Many laboratories have discontinued antigen testing of CSF because it generally offers no better sensitivity than a properly performed Gram stain. No rapid tests have proved sensitive enough to determine maternal colonization directly from vaginal swabs. However, sensitive PCR test is now coming into use.(32)
35.3.4.1.5 Definitive Identification.
Streptococci are classified into Lancefield groups on the basis of their cell wall carbohydrate antigens. The classical methods of grouping employ an extraction step, usually hot acid (Lancefield method) or nitrous acid, followed by detection of liberated antigens with specific rabbit antisera. More recently, latex and similar particle agglutination kits make it possible for any laboratory to provide rapid and accurate group identification without having to maintain serologic supplies. Molecular methods are now replacing some of the more tedious procedures.
Classic typing of group A streptococci is done by precipitation of M and T proteins with specific antisera, as described by Lancefield in 1928.(5) The M protein is the major antigenic surface marker, and antibodies to its variable N-terminal region are protective both in humans and in mouse protection tests. The T proteins are trypsin-resistant antigens that are not associated with protection but are useful markers for certain M types and for strains having no detectable M protein. T typing is done first by agglutination after trypsinization of the streptococcal cells. M typing is then done on the basis of T typing results, after an acid extraction step and precipitation with specific antisera. For example, T1 strains are invariably M1, and T3 strains are M3, whereas T8/25/Imp.19 strains may be M2, 55, or 57. About 93 M types are internationally recognized, but a quarter or more of isolates are not typeable with either T or M antisera. The major technical difficulties with this system are the difficulty in making antisera and validating new M types by functional protection testis. Testing for many of the less common but established M types cannot be done simply because typing sera are no longer available.(33) One method to overcome these problems is a surrogate typing system based on the neutralization of opacity factor (OF) described by Fraser and Maxted in 1979 and later modified by Johnson and Kaplan.(34) This test is relatively simple and correlates well with M typing. A second surrogate for M typing is “emm typing,” which is based on the DNA sequences of putative M protein genes, described in the next section.
The epidemiologic importance of group A typing is obvious, since certain M types are commonly associated with specific kinds of infection or sequelae. Table 3 lists the most common M types associated with uncomplicated pharyngitis, severe systemic infections, and rheumatic fever, and with acute glomerulonephritis.(35–37) Molecular studies have confirmed these observations and further identified emm-type patterns particularly associated with skin infection.(38) M1 strains are common in both uncomplicated pharyngitis and in severe invasive disease, but epidemiologic evidence suggests that the serious disease is caused by especially virulent strains or clones, and virulence is not always associated as a general property of that serotype.(36) Molecular methods, described below, now confirm such observations and shed light on the evolution of virulent clones and the virulence genes themselves.(39–41)
The typing of group B streptococci is based on the detection of capsular polysaccharides, listed in Table 4. There are four “classical” types: Ia, Ib, II, and III; two newly recognized types of growing importance: IV, V; three new relatively uncommon types: VI, VII, VIII; and a newly proposed type IX.(42,43) In her original description of the type polysaccharides, Lancefield noted that, finding no antigens analogous to the M proteins of group A streptococci, she was looking for capsular materials like those found in the capsules of pneumococci.(5) The group B indeed proved to have capsular polysaccharides, and are all similar in structure, composed of glucose, galactose, and N-acetylglucosamine. Unlike pneumococci, they all have side chains containing terminal sialic acid residues that are major antigenic determinants. There are a large number of surface protein antigens of pathogenic and immunological importance.(44) Type Ib strains, about half of type II and some type III strains also carry the “c protein,” a complex antigen that binds the Fc portion of IgA. The R antigens, which are resistant to trypsin, occur on some type II and III strains but are not frequent among human isolates. The X antigen is found almost exclusively in veterinary strains, particularly those from bovine mastitis.
The pneumococci are classified into about 90 distinct types based on antisera to their capsular polysaccharides. The Danish typing system recognizes 48 main types or groups of closely related types. (Each of these corresponds to an individual type of the American system, which is no longer in common use.) For example, types 1–5 each contain only one distinct type. Group 6 includes type 6A (America type 6) and type 6B (American type 26) and a recently identified type 6C.(45) Knowledge of the distribution of types in human infections led directly to the selection of the most important types in the formulation of pneumococcal vaccines.
Group D and viridans streptococci are usually speciated by their pattern of biochemical reactions. Various test kits and automated equipment are in general use in most clinical laboratories and give basically similar results. However, these products do not always conform to the latest taxonomic changes. Two major identification schemes are currently in use, one from Great Britain, the other from the CDC in the United States. They differ mainly in the classification of group F and the S. anginosis (“milleri”) group. This group currently consists of three species: S. anginosis, Streptococcus constellatus, and Streptococcus intermedius, which differ in their production of β-glucosidase, hyaluronidase, and several other glycosidases.(24) A group of organisms formerly described as “nutritionally deficient streptococci” have been reclassified into two new genera, Abiotrophia and Granulaticella, on the basis of 16S ribosomal RNA similarities.(24) These organisms are noteworthy as a cause endocarditis.(46) Streptococcus mutans is divided into eight serologic types based on cell wall carbohydrates, but epidemiologic studies now favor molecular methods for distinguishing strains among types.(8)
Most enterococci share a glycerol teichoic acid antigen with the group D streptococci. However, enterococci are usually characterized by their ability to grow in broth containing 6.5% NaCl and hydrolyze esculin in the presence of 40% bile salts (bile-esculin medium), and a positive PYR reaction. Strains are divided into five major groups and 33 species mainly on the basis of biochemical tests. Enterococcus faecalis is distinguished from Enterococcus faecium by growth in the presence of tellurite, reduction of tetrazolium, and fermentation of sorbitol.(25,47)
35.3.4.1.6 Molecular Methods.
Molecular methods have now been applied to various streptococcal species for direct detection, identification, epidemiology, and studies of molecular evolution. Although it is unlikely that the polymerase chain reaction (PCR) will ever completely replace the blood agar plate, hybridization with labeled gene probes has been successfully employed for detection of group A streptococci from throat swabs of patients with pharyngitis.(48) A rapid PCR test has been developed for detection of group B streptococcal colonization directly from swabs in pregnant women.(32) Pneumococcal DNA in materials such as blood cultures and middle ear fluids has also been demonstrated by PCR, using primers derived from known nucleotide sequences from genes coding for autolysin or pneumolysin.(49)
Molecular identification of group A streptococci M protein genes, called emm typing, has now essentially replaced classical serologic M typing.(50,51) This method is based on DNA sequencing of the N-terminal end of the gene, which codes for the highly variable antigenic portion of the M protein generally detected by specific antisera. In addition to the 93 classically validated M types, 110 officially designated emm types have been described, along with many more provision types and subtypes. The CDC maintains a dedicated, curated web site and searchable database of validated emm types, provisional types, and subtypes (http://www.cdc.gov/ncidod/biotech/strep/strepindex.htm). This has been especially useful for epidemiological tracking of otherwise nontypeable strains. It also has the advantage that emm types can be identified in isolates that express only small amounts of M protein and are only weakly antigenic in conventional M typing.(33) Nevertheless, the emm typing is not without its own set of difficulties. Many strains have several emm or M protein-like genes that may look like M protein genes but code for proteins with lectin-like functions, such as binding of immunoglobulins or fibronectin, and some appear to be extra copies or even defective genes. The amplification and/or detection of these genes may depend greatly upon the selection of primers and the conditions of the assay.
Several other molecular approaches differentiate among streptococcal strains or types but are not necessarily intended to correlate with given M or T typing systems. “Ribotyping” is based on the pattern of amplified ribosomal RNA in agarose gel electrophoresis or by automated systems. Depending upon the primers utilized, species-specific and sometimes strain-specific identification may be possible. Because ribosomal RNA nucleotide sequences are highly conserved, few differences may be seen even between strains of differing M types.(52) Restriction fragment length polymorphism (RFLP) relies upon endonucleases, such as SmaI or SfiI, that cut DNA at relatively fewer sites, producing longer more distinctively sized fragments. These large (20–500 kb) fragments must be resolved using pulse field gel electrophoresis, hence the more familiar name, PFGE. PFGE has proved useful in a wide variety of epidemiological studies.(53) Various methods similar to those just described have been employed for epidemiological studies of group B(54) and group G(55) streptococci, pneumococci,(56) and enterococci.(57,58) Molecular methods have also focused on genes of particular interest because of their function in disease, antibiotic susceptibility, or epidemiology. Two highly pathogenic clones of group A Streptococcus were tracked and delineated by the allelic variants of their scarlet fever toxin (SPE-A), serotyping, and multilocus enzyme electrophoresis (MLEE).(59)
Two new molecular typing methods have come to the fore over the past decade: MLST—multilocus sequence typing and MLVA—multilocus variable-number tandem repeat analysis. MLST was proposed in 1998 as a universal definitive and portable method characterizing bacteria.(60) Selected internal fragments of about 500 bp in length are amplified from seven different “housekeeping” genes, which are relatively stable genetic markers. The sequence of each locus is assigned a different number, whether it represents a single point mutation or a large recombinatorial replacement. MLST methods are in use for group A Streptococcus,(61) group B Streptococcus,(62) S. pneumoniae,(63) S. suis,(64) and E. faecium.(65) These techniques have been used to track clonal spread of group A streptococci resistant to multiple antibiotics,(53) to characterize nontypeable group B streptococci,(66) to study the population biology of pneumococci,(67) and to assess both nosocomial(58) and global spread(57) of vancomycin-resistant enterococci.
MLVA methods depend on PCR amplification of selected gene segments that contain a variable number of short repeated sequences. These segments vary among isolates and yield gene products of different lengths that can be separated by electrophoresis on agarose gels. The banding patterns (done individually or in a multiplex) are highly reproducible and most systems have powers of resolution equal to that of MLST. MLVA is generally cheaper, much easier to perform, but more suitable for short-term outbreak investigations than for long-term population studies, compared to MLST. In some systems each allele associated with given locus is assigned a number corresponding to the number of tandem repeats, thus giving a numerical repeat profile that can be compared without reference to the gel pattern itself.(68) MLVA methods have been applied to pneumococci,(69) E. faecalis,(68) and E. faecium.(70) However, the current MLVA typing scheme for E. faecium was found to be somewhat less discriminatory than MLST and PFGE for hospital studies.(71)
35.3.4.2 Serologic and Immunologic Diagnostic Methods.
Antibody tests have been developed as clinical and epidemiologic tools in the study of group A, group B, and pneumococcal infections. In general, antibodies are markers of past experience with the organisms and do not indicate when an infection took place. For this reason they are most useful when acute and convalescent antibody levels are compared in relation to an episode of presumed infection.
Assays for the group A Streptococcus are based on the development of antibodies either to cellular antigens or to extracellular enzymes. These are listed in Table 5 and further described in Section 4. Tests for antibody to M proteins, which confer immunity, and to the group A carbohydrate have been used primarily for research purposes. Assays used clinically for confirmation of recent infections have been reviewed by Shet and Kaplan.(72) The antistreptolysin O (ASO) is the most reliable and is widely available. It is of no immediate value in the diagnosis of acute streptococcal pharyngitis, and it should not be expected to differentiate carriage from infection. Nevertheless, about 80% of patients with rheumatic fever or pharyngitis-associated acute glomerulonephritis infection will mount a significant ASO response. A rise in titer is usually seen 3–6 weeks after infection, and a rise, even if modest, is more helpful than a single determination. Test kits give a titer of >166 Todd units as elevated for adults, but there is considerable variation in the “normal” values among populations and laboratories. In general, single ASO titers above 250 in adults and above 300 in school-aged children are considered elevated. Compared to pharyngitis, skin infections tend to elicit feeble ASO responses but greater responses to DNase B. The anti-DNase B titer peaks later, at 6–8 weeks after either skin or throat infections. This test is often useful when the initial ASO is low or negative. There is less clinical experience with the anti-hyaluronidase and anti-streptokinase tests, although they may give comparable results and may be useful as confirmatory tests. The Streptozyme® hemagglutination test (Wampole Laboratories, Stamford, CT) is a crude screening test based on reactions with a mixture of streptococcal antigens, including streptolysin O, DNase, NADase, streptokinase, and hyaluronidase. It is simple and widely available but is not considered sufficiently reliable by many authorities. Positive responses appear earlier (1–2 weeks) and should always be confirmed with one or more of the standardized assays whenever rheumatic fever or acute glomerulonephritis is suspected.(30)
Assays for antibody to pneumococcal and group B streptococcal capsular polysaccharides have employed radioimmunoassay (RIA) for total antibody and enzyme-linked immunosorbent assays (ELISA) for total and class-specific antibody determinations. Since both pneumococci and group B streptococci have multiple capsular types, antibody to specific types must be considered. Although it has so far proved impossible to establish an absolute or minimal protective antibody level, infection appears to be more common in subjects with low antibody levels against the specific capsular antigen of the type causing infection. Assays for type-specific pneumococcal antibodies are now commercially available.
35.4 Biological Characteristics of the Organisms
The various streptococcal species have many biologic similarities and differences. The genus name suggests a “twisted chain,” which describes the microscopic appearance of many species, especially when grown in broth culture. The pneumococci are commonly described (and were formerly named) as diplococci because of their propensity to occur in pairs, but they are often indistinguishable from other streptococci in blood cultures. All the streptococci have a tough cell wall composed of cross-linked peptidoglycans. Most have a polysaccharide group antigen associated with the cell wall, and some have teichoic acids as major or additional components. Pneumococci exhibit prototypic bacterial polysaccharide capsules. The group A streptococci, in contrast, have the M proteins on their exterior surface, but these appear to play a similar role in helping the organisms resist phagocytosis. The group B streptococci, like pneumococci, have polysaccharide capsules as their major surface antigens. Pneumococci, however, also have autolytic enzymes that break down cell walls in late growth phases, releasing DNA and other intracellular components. Intact pneumococci also take up genetic material and are thus auto-transformable, a characteristic that appears to have facilitated the spread of antibiotic resistance within the species. With few exceptions, streptococci are aerobic and facultatively anaerobic. They are cytochrome-negative, catalase-negative, and ferment sugars mainly to lactic acid but not to gas. All streptococci secrete enzymes extracellularly, but those of group A have been studied most extensively.
35.4.1 Cellular Antigens and Enzymes
35.4.1.1 Group A Streptococcal Cellular Antigens and Enzymes.
The major components of group A streptococci are the cellular antigens and the extracellular enzymes listed in Table 5. M proteins, noted above and listed in Table 3, are important virulence factors of group A streptococci, contributing to the organism’s resistance to phagocytosis in the absence of type-specific antibody.(73) M proteins bind host proteins, especially fibrinogen, as a ploy to evade host defense mechanisms. Although immunity appears to be lifelong, most humans are usually infected by only a few different types and remain susceptible to the other types. Thus, repeated episodes of streptococcal infection may be due to different types rather than to a failure of host response. Certain M types, especially M1 and M3, have been associated with more severe forms of disease, and some are more common in pyoderma and acute glomerulonephritis(4,36) (see Table 3). Others have historically been associated with acute rheumatic fever and are referred to as “rheumatogenic” types. Although rheumatogenicity is not determined by M type alone, evidence for the cross-reactivity of certain M proteins with heart and brain tissue strongly suggests autoimmune mechanisms for the etiology of acute rheumatic fever and Sydenham’s chorea.(74,75)
The group A cell wall carbohydrate is a polymer of rhamnose with N-acetylglucosamine side chains. Humans normally make antibodies to this antigen but the role of antibodies has been controversial. There is now evidence that this antigen may play a role in sequelae of streptococcal infections by inducing antibodies cross-reactive with cytokeratin.(75) This could provide an explanation for the joint and skin manifestation of acute rheumatic fever and of guttate psoriasis. Vaccinating mice with group A carbohydrate cross-linked to tetanus toxoid appears to induce antibodies that are protective against challenge with group A streptococci.(76)
Hyaluronic acid capsules are produced by some (especially M18) strains, giving colonies a large highly mucoid appearance. This capsule material is indistinguishable from the ground substance of mammalian connective tissue and is not immunogenic. Its effect on virulence in mice is small, although similar capsules may occur on group C streptococci and have greater virulence than unencapsulated strains. Nevertheless, mucoid group A strains have been associated with severe disease in humans and with rheumatic fever.(36,74) Furthermore, the near-disappearance of acute rheumatic fever in the United States may be correlated with the replacement of rheumatogenic M types by nonrheumatogenic types in cases of pharyngitis.(77)
Lipoteichoic acids are composed of polyglycerophosphate attached to lipids. These surface molecules are directly involved in attachment of organisms to host epithelia and are of importance in the initiation of infection.(78) Other cellular components are less well defined in terms of their role in disease. As in other gram-positive bacteria, there is a rigid cell wall structure made from polymers of alternating glucosamine and muramic acid units cross-linked by peptide side chains. This serves to stabilize the organisms against outside osmotic changes. The peptidoglycan components are highly inflammatory and may play a role in inciting nonspecific host responses. The T proteins, noted above, occur in families that may be shared by a number of M types. The serum opacity factor proteins are coexpressed with specific M types and are not shared among M types.(34) The R antigen is an antigenic surface protein that occurs in strains of various types but appears to play no role in virulence or protection. Like groups C and G streptococci, group A and other streptococci also have antibody-binding proteins that bind antibodies nonspecifically via the Fc fragment, presumably to help the organism avoid specific, complement-fixing, antibody binding.(79)
Group A streptococci secrete various substances into the surrounding milieu that may contribute to the pathogenic process. There are two well-described hemolysins capable of lysing red blood cells and injuring other cell membranes and subcellular organelles.(80) Streptolysin O is the antigenic, oxygen-labile hemolysin used in the ASO test. Streptolysin O is a pore-forming toxin that facilitates the entry of NADase and presumably other toxins into cells.(81) Streptolysin S is nonantigenic, oxygen stable, and is responsible for β-hemolysis at the surface of cultures grown on blood agar under aerobic conditions. This hemolysin acts as an epithelial cell toxin and also impairs phagocytic clearance of the organisms.(82)
Deoxyribonucleases (DNases) are elaborated by groups A, B, C, and G streptococci. DNase B is the most common and most immunogenic of the group A DNases and is the basis of the antibody test of the same name. It is thought that these enzymes along with hyaluronidase and streptokinase combine to produce the thin pus seen in streptococcal infections, in contrast to the thick pus often associated with infections due to other pyogenic bacteria.(1) The pathogenic role of DNases now appears to be aid in evasion of innate host defense mechanisms.(83)
Streptococcal hyaluronidases (produced by groups A and C) are capable of hydrolyzing the hyaluronic acid of group A capsules and of mammalian connective tissue. Although formerly called “spreading factor,” its biologic role remains uncertain with regard either to cell metabolism or to the production of disease. It appears that hyaluronidase does facilitate spread of large molecules but not bacteria in the area of infection, but its major role may be to enable the organism to utilize hyaluronic acid as a carbon source.(84)
The streptokinases are antigenic proteins that convert plasminogen to plasmin, which in turn lyses fibrin clots. Group A streptococci produce either streptokinase A, the most common, or streptokinase B. An antibody test based on the former antigen is sometimes employed in the clinical assessment of group A disease. A distinctive low-molecular-weight streptokinase, called “nephritis strain-associated protein,” has also been identified from group A streptococci recovered from patients with acute nephritis.(85)
Nicotinamide adenine dinucleotidase (NADase; also called diphosphopyridine nucleotidase, DPNase) is produced by streptococci of groups A, C, and G. Anti-NADase antibodies are produced by the majority of patients recovering from group A streptococcal pharyngitis, but responses are poor following skin infections. NADase is toxic to leukocytes but requires pores formed by streptolysin O in order to enter cells and enhances the virulence of the organisms in vivo.(81) Recent studies have found NADase production in all strains of group A streptococci isolated from invasive cases and have demonstrated that the current expression of NADase in M-1 strains correlated with the temporal emergence of M-1 strains associated with invasive disease around 1985.(86)
Several proteinases of group A streptococci have been carefully studied and shown to exert pathologic effects in vitro and in vivo. A specialized peptidase has been described that diminishes chemotactic activity by inactivation of the C5a complement component. Streptococcus pyogenes exotoxin B (SpeB) is a cysteine protease that cleaves the hinge region of human IgG and has other immunomodulating properties.(87)
Streptococcal pyrogenic exotoxins (SPEs) are the erythrogenic toxins responsible for the characteristic rash of scarlet fever. These enzymes have been implicated as factors in streptococcal toxic shock, where they appear to be potent activators of tumor necrosis factor (TNF) and other cytokines.(4,88) There are three classic antigenically distinct toxins, designated SPE A, B, and C. All group A streptococci carry a gene (speB) that codes for SPE B, but it is not understood why some strains are stronger producers of the toxin than others. SPE A and SPE C are encoded by lysogenic bacteriophages, and only those strains infected by the phages are capable of producing toxin. Humans make antibodies to SPE A, B, and C, which appear to confer toxin-specific immunity to scarlet fever. It is possible to have scarlet fever more than once, due to different toxins. A large family of SPEs (so far SPE D–M) have now been identified with various pyrogenic, mitogenic, and superantigen properties.(89) The classic determination of susceptibility to scarlet fever is the Dick test.(1) Seldom used today, it is based on the observation that patients with antibody to a specific toxin show no response to a small intradermal injection of that toxin (negative Dick test). Susceptible individuals, who have no antibody to neutralize the toxin, develop inflammation at the injection site within 24 h (positive Dick test). SPE A shares structural and physiologic similarities with TSST-1, one of the toxins associated with staphylococcal toxic shock syndrome (see also Section 7.1).
35.4.1.2 Group B Streptococcal Cellular Antigens and Enzymes.
The group B streptococci differ from group A in that their virulence may be accounted principally by capsular polysaccharides rather than proteins. The capsular types, noted in Section 3.4.1 and in Table 4, are antigenically distinct by virtue of variations in linkages of the same essential sugars. A key feature is that all have terminal N-acetylneuraminic acid (sialic acid) residues that are major immunodeterminants. The capsules are antiphagocytic and require specific antibody for efficient opsonization. The quantity of sialic acid-containing antigen appears to be directly related to size and density of the capsule and to virulence in animal models.(90,91) The capsular material itself appears to inhibit the activation and chemotactic functions of neutrophils.(92) Many group B strains are also capable of binding fibrinogen to their surface in a manner that competes with the nonspecific binding of C3 complement.(87,92)
The group B antigen is a complex glucitol-containing polysaccharide associated with the peptidoglycan cell wall. Antibodies to the group B antigen are generally not protective, presumably because it is covered by capsular material. A human monoclonal IgM antibody to the group B antigen has been described that opsonizes strains of all serotypes,(93) but the large amount of antibody required appears to make impractical as an adjunctive therapeutic agent.
The major surface structures and protein antigen of group B streptococci have been reviewed by Lindahl and colleagues.(44) The major protein to be studied was the c protein, which occurs on all type Ib and some type II and III strains. Antibodies to this antigen are protective,(94) but common variants of the protein apparently confer resistance to intracellular killing by neutrophils. An important property of the beta c protein may be its ability to nonspecifically bind human IgA.(92) The alpha c protein is involved with adherence to epithelial cells via a glycosaminoglycan-binding region and mediates entry in host cells.(95) The R and X antigens are rarely seen in human isolates and probably play no role in protection or disease. Also present are lipoteichoic acids (LTA) that resemble the lipopolysaccharides (LPS) of gram-negative bacteria and engage the Toll-like receptors (TLR-2) of the innate defense system.(96)
The group B streptococci elaborate a number of extracellular enzymes, including hemolysins, CAMP factor, DNases, and “neuraminidase.” Pritchard et al. have shown that the enzyme thought for many years to be a “neuraminidase” is in fact a hyaluronic acid lyase that has a unique mechanism of action quite unlike that of hyaluronidases produced by group A streptococci or pneumococci.(97) Group B streptococci have several hemolysins, one of which has been identified as cytotoxic for mammalian cells in vitro and inhibited by phospholipids common to pulmonary surfactants.(80) The CAMP factor potentiates the activity of staphylococcal sphingomyelinase in vitro but is not essential for systemic virulence.(98) Like group A, group B streptococci elaborate a proteinase that decreases chemotactic activity by specifically cleaving complement C5a.(44,99) A pyrogenic exotoxin has also been identified from strains associated with a group B streptococcal toxic shock-like syndrome in infants.(100)
35.4.1.3 Pneumococcal Cellular Antigens and Enzymes.
Streptococcus pneumoniae is the paradigm of encapsulated bacteria. Its polysaccharide capsules are essential to virulence and antibodies against the capsule are the major specific defense against infection. The 90 recognized type-specific polysaccharides vary in composition, including linear polymers, branched chains, and teichoic acid-like antigens. The most frequently occurring types have been selected for inclusion in the presently licensed vaccines.(101)
The C-polysaccharide corresponds to the group carbohydrates of other streptococci but differs significantly in structure. Its major antigenic determinant is phosphocholine, linked to ribitol phosphate, galactosamine, and other sugars. Although humans make “natural” antibodies to this antigen, opsonization of pneumococci (and presumably protection) is almost entirely dependent upon anticapsular antibodies.(102) The Forssman antigen is a membrane teichoic acid similar to C-polysaccharide but linked to a lipid, forming what is essentially the lipoteichoic acid of the pneumococcus.
Pneumococcal surface protein A (PspA) has been identified on essentially all important clinical isolates and appears to play an important role in virulence. Humans including young infants make antibodies to PspA and to various other surface proteins, suggesting their use in a vaccine.(103) Enzymes produced by pneumococci include pneumolysin, amidase (the autolytic enzyme that breaks down cell wall material), neuraminidases, and IgA proteases. Pneumolysin is a pore-forming toxin that bears extensive amino acid sequence homology to streptolysin O and to the theta-toxin of Clostridium perfringens. It is highly toxic to pulmonary epithelial cells and may be important to the pathogenesis of pneumonia.(101)
35.4.1.4 Components of Other Streptococci.
Other pyogenic streptococci share many characteristics noted above. All have rigid peptidoglycan cell walls, with various distinctive or group antigens, and usually with some form of lipoteichoic acid. Group C streptococci may have hyaluronic acid capsules like those of group A. Group G streptococci may have the type 12 M protein of group A or similar surface proteins, as well as antibody-binding proteins. The group C streptococci from human, equine, and porcine sources produce species-specific streptokinases that are otherwise similar to those of group A.(104) A streptokinase derived from group C has been used clinically in attempts to clear clotted intravascular catheters, to lyse pleural adhesions in patients with lung infections, and to help remove clots in patients with coronary artery occlusions. Group G streptococci also produce streptokinases. We have described a patient with nephritis following infection with a group G strain that had a low-molecular-weight enzyme similar to the nephritis strain-associated protein of group A.(105)
The enteric and oral streptococci are usually unencapsulated. Some in the S. anginosis (milleri) group appear to have capsules more often when found in abscesses, and the capsules play a role in protection from phagocytosis.(106) Few toxins or noxious enzymes have been described among the enteric and oral streptococci, but this may be from lack of concerted investigation. Members of the S. anginosis group have, at the least, hyaluronidase, deoxyribonuclease, and various proteinases.(24,106) For many of the less virulent streptococci, the inflammatory response to infection probably relates more to the properties of the cell wall breakdown products than to specific enzymes or toxins. Characteristics that enable them to cause disease often relate to their ability to adhere to host tissues, such as tooth enamel, heart valves or prostheses, or to intravascular catheters. Streptococcus mutans, for example, adheres to the pellicle coating the tooth surface by specific protein receptors called antigen I/II; adhesion is further facilitated by the presence of sucrose. Streptococcus mutans also produce extracellular proteases that are capable of breaking down cemental collagens and other host substrates. Caries occur when the secretion of acids demineralizes the enamel and organisms adhere to and invade the tooth surface. Streptococcus mutans also produce mutacins, bacteriocin-like antibiotic peptides, that help protect their ecological niche in dental biofilm.(9,107) Enterococci and S. anginosis group streptococci are frequently found in mixed infections, especially in association with anaerobic bacteria, suggesting that additional factors are required for them to cause disease. Enterococci produce several pheromones that are chemotactic for neutrophils and may contribute to the inflammation associated with infection. Enterococcus faecalis also produces a plasmid-encoded hemolysin. Because enterococci are frequently resistant to common antibiotics, serious enterococcal disease also occurs as superinfection in patients receiving broad-spectrum antibiotics that may disturb the normal ecology of this usually benign organism.(12)
35.4.2 Antibiotic Susceptibility
The streptococci are generally quite susceptible to penicillin, including most oral and S. anginosis group streptococci. Exceptions include some pneumococci and group D streptococci, and the enterococci. Although streptococci are generally resistant to aminoglycosides, gentamicin is sometimes used for its synergistic effect in combination with a penicillin, particularly in patients with endocarditis due to viridans streptococci and enterococci.(108) Chloramphenicol has occasionally been used in penicillin-allergic patients, but other drugs, including erythromycin, clarithromycin, and clindamycin, are considered to be superior for most streptococcal species.
Groups A and B streptococci have never developed resistance to penicillins, probably because they are not naturally transformable, as are pneumococci and enterococci. They are somewhat less sensitive to vancomycin and cephalosporins, moderately resistant to chloramphenicol, and fairly resistant to aminoglycosides, sulfonamides, and tetracycline. Group B strains have shown some tolerance to penicillin, but the clinical significance of such observations is unknown. Tolerance to penicillin has also been suggested as one mechanism by which group A streptococci persist after treatment of pharyngitis. But although there may be a modest increase in efficacy of cephalosporins compared to penicillin, the explanation appears to be the more efficient eradication of the carrier state in patients whose pharyngitis was actually due to viral causes.(109,110) Another mechanism is thought to be the protection of susceptible streptococci by the production of β-lactamases by other bacteria in the pharynx or tonsils,(111) although this concept has been disputed.(112) Another explanation is that the streptococci penetrate the epithelial cells where they may persist even in the presence of extracellular penicillin.(113) Resistance to erythromycin occurs in about 5% of group A strains in the United States and most other parts of the world. However, local rates from 25 to 50% have been reported in Korea, Italy, and Pittsburgh, Pennsylvania. Resistance rates parallel antibiotic use and may be reduced by improving prescribing practices.(114,115)
Penicillin resistance in pneumococci has emerged slowly over the past two decades and has now become a frequent and serious problem worldwide. Most of these strains have intermediate susceptibility (MIC 0.1–1.0 μg/ml) but highly resistant strains (MIC >1.0 μg/ml), initially reported from South Africa and Spain, have now spread throughout Europe and North America. The widespread use of fluoroquinolones, macrolides, and azithromycin has led to increased resistance to those drugs in many areas.(116) Of considerable concern is the recent emergence of strains with very high resistance to penicillin and of multiresistant serotype 19A strains, because they are not included in the 7-valent conjugate vaccine (which contains type 19F).(117)
Although group B streptococci remain sensitive to penicillin, some strains can be penicillin tolerant, which has been speculated as a cause of treatment failure in cases of invasive disease.(118) Another problem is the increasing resistance to erythromycin and clindamycin, which are used as alternatives to penicillin in antibiotic prophylaxis for allergic women.(27) Resistance mechanisms to macrolides and clindamycin have been identified as methylase genes erm(B) and erm(TR) and efflux genes mef(E) and mef(A).(119)
Enterococci are moderately resistant to penicillins alone, because of the intrinsic properties of their penicillin-binding proteins. Enterococcus strains with resistance to β-lactam antibiotics and high-level resistance to aminoglycosides began to appear in the 1980s. Some strains of E. faecalis have also acquired β-lactamases as a mechanism of resistance.(120) Infections are usually treated with penicillin or ampicillin plus an aminoglycoside, which exert a synergistic effect against the organisms. Vancomycin-resistant enterococci (VRE), especially E. faecalis, made their appearance in the late 1980s and have been an increasing problem ever since.(57,121) Vancomycin acts by binding to the d-alanine–d-alanine on the end of cell wall muramic acid precursors. Resistance conferred by a plasmid or transposon carrying the vanA or similar gene, allows the organism to generate muramic acid precursors with peptides ending in d-alanine–d-lactate, to which the vancomycin has low affinity. VRE present difficult therapeutic challenges, because there are few alternatives to vancomycin.(12,57) Most VRE are E. faecium, which is sensitive to quinupristin–dalfopristin, but E. faecalis is resistant. Linezolid is effective against both species, but as more linezolid is being used, resistance has started to appear.(58)
35.5 Descriptive Epidemiology
35.5.1 Prevalence and Incidence
Group A streptococcal pharyngitis is one of the most common acute bacterial infections. The frequency of this disease, especially as manifested by scarlet fever, has declined dramatically since the beginning of the century, as illustrated in Figure 1.(1) The severity of the disease, reflected by mortality rates, declined concomitantly. This trend began long before the advent of antibiotics, suggesting a decrease in virulence or an increase in host resistance, or both. In the 1940s penicillin became widely available, and deaths attributed to scarlet fever and puerperal sepsis, the two most common lethal forms of group A streptococcal disease, became a rarity. The number of reported cases of streptococcal sore throat increased during the 1950s and 1960s, probably because of increased physician awareness of its relation to rheumatic fever, greater use of throat cultures, and the availability of antibiotics for treatment and prevention. Since the 1960s only one population-based study of streptococcal sore throat in an industrialized country has been published, a prospective study of 202 Australian families with at least one child in the 3- to 12-year age group.(122) The incidence of culture-positive cases was 13 per 100 child-years and was eight per 100 child-years for serologically confirmed group A streptococcal infection. This was similar to previous studies in suburban populations, but rates were about half that seen in crowded lower socioeconomic settings and lower still that in present day indigenous populations.(122)
Figure 2 shows the number of positive throat cultures and number of cases of acute rheumatic fever and acute glomerulonephritis in private pediatric practices participating in surveillance studies in Rochester, New York, over a 20-year period. These data were compiled and kindly supplied by Caroline Breese Hall, University of Rochester. Of approximately 23,000 throat cultures done annually, 18–25% were positive for group A streptococci in this relatively stable population. Meanwhile, the number of cases of acute glomerulonephritis declined from nearly 40 in 1967 to an average of one case per year from 1981 to 1988. Confirmed cases of acute rheumatic fever dropped from 20 to 28 per year to a very few from 1975 to 1985 and have continued to be very low. For example in Baltimore, between 1960 and 1964, the incidence of rheumatic fever was 26 per 100,000 among 5- to 19-year olds. By 1980 the rates had fallen to 0.2–0.8 per 100,000 nationwide among whites, but with rates several times higher among other ethnic groups. Beginning in the mid-1980s, an increase in new rheumatic fever cases was seen in Utah, Pennsylvania, Ohio, New York, and other areas. Disease incidence peaked in Utah in 1985 with 18 per 100,000 population age adjusted for 5- to 17-year olds,(3) and rates peaked again in 1998 and have subsequently declined.(123) Of particular interest was the observation that throughout this period incidence rates were essentially unchanged in Hawaii and New Zealand, where the disease is especially prevalent among Polynesian children. The explanation may be the local prevalence of certain rheumatogenic M protein types many of which were characteristically mucoid, whereas in other areas of the United States these have been largely replaced by nonrheumatogenic types.(77,123)
There has not been a similar decline in rheumatic heart disease in the developing world.(23) In a program begun in 1984 the WHO Cardiovascular Disease Unit surveyed 16 developing countries and found rates averaging 220 cases per 100,000 childhood population. Highest rates were in Africa and the eastern Mediterranean, lowest rates were in Southeast Asia and the Western Pacific. More recent data have found that prevalence rates of clinically diagnosed rheumatic heart disease have not changed in Cambodia in 2001–2002 (220/100,000) and Mozambique in 2005 (230/100,000). However, echocardiographic screening for mitral or aortic regurgitation revealed that 10 times as many children were affected.(124) The major problem in the developing world is establishing and maintaining effective primary and secondary prevention programs.(125) This principle applies as well to developed areas, such as Miami, Florida, where underprivileged inner-city children have attack rates of 15/100,000, compared to 0.7/100,000 for suburban middle-class children.(126)
Deaths from acute rheumatic fever are uncommon today. In developed countries deaths associated with chronic rheumatic heart disease continue to occur in persons who had acute rheumatic fever in childhood and develop severe mitral stenosis in the fourth decade or later. In 1975, for example, 9255 of 12,775 deaths attributed to rheumatic heart disease were in patients over 50 years of age.(1) The pattern is quite different in developing areas, as in South Africa, where a third of patients have mitral regurgitation usually associated with ongoing rheumatic activity.(127) Left untreated these lesions develop into a severe form of pure mitral regurgitation that requires surgery in the first or second decade of life. Degenerative valvular disease, including mitral stenosis and mixed lesions, is like those seen elsewhere but tends to occur at a younger age.
Another change in group A streptococcal disease in recent years has been the reappearance of serious acute infections, especially bacteremia and streptococcal toxic shock.(4) Since 1980, the number of invasive disease and deaths has increased in several countries. However, the rates in various population-based surveys differ depending upon whether disease was defined as toxic shock, necrotizing fasciitis, or all invasive disease. Surveillance in Ontario, Canada, revealed that the incidence of necrotizing fasciitis (NF) increased from 0.08 cases per 100,000 population in 1992 to 0.49 cases per 100,000 population in 1995, with a case-fatality rate of 13%.(128) In the Netherlands, 1994–2003, annual incidence of all invasive disease peaked in 1996 (4.0 cases/100,000/year) and was at its lowest in 1999 (2.0 cases/100,000/year).(20) Similar rates were noted from Israel.(129) In the United States 5,400 cases of invasive GAS infection (3.5 cases per 100,000 persons) were identified in 2000–2004, with 735 deaths (case-fatality rate, 13.7%). Case-fatality rates for streptococcal toxic shock syndrome were 36 and 24% for necrotizing fasciitis. Rates were highest among elderly persons (9.4 cases per 100,000), infants (5.3 cases per 100,000), and black persons (4.7 cases per 100,000) and were stable over time.(13) Chickenpox has been a major risk factor for invasive disease in children, but cases have declined since the introduction of the varicella vaccine in 1995.(130) Severe invasive infections due to group A, B, C, and G streptococci were reviewed in Denmark from 1999 to 2002. Group A infections occurred at a rate of 2–3/100,000 persons/year. Of particular note was that group G infections rose, mainly among the elderly, from 1 to 2/100,000 during the observation period. Septic shock and toxic shock syndromes were seen in group B, C, and G infections, although not as frequently as with group A streptococci.(19)
Acute poststreptococcal glomerulonephritis is currently a rare disease, as shown in data from Rochester, New York, in Figure 2. There are no contemporary data on rates for nephritis associated with either throat or skin infections in the United States, and no recent reviews. Prospective studies in Alabama (1966–1969) revealed 91 cases of nephritis relative to 1,149 cases of uncomplicated streptococcal pyoderma treated in a clinical setting, for an attack rate of about 8%.(35) Of note, however, is that outbreaks of glomerulonephritis associated with group C streptococci continue to occur, usually in association with unpasteurized dairy products.(131,132)
Group B streptococci emerged in the 1970s as the leading cause of neonatal infection. In the 1980s attack rates of early-onset disease were about 2 per 1,000 live births in defined populations in Chicago, Illinois, and Birmingham, Alabama.(26,133) Several clinical trials demonstrated the potential for prevention of early-onset disease by selective intrapartum antibiotic prophylaxis, which led to the first guidelines issued in 1996 by the CDC, the American College of Obstetricians and Gynecologists (ACOG), and the American Academy of Pediatrics (AAP). Two selection strategies were used: One (ACOG) relied of identification of clinical risk factors, such as prematurity, maternal fever, and prolonged rupture of amniotic membranes. The other (AAP) was based on screening women for vaginal/rectal colonization by group B streptococcal at 35–37 weeks of gestation. Those with colonization and/or risk factors were offered penicillin given intravenously during labor. This resulted in a 65% decrease in early-onset cases to about 0.5 per 1,000 live births from 1993 to 1998, where they remained unchanged through 2001. Meanwhile, further studies in the Active Bacterial Core Surveillance program found that routine antenatal screening prevented significantly more infections than the risk-based strategy.(134) Revised guidelines and updated prophylaxis regimens were published in 2002.(28) Since that time, rates of early-onset disease have declined and additional 31% to 0.34 per 1,000 live births.(14) Rates among African-Americans have seen the largest decline but are still about twice that in the White population. Early-onset disease rates in Europe vary from 0.3 to 2/1,000 live births, and several countries have prevention guidelines.(16) Clinical studies in France and Italy have found similar reductions in attack rates using a combined culture and risk strategy.(135) Experience using a risk-only prevention in the Netherlands has resulted in only modest reductions from 0.54 to 0.36 cases/1,000 live births, and changes in guidelines have been recommended.(136) Early-onset disease rates are about 2/1,000 live births in South Africa and 0.9/1,000 in Malawi, but prevention strategies are difficult to apply in resource-limited settings.(137)
Late-onset disease, generally defined as occurring in infants older than 7 days, has remained unchanged for over a decade, with rates in the United States about 0.4/1,000 live births.(14) Prematurity is the major risk factor in late-onset disease, occurring in 50% or more of cases.(14,138) Rates are about the same in northern Italy (0.5/1,000 live births),(139) but higher in South Africa and Malawi (about 1/1,000 live births),(137) and considerably lower in the Netherlands (0.14/1,000 live births).(136)
Few data are available on maternal infections due to group B streptococci, such as bacteremia, chorioamnionitis, endometritis, and urinary tract infection. Maternal sepsis occurred in 0.5–2/1,000 deliveries in Alabama, with lowest rates associated with aggressive antibiotic use in mothers undergoing Cesarean section delivery.(140) Rates of chorioamnionitis and endometritis have declined since the introduction of intrapartum prophylaxis.(141)
Group B streptococcal infections in nonpregnant adults have increased between twofold and fourfold over the past two decades.(142) While still occurring at rates of a few per 100,000 population among young and middle-aged adults, those over 65 years are especially vulnerable, with rates of 25/100,000. Predisposing factors, such as diabetes mellitus, malignancy, and residence in nursing homes, are common. Infections of skin and soft tissue, urinary tract, and pneumonia predominate.(143)
Enterococci have been most notable in hospital settings, where endemic infection and outbreaks are common.(121) Vancomycin-resistant enterococci (VRE) now account for about 28% of nosocomial infections.(21) In a study of 24,000 blood culture recorded in 49 US hospitals, 1995–2002, enterococci were found in 9% of nosocomial blood stream infections (about 5/10,000 hospital admissions). The majority of blood isolates were E. faecium, of which 60% were VRE.(144) In the only population-based study of invasive VRE, in metropolitan Atlanta, Georgia, disease incidence increased from 0.9/100,000 persons/year in 1997 to 1.7/100,000 persons/year in 2000.(145) Enterococcus faecium accounted for over 80% of isolates, followed by E. faecalis, and a few Enterococcus gallinarum and Enterococcus durans. The crude 30-day in-hospital mortality was 40% and was best predicted by three factors: the Charlson comorbidity index, immunocompromise from chemotherapy, and prior antibiotic use. African American patients had a higher mortality rate, attributed largely to higher rates of chronic conditions, especially end-stage renal disease.
In terms of sheer numbers of persons, dental caries caused principally by the mutans streptococci, S. mutans, Streptococcus sobrinus and their relatives, probably infects more people than all other streptococci combined. However, the last 40 years of the 20th century saw a remarkable decline in dental caries worldwide, beginning in western Europe and North America.(146) Rates of DMFT (decayed, missing, or filled teeth) were commonly 10/100 surfaces at risk in the 1960s have come down to around 1/100 surfaces by 1988 and have remained relatively stable. The major decline in caries has been attributed mainly to fluoridation programs, fluoride-containing dentifrices, and school dental services. By the mid-1980s about half of school-aged children in the United States and Canadian children had permanent teeth completely free of cavities and restorations.(147) Some of these good news and further reductions in DMFT rates to 1/100 surfaces and below can be ascribed to the introduction of tooth sealants, general improvements in dental care, and changes in parental beliefs and attitudes.(148,149)
Survey methodology for measurement of dental caries is well established and periodically revised.(150,151) Since the populations of developing countries are skewed toward the younger age groups, who have fewer caries relative to the older populations in the developed world, a population-weighted mean DFMT at age 12 is used for global comparisons. By this measure WHO can monitor trends from more than 1,000 surveys submitted to the WHO Global Oral Data Bank, set up in 1970. Some developing countries have seen a rise in DFMT thought to be associated with changes in diet and other factors associated with urbanization.(150) In the absence of fluoridation and adequate dental care, increased sugar consumption may also play a role.(152) Most caries and DMFT data from the developing world now come from regional or national survey or from compilations of published reports.(153)
With the decline in caries incidence in many countries DFMT data may be somewhat less useful, especially for clinical intervention trials, in which individual counts of new decayed, missing, and filled surfaces (DMFS) over a defined period may be better indicators. The decline in caries has also had an impact on the number of patients required for statistical power in clinical studies.(154) Newer models focus on the evaluation of caries risk, such as Cariogram, a software program that evaluates an individual’s caries risk profile and illustrates it in graphic form. The predictive variable which makes the greatest contribution to the model is S. mutans count, followed by the DMFT index and the buffer capacity of the saliva.(155)
35.5.2 Epidemiology and Contagiousness
Of all the streptococcal infections only scarlet fever has been feared as an epidemic disease in the same sense as cholera and plague. In most areas of the world, group A streptococcal disease is endemic, with fluctuations exceeding the normal prevalence levels occurring seasonally or sometimes over an extended period. Localized epidemics of streptococcal pharyngitis or skin infections and acute rheumatic fever are occasionally reported from newborn nurseries, hospitals, nursing homes, day care facilities, and military installations.(156,157) An unusual nursery epidemic occurred when infants were infected from clothing that was improperly cleaned in a hospital laundry.(158) Environmental contamination is thought to be a source of spread within day care facilities, with several studies showing streptococci recovered from environmental surfaces, fabrics, and toys shared by many of the children. A large outbreak of perianal infection prompted a careful investigation that revealed a particular group A streptococcal clone associated with an attack rate of 2–7 per 1,000 children per year in a small rural community in Denmark.(159) Although several urban myths have circulated about contracting streptococcal sore throat from the family dog, household pets are an unlikely source of group A streptococcal infection.(160)
Streptococci associated primarily with the respiratory tract, such as group A and the pneumococcus, cause infections that are initially related to that portal of entry. Of course, some group A strains prefer to colonize the skin and cause impetigo, whereas others affect either skin or throat. The group B streptococci, in contrast, are gut organisms. Asymptomatic gastrointestinal, and to a lesser extent genitourinary, colonization is common. Their infections relate to the aberrations induced by pregnancy, labor, and delivery, and to the unique conditions of infants in the newborn period. The enterococci are also normal gut organisms, but their infections are more generally opportunistic in nature.
Group A streptococci are not considered part of the normal flora of the respiratory tract, and their presence is generally associated with overt infection. Transmission to other persons is greatest from an infected individual, and communicability appears to be dose related. Nevertheless, a large reservoir of asymptomatic carriers, mainly children, exists with endemic rather than epidemic characteristics.(122) Individuals identified as carriers harbor relatively small numbers of organisms. They are at little risk for developing acute disease or sequelae themselves, and they are an uncommon source of new infection.(161) However, the identification of the carrier state, usually defined by the absence of a serologic response, is fraught with difficulties that continue to cloud the relationship between colonization and disease.
Group B streptococci cause serious disease in the perinatal period, but only a small number of infections occur among colonized mothers and infants exposed in utero, during, or after delivery. Maternal group B infections may be initially subclinical and possibly contribute to premature labor or septic abortion.(162) Amnionitis may be present before the onset of fever or other symptoms. After delivery, a previously asymptomatic mother may develop endometritis, usually without bacteremia. Classical puerperal sepsis due to group A streptococci, in contrast, was often transmitted via obstetric personnel and occurred as a fulminant infection after delivery, sparing the infant. With group B streptococci, infected infants are usually exposed in utero to the serotype carried by the mother. Infants with this “early-onset” form of infection are usually bacteremic at delivery and become symptomatic within a few hours of birth.(26,163) Infection is directly related to the size of the inoculum to which the infant is exposed, by swallowing or aspirating infected amniotic fluid. Most infants are lightly colonized and at little risk for infection, whereas those who are infected are almost invariably heavily colonized at birth. Some infants may acquire organisms via the respiratory tract during transit through the birth canal, or from persons other than the mother, and become symptomatic at a later time. Development of the late-onset form of disease may be delayed for days or weeks, and only about half of these infants will be infected by an organism acquired at birth or from the mother.(26,138)
Pneumococci are often thought of as normal respiratory flora, but pneumococcal infections are not opportunistic in the sense that they are caused by any pneumococcus that happens to reside in the nasopharynx. Most infections are due to new types not previously carried by a given individual. This was first observed in the classical investigations of Hodges and MacLeod on pneumonia at a United States Air Force training facility in the 1940s.(164) Within about 6 weeks of arrival, new recruits often acquired one of a small number of “epidemic” types (1, 2, 4, 5, 7, and 12) prevalent at the base. Although the rate of carriage of the epidemic types was relatively low, the “infectivity factor” (measured by the ratio of cases of pneumonia to the number of carriers) was much higher than that of other types commonly carried. Similarly, infants in our prospective study frequently carried one of several common types for prolonged periods, but when they develop otitis media it was usually within 4 weeks of acquiring a type they had not carried previously.(165) This epidemiologic relationship has been nicely confirmed in the Finnish Otitis Media Cohort Study.(166)
The concept of dental caries as a transmissible infectious disease was drawn from animal studies in the 1960s. Streptococcus mutans has been implicated as a major pathogen in caries, and it appears that most infants acquire S. mutans strains from their mother.(7,107) These observations have been confirmed using molecular methods in a prospective studies of acquisition and infection.(8,107) They further developed evidence for a discrete “window of infectivity” between 18 and 30 months of age, coinciding with the emergence of the 20 primary teeth. Children who did not acquire S. mutans during this period were at much lower risk for caries, at least through 6 years of age. To develop stable colonization S. mutans requires nonshedding tooth surfaces over a period of time. Children generally harbor several S. mutans genotypes, with a tendency to form stable colonization by strains transmitted from the mother.(107) Based on epidemiologic evidence from caries prevalence surveys, it is postulated that a second window of infectivity may exist coincident with the emergence of permanent teeth between 6 and 12 years of age.
Streptococcus suis is an emerging zoonotic pathogen found in pigs raised in suboptimal conditions. It affects humans who have direct contact with pigs and pork, with little evidence for person-to-person spread among humans. In three outbreaks in China, in 1998, 1999, and 2005, over 200 people were infected, and 53 died. Nearly three quarters of cases reported have been from China, Thailand, and the Netherlands.(11)
35.5.3 Geographic Distribution
Streptococcal diseases are of worldwide importance. Group A streptococci appear to be well adapted to humans living in temperate or tropical climates, although differences in the temporal distribution and perhaps the characteristics of disease may vary. In some tropical areas, groups C and G streptococci are more frequently isolated in cases of pharyngitis than are group A strains. As noted above, group B streptococcal carriage is widespread, but infection rates are highest in North America and western Europe, with lowest rates reported from the United Kingdom, northern Europe, and parts of Asia. Pneumococci are the leading cause of bacterial respiratory infection in all parts of the world. In some areas, such as sub-Saharan Africa where seasonal epidemics of meningococcal disease are common, pneumococcal disease remains endemic and accounts for many cases of meningitis throughout the course of the year.
Dental caries occur worldwide. Although caries have been more common in industrialized areas than in developing countries,(150) recent international comparisons have been encouraging, with about 50% of children caries free across 17 countries surveyed.(148) Sweets and sugary drinks continue to play a modest role, but the most important factor now is seen to be parental beliefs and attitudes (the “Brushing Parental Efficacy Factor”) that promotes earlier and better supervision of tooth brushing and dental care.(148) Although this has been attributed in part to the higher use of sucrose and refined foodstuffs and social changes associated with urbanization, the major factors remain lack of dental care. The incidence of caries is mitigated to some extent by the availability of artificial fluoridation in dentifrices and water supplies.(152) Caries have always been less common in geographical areas with natural fluoridation.
35.5.4 Temporal Distribution
Group A streptococcal infections follow characteristic seasonal patterns. In northern parts of the United States streptococcal pharyngitis is typically seen over the winter months, peaking in February or March, while skin infections occur mainly in the summer. Figure 3 illustrates this pattern in surveillance data from private pediatric practices in Rochester, New York, for the 12 years 1977–1988. In the southeastern states there is both a late fall and a late winter peak of respiratory infection, coinciding with the beginning of school in the fall and with increased indoor activity or crowding during colder months. Seasonal variation is less evident in tropical or subtropical areas, although gathering of children at school or other institutions appears to increase the incidence of disease at certain times of the year. Streptococcal skin infections are most common in the rainy season in tropical areas. Such conditions favor the exposure of unprotected skin to the assault of minor trauma and the bites of mosquitoes and other insects. Organisms present on the skin surface, or rarely from the respiratory tract, may be inoculated into damaged skin by itching or scratching.

The number of cases of scarlet fever (solid lines) and streptococcal impetigo (dotted lines) seen monthly in private pediatric practices participating in streptococcal surveillance studies in Rochester, New York, 1977–1988. The data were kindly provided by Caroline Breese Hall, University of Rochester.
In temperate climates pneumococcal infections tend to peak in winter months. The disease incidence is not related to the carriage rate, which varies only slightly over the year, but parallels the markedly seasonal rate of acquisition of new strains.(165) In the study of Hodges and MacLeod there was also a strong correlation of pneumococcal lobar pneumonia with the seasonal peaks of influenza virus infection.(164) Present day findings suggest that the association with influenza is rather weak, although a stronger association may be noted for respiratory syncytial virus.(167) In the “meningitis belt” of Africa pneumococcal meningitis epidemics usually occur along with meningococcal epidemic season, beginning with the dry weather in February–March. This seasonal pattern is not understood but may involve increase indoor crowding because of the weather and also change in the respiratory mucosa in response to severe drying.(168)
35.5.5 Age
Group A streptococcal pharyngitis is uncommon in children under 4 years of age. It increases in frequency as children enter school, peaking at 9–12 years of age. These children are the primary source of respiratory infections that occur among families and are thus a source of exposure for parents and other adults in the household. Streptococcal impetigo, in contrast, is chiefly a disease of younger children. It is frequently seen in toddlers and children under 4 and typically reaches a peak incidence at about 6 years of age. Adolescents tend to be subject to milder and often self-limited disease.(122,169)
Group B streptococcal remains a common cause of sepsis and meningitis in neonates and infants up to about 3 months of age.(14) Prematurity is the major risk factor in late-onset disease.(138) Group B streptococci are a common though sometimes disregarded cause of urinary tract infection among adult women, especially during pregnancy, and are an important cause of perinatal and postpartum infection.(162) This has been associated with late abortions and problems of the perinatal period. Rarely does an older child or adult develop a serious infection in the absence of some compromise of normal host defenses. Older adults, however, account for as much as 40% of all group B streptococcal infections. Most common are cases of cellulitis or pressure sores, urinary tract infection, bacteremia, and pneumonia. These are often associated underlying conditions, especially diabetes mellitus, nursing home residence, cardiac disease, and malignancy.(143)
Pneumococcal disease is seen in all age groups, but principally affects the very young and the very old. Among children, 70% of meningitis and bacteremia occur in those under 24 months of age, peaking at 8–12 months of age. The introduction of a 7-valent conjugate vaccine in 2000 resulted in a 60% reduction in invasive disease with the largest decline in infants <12 months of age.(170) The incidence of bacteremic infections increases sharply with age over 55 years, and the case-fatality rate in this group is over 80%. A welcome indirect effect of the 7-valent pediatric vaccine has been the reduction of pneumococcal disease among adults over age 65.(15,171)
Serious infections by enteric and oral streptococci are less subject to the effects of age than to the natural defenses of the host. Low-birth weight babies are increasingly infected by group D and viridans streptococci and enterococci, perhaps because of the kinds of interventions required for the management of very premature infants or changes in patterns of antibiotic use. Nosocomial infection caused by enterococci spans the range of age, but is most common among older hospitalized adults.(12)
Dental caries is a chronic disease that continues throughout life.(149) Longitudinal studies from diverse localities show that rates of development of new caries are about the same in adults as they are in children, although older adults are more likely to get root caries and gum disease. However, as noted in Section 5.2, there appears to be an age-specific window of acquisition of S. mutans at 18–30 months of age that correlates with subsequent risk of caries development.(8)
35.5.6 Sex
Sex is not a factor in the development of streptococcal disease, except as it relates to pregnancy and to specific genitourinary infections, especially those caused by group B streptococci.(162) These organisms may be transmitted by close, intimate, or sexual contact, but genital colonization is not associated with symptoms in either sex.(172) Colonization may be higher in women during the first half of the menstrual cycle, perhaps because of greater adherence to vaginal epithelial cells at this time. The peptostreptococci are recognized in pelvic inflammatory disease but are rarely encountered (or looked for) elsewhere.
35.5.7 Race and Genetic Factors
No one is spared from susceptibility to streptococcal infections. Much of the association between race and susceptibility can probably be accounted for extrinsic factors, such as poverty, crowding, and lack of medical care. Nevertheless, there is growing evidence that certain persons within racial groups may have some genetic host predisposition. Studies of histocompatibility leukocyte antigen (HLA) distributions point to increased risk of rheumatic fever for blacks expressing the DR2 phenotype and for whites with the DR4 phenotype.(75) Agammaglobulinemia and IgG subclass deficiencies are associated with recurrent pneumococcal infection. Various complement deficiencies, especially that of the second component (C2), should also be considered in children with repeated pneumococcal disease. Children and adults with sickle cell disease are at increased risk because of functional asplenia, which develops after repeated episodes of splenic infarction. Down’s syndrome and cleft palate are associated with increased frequency of otitis media due to pneumococci and other organisms.
35.5.8 Occupation
Occupation is rarely a factor in the development of group A streptococcal infections. Physicians, nurses, and laboratory workers in close contact with infected patients or their cultures seldom develop disease. Epidemics of skin infections have occasionally appeared in meat packers, and foodborne.(132,173) Group B streptococci are a major cause of mastitis in cattle. Spread is thought to occur mainly via the hands of dairy workers from human or bovine sources. Molecular studies suggest that at least two lineages of strains from bovine mastitis are very closely related to some isolates causing human disease.(174) Consumers of raw infected milk may become colonized with group B streptococci but do not appear to be at risk for disease. Groups A and C streptococcal diseases have occasionally been associated with milk-borne transmission.(132) Group C infections have also been associated with exposure to horses and other animals. Workers in the pork industry occasionally develop meningitis due to S. suis, as noted above.(11) Streptococcus iniea, a common fish pathogen, has been associated with infections in workers at a fish farm and others handling or cooking fish.(132)
35.5.9 Other Settings and Predisposing Factors
Family studies of respiratory bacteria have indicated that the group A streptococcus and the pneumococcus enter a family unit most commonly via the school-aged children.(122) These organisms spread rather slowly to other family members, some becoming colonized and very few developing overt infection. Spread is often facilitated by concomitant viral respiratory infections. Socioeconomic factors, crowding, and substandard housing have frequently been cited as contributing to the spread of these organisms and to the development of acute rheumatic fever and bronchopneumonia. Schools, day care centers, nursing homes, and long-term care facilities may experience periodic problems with group A streptococci.(175) Spread of pneumococci generally occurs slowly with little consequence in day care centers, but occasional outbreaks of serious disease have been reported in child care and nursing home settings.(176)
The military has been associated for over a century with increased risk for developing streptococcal disease, especially acute rheumatic fever and pneumonia.(164,177) Our present understanding of the epidemiology of rheumatic fever and methods for antibiotic prophylaxis date from important studies done in the US Armed Forces during and after World War II. Rates of streptococcal pharyngitis are much lower in recruit camps where penicillin prophylaxis was routinely used. In one report, however, antibiotic prophylaxis was not effective until penicillin-allergic recruits, who continued to harbor streptococci, were given oral erythromycin.(178)
Nosocomial spread of groups A and B streptococci continues to be reported, especially from obstetric and surgical services and newborn nurseries.(142,156) Sources of infection may be other patients or personnel who carry organisms in the nose, throat, skin, vagina, or anus. Enterococcal infections in neonates and surgical patients usually originate from the patient’s own flora, under the influence of physical interventions and antibiotic therapy.(12,58,121) Intraabdominal wounds, burns, intravascular catheters, and the urinary tract are the most frequent sites associated with nosocomial enterococcal bacteremia. Pneumococci are important but infrequent causes of nosocomial outbreaks.(176)
Predisposing host factors may be genetic or acquired, such as sickle cell disease, immunodeficiency, or splenectomy. Splenectomized patients have a 50- to 200-fold greater risk of serious bacteremic infection.(179) Surgical repair, rather than removal, of a traumatized spleen is frequently possible and always preferred to removal. Overall, about a fourth of children with pneumococcal bacteremia or meningitis have some underlying condition or host defense abnormality, and risk for these children persists well beyond 24 months of age. Patients with human immunodeficiency virus (HIV) infection or acquired immunodeficiency syndrome (AIDS) are at particularly high risk of bacteremic pneumococcal infection.(180) Intravenous drug abuse, also a known AIDS risk factor, is associated with an increase in group G streptococcal infection.
35.6 Mechanisms and Routes of Transmission
The transmission of streptococci, introduced in Section 5.2, depends on factors such as the usual ecologic niche of the species, its occurrence as part of the normal flora, and the ease with which it may be carried by hands, in secretions, or possibly in droplets. The group A streptococci are transmitted principally by direct contact. Contagiousness is greatest during acute respiratory infection, whereas the chronic carrier is a relatively low risk as an infectious source. This probably reflects the fact that development of infection requires a fairly large inoculum. About 100 organisms are required to infect adult volunteers by directly inoculating the tonsils and pharynx with organisms on a cotton swab. Although streptococci may occur in droplets and survive in dust, an individual is unlikely to acquire a large enough inoculum to become infected from these sources. Streptococci recovered from contaminated blankets and dust may also be less infective. Direct transmission of respiratory secretions may occur via hands, person-to-person contact such as kissing, or projection of large droplets during coughing or sneezing. Treatment of infected persons eliminates the risk of spread within 24 h, permitting resumption of work or school activities as soon as constitutional symptoms have abated.(181)
Pneumococci are thought to be transmitted by similar routes.(182) Coughing is a more regular feature of pneumonia than it is of other pneumococcal infections or of streptococcal pharyngitis. Transmission appears to be favored by symptoms of cold and coryza. Dust particles may harbor pneumococci but do not play a significant role in transmission.(164) Direct spread of secretions containing viable organisms is the most likely source. Covering one’s mouth with a hand may deflect a cough or sneeze, but the hand may then transmit fresh secretions.
Large milk-associated epidemics of group A streptococcal disease such as occurred in early in the last century have now been essentially eliminated by the widespread adoption of pasteurization.(132) Small outbreaks of group A and C infections continue to be seen with contaminated prepared foods, such as egg salad, or with cheese and dairy products from cows or goats.(131,132) Despite the prevalence of group B streptococci in bovine mastitis, milk-borne group B infections have not been reported. However, some virulent group B strains appear to be genetically related to lineages of bovine origin.(174)
Skin infections due to group A streptococci are often caused by serotypes different from those associated with throat infections (see Table 3). Similarly, certain corresponding emm types are markers for strains with a strong preference for skin infection.(38,75) Streptococci may occur on normal skin but do not cause infection unless there is a break in the cutaneous epithelium. Minor injuries such as scratches, abrasions, cuts, or insect bites may become points of entry. Mosquito bites are an especially common site of inoculation, where organisms are rubbed into the wound during itching. In Trinidad, streptococcal impetigo may be transmitted by flies of the genus Hippelates, which feed on open skin sores. Streptococci from the nasopharynx may be transmitted to skin sites, but it is more common for the skin to be colonized first and the throat later. Classical erysipelas, in contrast, is thought to be transmitted via the respiratory tract, either from the patient or from a caretaker. Erysipelas is occasionally seen following superinfection of chicken pox lesions.
The group B streptococci causing early-onset perinatal infections are those carried by the mother in the lower gastrointestinal and genitourinary tracts. Organisms may enter the amniotic cavity following rupture of amniotic membranes, but the fetus may become infected with membranes intact. Although rupture of membranes for greater than 12 h is a recognized risk factor for ascending infection, the duration of labor is also important, perhaps because of the entry of organisms via microscopic defects in the membranes. Among twins, who have a higher rate of infection than singletons, it is usually the first twin who is closer to the source of infection and at greater risk. Once the streptococci have entered the amniotic fluid, they proliferate rapidly and are aspirated or swallowed by the fetus. Late-onset infections may have a maternal source in about half of cases, with colonization occurring at delivery.(26,138) Other infants may acquire streptococci later from persons outside the immediate family, presumably via the oral or respiratory route. Late-onset and recurrent infections have also been transmitted by mother’s milk in cases with mastitis, asymptomatic colonization, or banked breast milk.(183)
Oral streptococci are part of the normal flora and are acquired early in life from the mother and family members.(7,8,107) Enteric streptococci generally cause opportunistic infection only after perturbations of normal defenses. Nosocomial infections are usually due to a patient’s own flora. Transient bacteremia may occur with dental manipulation, transurethral prostate resection, or gynecologic and gastrointestinal surgery. Patients with known history of valvular heart disease or artificial heart valves are at higher risk for developing endocarditis due to otherwise “benign” streptococcal species. In such cases a prophylactic antibiotic is administered just prior to the dental or surgical treatment (see Section 9.2). Enterococcal infections may be similarly opportunistic or nosocomial in origin.(12)
35.7 Pathogenesis and Immunity
35.7.1 Pathogenesis
The development of infection involves a multitude of interrelated bacterial and host factors that vary enormously among streptococcal species. The biologic characteristics associated with virulence among various streptococci are summarized in Section 4; certain host factors and modes of transmission are noted in Sections 5.9 and 6. The pathogenic process is not clearly understood for any streptococcal disease, but it may be useful to consider three general stages.
First, organisms are acquired by the host and either succeed in colonizing their preferred sites or are eliminated by host defenses at the epithelial surface. For many streptococcal species the specific mechanisms of adherence are known.(75,78,92,184) Adherence may be important in the establishment of colonization but is not necessarily a property that distinguishes virulent from commensal species or strains. To ward off bacterial invasion the host has epithelial barriers, mucus layers, and secretions containing enzymes and antibodies.
The second stage begins when organisms succeed in breaching local defenses and enter the epithelial and subepithelial tissues, or in the case of S. mutans get into and through the tooth enamel.(75,92,184) Most of the acute pathologic effects of group A streptococci occur at this stage by causing pharyngitis or skin infection, with invasion of the submucosal or subepidermal layers. This is frequently accompanied by lymphadenitis but rarely progresses to bacteremia. In pneumococcal pneumonia and in otitis media the initial insult is not a direct breach of epithelium but rather the invasion of a normally sterile compartment; symptoms of disease ensue as organisms multiply and induce inflammation in surrounding tissue. The host responds with nonspecific secretory and serum forces, including the release of vasoactive and chemotactic mediators, activation of the alternative complement pathway, and with the mobilization of neutrophils and tissue macrophages. Eventually, specific secretory and serum antibodies develop and contribute to resolution of the disease.
The third stage is systemic infection, in which organisms multiply in blood and tissues. Severe streptococcal infections, including streptococcal toxic shock, depend upon the organism’s ability to evade host defenses until it establishes a sufficient mass of growth to cause systemic manifestations. The M proteins protect against phagocytosis and also down-regulate complement activation on the bacterial surface.(73) C-5 peptidase is an enzyme that inactivates complement C5a and decreases chemotaxis and secondary inflammatory responses.(87) Spread of infection within the tissues may be facilitated by the action of hyaluronidase and proteinases. Shock is probably mediated by tumor necrosis factor-α (TNFα), interleukin (IL)-1β, and IL-6, all of which may be induced by pyrogenic toxins (SPE), streptolysin O, and cell wall breakdown products. Further alterations in host physiology occur by cytokine activation and by direct and indirect effects on hemodynamics, metabolism, and the function of individual organs.(4,185,186)
Similar mechanisms are involved in acute group B streptococcal sepsis.(92,187) Early-onset infections usually begin in utero, and it is suspected that the organisms gain access to the circulation by breaching the gastrointestinal or pulmonary epithelial barriers. The organisms may be actively taken up by pulmonary alveolar cells acting as nonprofessional phagocytes, which are incapable of killing the organisms preventing tissue invasion. Alternatively, the organisms can cross the epithelial barriers by transient openings in the cell junctions.(188) Group B streptococci also have mechanisms to evade the inflammatory responses of the host, including the antiphagocytic properties of the polysaccharide capsules, a C5a inactivating enzyme similar to that of group A streptococci, and the c protein, which binds IgA in a nonimmune fashion. The early manifestations of severe disease depend upon the inflammatory responses mediated by both specific and innate host defense factors. Group B streptococcal surface structures and breakdown products, especially cell wall peptidoglycan, interact directly with macrophages and monocytes promoting release of proinflammatory cytokines. Cell wall activates C3 complement via the alternative pathway, and both peptidoglycan and lipoteichoic acid (LTA) interact with components of the Toll-like receptor (TLR) system, which in turn promotes cytokine responses. Tissue damage due to hemolysins and other toxins further the inflammatory response. While the initial inflammatory response is often minimal in infants, despite the presence of bacteria in the lung or other tissue, localized, overexuberant responses in the central nervous system appear to play a major role in disturbing the blood–brain barrier, opening the way to development of meningitis.(92,187)
The most severe infections, particularly streptococcal toxic shock syndrome, have all the elements of invasive disease, and in addition have the effects of streptococcal superantigens.(75,89,185,186) These include streptococcal pyogenic exotoxins (SPE) A, B, C, F (mitogenic factor), G, H, J, and are much like the staphylococcal toxic shock toxin (TSST-1) and staphylococcal exotoxins SE A–E and H. The absence of neutralizing antibodies to these toxins is associated with increased risk of severe disease.(189) Superantigens are a family of protein toxins that activate the immune system by binding directly to both the MHC class II molecules of antigen-presenting cells and the Vβ T-cell receptor, causing nonspecific activation of up to 30% of the entire T-cell population. This in turn causes massive release of cytokines, including TNFα, interferon-γ, IL-2, and IL-6. More T and B cells are recruited to the site of infection, resulting in further release of IL-1, TNFα, and other mediators. The triggering of an overexuberant host response is thought to play a large role in hypotension, disseminated coagulopathy, and multiorgan failure seen in toxic shock syndrome.
The pathogenesis of the nonsuppurative sequelae of group A infections has yet to be fully elucidated. Examples of the cross-reactivity between M proteins and components of heart, brain, and connective tissue have now been convincingly confirmed and add weight to the long-held hypotheses of autoimmune mechanisms for rheumatic valvular disease, Sydenham’s chorea, and skin manifestations.(75) Although multiple complex factors appear to be involved in disease process, these and other studies have identified M protein epitopes that cross-react with myosin, DNA, and α-helically coiled proteins such as tropomyosin, actin, and keratin. Antigenic mimicry between cell wall carbohydrate moieties and cytokeratin may eventually help explain the occurrence of erythema marginatum, subcutaneous nodules, rheumatic arthritis, and perhaps streptococcal-associated guttate psoriasis. The diverse manifestations of acute rheumatic fever might be explained in part by the specificity and titer of antibodies cross-reactive with different tissue components. In a similar fashion, acute glomerulonephritis may involve the development of antibodies that cross-react with basement membrane collagen and laminin.(75) The cationic charge of the antigens may also influence their affinity for the glomerular basement membrane and the nature of immune complexes formed. Another feature of nephritogenic streptococci is the presence of a nephritis strain-associated protein.(85) This distinctive low-molecular-weight streptokinase is a plasminogen activator and could induce proliferation of cells, release of inflammatory products, and activate complement, thus contributing to known pathologic features of the disease.
The pathogenesis of dental diseases has been described as “examples of ecological catastrophes.”(190) Caries development involves dynamic relationships among dental plaque organisms, dietary carbohydrates, and mucosal host defenses. Fermentable carbohydrates, especially sucrose, favor the adherence of mutans streptococci to the tooth surface by several different mechanisms, including glucan-binding and salivary-binding proteins. Streptococcus mutans, together with Streptococcus sobrinis, lactobacilli, and other bacteria form biofilms on the tooth surface. The biofilms have an extracellular water-insoluble carbohydrate matrix which helps stabilize and protect the bacterial colonies and concentrate acids from fermentation, which in turn lower the pH, and aid in demineralization of tooth enamel. This process is countered by the host by the buffering capacity of saliva and defensive components, such as lysozyme, lactoferrin, and secretory IgA. Specific antibodies to S. mutans surface proteins can inhibit sucrose-dependent adherence and interfere with biofilm formation.(107,184)
35.7.2 Immunity
Specific immunity to streptococcal infections is thought to depend on the development of antibodies to capsular and other surface determinants. Antibody assays for various streptococcal antigens have been noted in Section 3.4.2, and current developments in streptococcal vaccines are further discussed in Section 9.6. Although most of our knowledge of the immune response relates to the occurrence of antibodies in the serum, recent studies of mucosal immunity suggest that the first line of host defenses are at the local level. The precise role of secretory antibodies in preventing, modifying, or eradicating bacterial colonization is not presently understood. Conversely, the effects of bacterial antigens at respiratory and gastrointestinal sites are poorly understood in regard to the systemic antibody response and the development of autoantibodies. In some cases it is likely that the organisms have developed a form of mimicry to confuse or evade the immune response of the host. Many streptococci have antigens that cross-react with other organisms, common foodstuffs, or components of the host’s own tissue. Antibodies undoubtedly have functions other than protection against disease. They are known to be important in the recovery from established infection and probably function in the removal of antigens from local and systemic sites.
Assays for group A streptococcal antibodies (Table 5) are used clinically to determine if a patient has had a recent infection.(72) Although humans normally make antibodies to streptolysin O and other extracellular components, only antibodies to M proteins are associated with protection against subsequent disease.(73,75,185) Serum IgG antibodies to M proteins arise in response to infection or immunization and can initiate bactericidal activity in whole blood opsonophagocytic assays. These antibodies, however, are not as efficient as secretory IgA antibodies in protecting mice against infection via the intranasal route. Intranasal immunization of volunteers with purified M protein resulted in greater resistance to colonization with live streptococci than did subcutaneous immunization, and serum antibody response was not a reliable predictor of resistance to pharyngitis. At present, group A vaccines remain experimental, but it appears that local immune mechanisms may be more efficiently utilized and less likely to result in systemic side effects.
Antibodies to the capsular polysaccharides of group B streptococci are thought to mediate protection against systemic invasion. This concept is based on the finding that few infants with group B streptococcal disease have antibodies to the offending type, and that antibodies are protective against bacterial challenge in animal models.(191) Naturally occurring antibodies in mothers are often of the IgM class and do not readily cross the placenta, and less IgG antibody is transferred to the premature than to the term fetus. Protective levels of IgG seem to vary with serotype, and protection increases as fetuses receive more maternal IgG at > 34 weeks gestation. In a prospective study of infection levels have been empirically estimated to be ≥5 μg/ml for type Ia and ≥10 μg/ml for type III.(192,193) Despite the presumed importance of antibodies, it should be pointed out that the prevalence of group B streptococcal antibodies among pregnant women is generally low, with only 7–23% sera having >2 μg/ml against types Ia, Ib, II, III, and V in a defined population.(194) Thus, the majority of infants are “antibody deficient,” whether colonized or not, yet only a small number develop disease, even when exposed to infected amniotic fluid in utero.(195) The presence of mucosal antibodies may modify colonization, but so far a clearly defined role for secretory immunity is not apparent.
Most of our knowledge of pneumococcal immunity comes from studies of purified polysaccharide vaccines. Adults respond well to most of the antigens, but infants respond poorly. Conjugate vaccines improve the immunogenicity of vaccines by coupling the polysaccharides to protein carriers to elicit T-helper cell involvement in the immune response. Although an IgG level of >0.2 mg/ml has been used as a marker of vaccine response, there is no consensus as to what constitutes a protective serum antibody level.(196)
35.8 Patterns of Host Response
35.8.1 Clinical Features
The manifestations of streptococcal diseases are remarkably diverse. Their clinical presentation, diagnosis, and therapy are discussed in detail in many of the medical, pediatric, and infectious disease textbooks. The most common and most important diseases caused by the major streptococcal group are listed in Table 6. Diseases associated with other streptococci are noted in Tables 1 and 2.
The typical form of group A streptococcal respiratory disease in children and adults is acute exudative pharyngitis. The onset is abrupt, with fever, chills, a sore throat with pain on swallowing, malaise, headache, often with abdominal pain, nausea, or vomiting. On physical examination, the pharyngeal mucosae are erythematous, edematous, and streaked with a purulent nonadherent exudate over the tonsils or posterior pharynx; petechiae may be present. The anterior cervical lymph nodes may be enlarged and are usually acutely tender. In young children the findings may be less specific, often with fever and lymphadenitis but relatively little inflammation of the upper respiratory mucosae. Mild or subclinical infection may occur at any age and may be missed. This is of concern because up to half of patients developing rheumatic fever do not give a clear history of an antecedent sore throat. With scarlet fever the pharyngitis is accompanied within about 24 h by a fine red exanthem beginning on the trunk and intertriginous areas, later spreading to the extremities. The face is usually spared, but the tongue may be inflamed with a “strawberry” appearance. Careful auscultation of the heart should be part of the physical examination on all patients with acute streptococcal sore throat or scarlet fever.
Streptococcal impetigo may appear as single lesions of the epidermis, frequently on the lower extremities, spreading to other areas as new insect bites or breaks in the skin become infected. Early lesions are pustular and rapidly develop into mature lesions about 1 cm in diameter with a characteristic honey-like crust. Lesions may become concomitantly infected by staphylococci, which may be resistant to penicillin therapy. Erysipelas is a serious superficial soft tissue infection that extends into the subcutaneous lymphatics and appears with a rapidly advancing well-demarcated border. Erysipelas often involves the face, a surgical wound, an umbilical stump, or a chicken pox lesion. The patient is febrile, toxic, and may be bacteremic. Necrotizing fasciitis is a deep-seated infection of subcutaneous tissue that destroys fascia and fat but may also destroy skin and muscle. Patients may be diabetic or otherwise debilitated. Recently reported cases have occurred mainly in previously healthy individuals who had trivial or inapparent trauma at the affected site. A hallmark, though nonspecific, is the rapid progression from tenderness to severe pain at the site of infection. Infections may become gangrenous and require surgical debridement or fasciotomy.
Streptococcal toxic shock has been observed with varying frequency in Europe and North America during the past decade or more.(4,13,20) Persons may be affected at all ages, usually without predisposing or underlying diseases. Most cases involve a skin or soft tissue focus of infection or pneumonia (as in the case of puppeteer Jim Henson), and most patients are bacteremic. In children a large proportion of cases are associated with infected chicken pox lesions, but this has almost disappeared as a risk factor since the routine use of varicella vaccine has been implemented. Criteria for diagnosis of streptococcal toxic shock are given in Table 7.(197) This syndrome differs from other serious streptococcal infections, and to some extent from staphylococcal toxic shock, by the rapid development of hypotension and multiorgan failure early in the course of infection. Streptococcal toxic shock is rarely associated with sunburn-type rash; however, such a rash is common in staphylococcal toxic shock syndrome.
The nonsuppurative sequelae of group A infections may present acutely or insidiously. Acute rheumatic fever varies greatly in its manifestations. The diagnosis was made with the guidance of the Jones Criteria (updated in 1992),(198) described in Table 8. The onset is typically abrupt, with fever and polyarthritis. Myocarditis or valvulitis, most commonly involving the mitral valve, occurs in about half of patients suffering their first attack. Carditis may be the only major manifestation in some patients and may develop insidiously, presenting as heart failure without any clear history of prior rheumatic fever or obvious streptococcal infection.(3,198) Because of difficulties in making the diagnosis, other conditions, such as collagen-vascular diseases and infective endocarditis, must be considered whenever acute rheumatic fever is suspected. Acute glomerulonephritis presents fewer diagnostic problems. A recent skin or throat infection is usually evident by examination, history, culture, or antibody tests. The urine is dark, containing many red blood cells and casts. The patient usually has edema and elevated blood pressure; the blood urea nitrogen and creatinine are usually elevated and the C3 complement level is low. With appropriate acute care, nearly all patients have a complete recovery.
Group B streptococcal disease in the neonate usually begins in utero with nonspecific symptoms appearing within the first few hours of birth.(26,163) Unexplained apnea, respiratory distress, temperature instability, or poor feeding may be the only clues to early-onset disease. Infection usually takes the form of undifferentiated sepsis with, or more often without, meningitis. The disease is well advanced by the time hypoxia, cyanosis, acidosis, or vascular collapse becomes obvious. Lung involvement is frequent but the chest X-ray is typical of hyaline membrane disease more often than of discrete pneumonia. Similarly, there may be little or no CSF pleocytosis even when bacteria are recovered from the spinal fluid. In general, the inflammatory response parallels the maturity of the infant, the specificity of clinical signs and symptoms, and to some extent the prognosis. Late-onset infections, occurring beyond the immediate newborn period, often tend to be more localized and have a better outcome. Meningitis is common, but sepsis without meningitis is frequently seen. Bacteremia or meningitis may be associated with an infective focus, such as omphalitis, otitis media, or osteomyelitis. The long-term outcome of infants who survive group B streptococcal meningitis is generally good. Very occasionally, neonates develop similar disease due to group G streptococci or pneumococci. Maternal group B streptococcal disease may occur during gestation, notably urinary tract infections and septic abortion. Infection around the time of delivery, especially amnionitis, is a threat to both fetus and mother. Endometritis and bacteremia are the most frequent postpartum infections. Endocarditis is an unusual complication of perinatal infection or septic abortion.(162)
Group B streptococcal disease also occurs in adult men and nonpregnant women. In a recent survey of invasive group B infections metropolitan Atlanta hospitals clinical diagnoses included skin, soft tissue, or bone infections (36%), bacteremia without focus (30%), urosepsis (14%), pneumonia (9%), and peritonitis (7%).(142) Another excellent clinical series, which also included data on group A, C, F, and G streptococcal infections, found that the case mortality rate was 31% among adults with group B streptococcal bacteremia.(199) Two-third of all patients were over 50 years of age, 22% had primary bacteremia, 25% had underlying nonhematologic malignancies, and 19% had diabetes mellitus. At least 50% of the mortality due to group B streptococci now occurs in the age group >65 years, attributed mainly to pneumonia and bacteremia without an identified focus.(143)
There is good evidence that group C and G streptococci are a cause of endemic pharyngitis in adults in open populations.(200,201) Of the several streptococci falling into serologic group C, it appears that large-colony Streptococcus equisimilis is more likely to be associated with clinical disease than the tiny-colony S. anginosis (“milleri”) group. The presence of these organisms must be determined by throat culture, because the rapid Streptococcus antigen detection kits are specific for group A streptococci.
35.9 Control and Prevention
35.9.1 General Preventive Measures
Personal hygiene, adequate nutrition and housing, health education, and access to medical care are all important factors in prevention of streptococcal diseases. Inspection of food and milk production and proper pasteurization of dairy products are taken for granted in most developed countries but remain problems in certain areas. Strict asepsis is required in surgical and obstetric procedures. Simple infection control measures, especially handwashing, must be continually encouraged, and attention must be paid to the health of hospital employees working in patient areas.
35.9.2 Antibiotics in Treatment and Prevention of Group A Streptococcal Disease
Primary prevention of acute rheumatic fever consists of identifying and treating persons with acute streptococcal pharyngitis.(30) Antibiotic therapy is aimed at eradicating streptococci from the respiratory tract. Shulman et al. have made the case over and again that penicillin remains the drug of choice for treatment of streptococcal pharyngitis.(110,202) Penicillin may be given as a single intramuscular injection of (“long-acting”) benzathine penicillin or as a 10-day course of oral phenoxymethyl penicillin. Other oral penicillins, especially amoxicillin, are also effective but are more expensive and offer no advantage other than palatability. The older oral cephalosporins (cephalexin, cefaclor, cephradine, cefadroxil) are effective in a number of conventional 10-day dose regimens. Several newer cephalosporins (cefprozil, cefpodoxime, loracarbef) are equally effective; 5-day dose regimens are currently under investigation but will not be recommended without further evaluation. Erythromycin is a well-established alternative drug for penicillin-allergic patients, except in some areas where resistance may be a problem. Clindamycin is effective but has a small potential risk of pseudomembranous enterocolitis. Tetracyclines, sulfonamides, and chloramphenicol are not effective.
Spread of streptococci within populations has been an effective means of reducing exposure in households and institutional settings. Mass prophylaxis with benzathine penicillin has been used in some epidemic situations but is now chiefly confined to certain military populations(157) (see Section 5.9). Eradication of pharyngeal carriage of group A streptococci using oral antibiotic regimens has been attempted with varying degrees of success. Effective regimens include amoxicillin/clavulanate (Augmentin®) or clindamycin orally for 10 days.(203,204) Patients with symptomatic streptococcal sore throat may remain infectious for 24 h after the onset of therapy and should not return to work, school, or day care before completing a full 24 h of antibiotic therapy.(181)
Secondary prevention consists of the regular administration of antibiotic to persons who have had rheumatic fever in order to prevent subsequent group A infections that could trigger recurrent attacks or exacerbate existing rheumatic heart disease.(30) Secondary prophylaxis is cost-effective, reduces the risk of recurrence, and in many patients allows for healing of valvular damage occurring in the initial attack. Long-acting intramuscular benzathine penicillin is usually given at intervals of 2–4 weeks, depending on local prevalence of rheumatic fever. Although dosing every 3 weeks may not provide adequate penicillin levels through the third week, this regime appears to be adequate in most situations and is often recommended.(205,206) Alternatively, oral penicillin may be given daily, but lack of compliance is a major problem. Patients unable to take penicillin may be given sulfadiazine or erythromycin. The duration of secondary prophylaxis is not certain but must be tailored to the individual. Patients with valvular rheumatic heart disease are given prolonged, even lifelong, prophylaxis. Those without cardiac involvement should have prophylaxis for at least 5 years and at least through age 18. Prophylaxis may be safely discontinued in young adults without carditis, provided that they have adequate medical follow-up and prompt culture and treatment of pharyngitis episodes.(207) Patients with rheumatic carditis as part of their initial attack are at greater risk for more serious carditis recurrences and should be given prophylaxis well into adulthood and perhaps for life.
Patients who have had isolated chorea as the only manifestation of rheumatic fever appear to be at much less risk for carditis during subsequent recurrences. Most authorities recommend that these patients receive prophylaxis until age 21 or for at least 5 years, whichever is longer. Some patients have a syndrome of poststreptococcal reactive arthritis without fulfilling Jones’ criteria. A few such patients have had silent or delayed mitral insufficiency and later developed acute rheumatic fever.(208) It is therefore generally recommended that patients with poststreptococcal reactive arthritis receive prophylaxis for at least 1 year at which point it may be discontinued if no evidence of carditis develops.(30)
The prevention of acute glomerulonephritis by antibiotic therapy has not been convincingly demonstrated, and prophylaxis may not be practical in most patient populations. Prompt treatment of minor skin trauma and insect bites with topical antibiotic ointment has been shown to reduce the occurrence of streptococcal skin infections and could reduce the risk of subsequent nephritis.(209,210)
Although it is well known that group A streptococci can spread from infected patients to close contacts, available evidence does not support the routine administration of prophylactic antibiotics to close or household contacts of patients with streptococcal toxic shock or necrotizing fasciitis.(211)
35.9.3 Surgical Approaches to Recurrent Group A Streptococcal Disease
Tonsillectomy or tonsillectomy with adenoidectomy are frequently performed because of recurrent throat infections. Although children who have surgery experience fewer throat infections over the subsequent 2 years, the difference in rates compared to controls is not impressive. These findings were confirmed by Paradise et al. in a carefully controlled study with stringent entry criteria.(212) Surgical intervention was beneficial for severely affected children over at least 2 years following surgery. Nevertheless, a substantial proportion of those managed nonsurgically had relatively little throat infection during the period of study, and the actual reduction in group A streptococcal infection rates was small. Their results appeared to “justify but by no means to mandate the performance of tonsillectomy” in carefully selected children. Treatment should be individualized, and should be considered only for severely affected children. More clearly defined indications for surgical intervention include patients with peritonsillar abscess or severe obstructive symptoms.
35.9.4 Antibiotics in Treatment and Prevention of Endocarditis
Several national groups periodically issue detailed guideline for management of infective endo-carditis.(108,213,214) The major organisms include viridans streptococci and S. bovis, Abiotriphia and Granulicatella, S. pneumonia, group A, B, C, and G streptococci, and Enterococcus. Dosage and duration of antibiotic therapy depend upon whether the offending organism is highly susceptible or relatively resistant to penicillin. Enterococci vary in susceptibility to penicillin and gentamicin, and some strains, especially among E. faecium, are resistant to vancomycin.
Guidelines for prevention of infective endocarditis have recently been revised by British and American cardiology, dental, and infectious disease organizations.(215,216) Whereas it used to be commonplace to administer antibiotics prior to dental procedures for patients with a wide range of heart valve disorders, now only few limited diagnoses are considered for prophylaxis. These include patients with prosthetic heart valves, patients with a prior history of endocarditis, and those with unrepaired congenital heart disease and those with residual defects, prosthetic materials or devices that inhibit endothelialization. It has been concluded that bacteremia resulting from daily activities is much more likely to cause endocarditis than bacteremia associated with dental procedures. Only an extremely small number of cases would be prevented even if prophylaxis were 100% effective. Scientific data demonstrating the efficacy of prophylaxis is lacking, except for conditions associated with highest risks for adverse outcomes.
35.9.5 Intrapartum Chemoprophylaxis Against Group B Streptococcal Disease
The rates of early-onset group B streptococcal invasive disease have declined significantly following the implementation of various programs of maternal screening and administration of intrapartum antibiotics, as described in Section 5.1. The original 1996 guidelines, a compromise that used either maternal culture screening or maternal risk factors, resulted in a 65% decrease in early-onset cases. Subsequent population-based surveillance of the two different approaches found that culture-based programs were at least 50% more effective than risk-based programs.(134) This prompted a revision of the guidelines in 2002 by the CDC in cooperation with the American College of Obstetricians and Gynecologist (ACOG) and the American Academy of Pediatrics (AAP).(28) The new guidelines, outlined in Figure 4, is based on results of combined vaginal and rectal culture performed on women at 35–37 weeks of gestation. Further surveillance during 2002–2004 has confirmed that the rates of early-onset disease have declined an additional 31% since implementation of the new guidelines.(14) Several European countries and Australia have instituted similar guidelines, and Dutch investigators have recommended a shift from risk-based to screening-based programs.(136)

Indications for intrapartum antibiotic prophylaxis to prevent perinatal GBS disease under a universal prenatal screening strategy based on combined vaginal and rectal cultures collected at 35- to 37-week gestation from all pregnant women. (From Centers for Disease Control and Prevention.(237))
The 2002 guidelines call for using penicillin G as the first choice for intrapartum prophylaxis, with ampicillin or cefazolin as alternatives.(28) A potential problem with antibiotic use in this setting is the possibility of selecting organisms with increased antibiotic resistance. So far no group B streptococci have become penicillin resistant. There is, however, some increased frequency of resistance to clindamycin, which is used as an alternative for penicillin-allergic patients.(27) Resistance to ampicillin among nontarget organisms, such as Escherichia coli, parallels rates in other community-acquired infections and does not appear to be related directly to intrapartum prophylaxis. Nevertheless, the resistance patterns of other organisms causing neonatal sepsis should receive continued attention and surveillance.(28)
Prevention of neonatal infections by vaginal chlorhexidine disinfection during labor has also been investigated.(217) A reduction in transmission of group B streptococci from mother to infant has been demonstrated, but numbers have been too small to assess an effect of prevention of infections.(218) This approach might reduce the number of infection that develop as a result to colonization of infants during delivery, but as with intrapartum antibiotics, it should not be expected to affect infections that are already established in utero.
35.9.6 Passive Immune Prophylaxis Against Streptococcal Infections
The administration of gamma globulin has been employed for prevention of various bacterial infections in immunodeficient patients. The spectrum of host defense abnormalities that may benefit from this approach now includes patients with hypogammaglobulinemias, IgG subclass deficiencies, malignancy and immunosuppression, severe burns, bone marrow transplantation, and HIV infection.(219) Although passive immunotherapy was the only efficacious treatment for pneumococcal pneumonia in the years prior to the advent of antibiotics, no immunoglobulin products are in current use as adjunctive treatment for streptococcal infections.
35.9.7 Immunization Against Streptococcal Infections
A vaccine against rheumatic fever has been the holy grail of many investigators over the years. As reviewed by Bisno et al., current research involves two broad categories of vaccines: those based on type-specific M protein components and others containing virulence determinants that are common to all or many serotypes.(220) The M protein molecule is a coiled coil with three main antigenic regions: a nonhelical amino-terminus conferring type specificity and susceptible to antibody; the second area consists of B repeat subunits that cross-react with human tissue components; a third C repeat region has epitopes common to many M proteins; finally, the carboxy terminus ends with a cell wall spanning anchor region.(73) A multivalent recombinant M-type vaccine has now been constructed using the amino-terminal peptides of 26 of the clinically most important M types.(221) This vaccine has been tested for safety and immunogenicity in humans, and it elicits opsonizing antibodies to the respective M types. The vaccine does not contain any tissue cross-reactiveM epitopes from the B repeat area of the M protein and thus should not be able to provoke autoimmune-like responses. Other approaches to vaccines are promising but have not yet been studied in humans. A vaccine that contains epitopes of the carboxy-terminal C repeat area of the M protein cross-reacts with most of the common M types but also avoids the tissue-reactive B repeat area.(222) Another vaccine uses a lipid core as a carrier for the C repeat peptide, which has the advantage of not requiring a vaccine adjuvant.(223) A vaccine against the group A carbohydrate is enhanced by conjugation to tetanus toxoid to produce antibodies presumably protective against all strains.(76) A vaccine against the fibronectin-binding protein (FB54) targets a surface protein strongly associated with virulence.(224) Vaccines against the C5a peptidase of either group A or group B streptococci might not be directly protective but could reduce the effects of the more serious invasive infections.(225)
Group B streptococcal polysaccharide vaccines have been under investigation for over two decades.(226) Although intrapartum antibiotic prophylaxis has been fairly successful, it fails to prevent about 25% of early-onset infections and does not late-onset disease. Vaccines are projected to offer broader more cost-effective protection.(227) The goal of the vaccine approach is to immunize women in order to induce antibody that will later be capable of protecting the fetus against early-onset disease and perhaps afford protection for several months against late-onset disease. Ideally, a vaccine should induce antibodies of the IgG class to cross the placenta and be effective against all of the major serotypes. The first purified polysaccharide vaccine, against type III, was only modestly immunogenic. The immunogenicity was significantly improved by conjugation to tetanus toxoid, as was so successful with Hemophilus influenzae and pneumococcal vaccines. Phase I and phase 2 clinical trials have been successfully conducted with individual conjugates of types Ia, Ib, II, III, and V, and preclinical testing has been done with several multivalent vaccines.(226) Several surface proteins of known association with virulence are also being considered. These include several proteins common to nearly all strains, such as alpha, Sip, Rib, and the C5a peptidase, and the c protein, which occurs mainly with type Ia and Ib strains.(44,228) Assuming the eventual development of an appropriate vaccine, it will still be necessary to carefully define the target population. There is yet little enthusiasm for administering vaccines to pregnant women, mainly because of safety and liability issues.(229) It is possible that the target population would have to focus on or include nonpregnant women of childbearing age. The prospects for protecting the more premature fetus is uncertain, since only a minimal amount of maternally derived antibody is able to cross the placenta before the last trimester.(193) Nevertheless, it would be reasonable to suggest that any degree of protection afforded the mother would indirectly affect the fetus.
Pneumococcal vaccines have been studied for nearly 80 years. The 23-valent pneumococcal polysaccharide vaccine licensed in 1983 has been moderately successful in preventing invasive disease adults but has had little effect on nonbacteremic pneumonia.(230) A pediatric 7-valent conjugate vaccine (containing types 1 or 4, 6B, 9 V, 14, 18C, 19F, and 23F) was introduced in the United States in 2000, resulting in a decrease of at least 60% in invasive pneumococcal disease among children less than 2 years of age.(170) Wide application of this vaccine has also benefited older adults by producing “herd immunity” and reducing spread.(171) However, nonvaccine serotypes are starting to creep into the population, including a particularly virulent 19A strain.(117) The need for a more universal pneumococcal vaccine is apparent. Several pneumococcal surface proteins, such as PspA, are currently being studied as candidate vaccine for humans.(103,231)
35.9.8 Prevention of Dental Caries
Conventional approaches to caries prevention have been succinctly reviewed in the Canadian Task on the Periodic Health Examination.(147) Primary prevention includes fluoride, fissure sealants, dietary counseling, oral hygiene, and identification and care of individuals at high risk of developing dental caries. Patients at greatest risk are those with bulimia, Sjögren’s syndrome, chemotherapy, radiation therapy, or use of drugs that reduce saliva flow over long periods.
Fluoride-containing toothpastes afford considerable protection against dental caries and are the now most widely used method of providing fluoride. Fluoridation of drinking water at levels of 0.7–1.2 ppm remains an effective public health measure but is not without controversy. About two-thirds of the US population receive fluoridated water, compared to 40% in Canada, 10% in the United Kingdom and in Spain. France does not fluoridate, and Switzerland has replaced fluoridation with fluoride in domestic salt. Fluoride mouthwashes are probably of marginal value in communities with fluoridated water. They are not intended for children under 5 years of age, who may ingest excessive amounts and be in danger of fluorosis. Professional application of topical fluoride may be helpful for high-risk individuals and patients with active caries but is not currently recommended for routine use because of the overall decline in caries incidence.
Sealing of dental pits and fissures with synthetic resins has been done for over 15 years with modest success. Sealants do not add significant protection to initially sound tooth surfaces but may add to further reductions in caries where rates are already quite low.(146) This approach is recommended for selected high-risk patients whose permanent molars have erupted within the previous 2–3 years.(147)
Traditional brushing and flossing has little or no effect on caries prevention, except as a method of applying fluoride in the dentifrice. Professional cleaning (dental prophylaxis) does not prevent caries, although it may be useful for removing stains or calculus. The effectiveness of dietary counseling aimed at reducing intake of sucrose has not been established. Avoiding prolonged use of baby bottles and bedtime bottle propping may prevent “nursing caries.” Nevertheless, it is now recognized that parental attitudes and beliefs play a key role in moderating oral health-related behavior in young children.(148)
Vaccines against dental caries, based on antigens derived from S. mutans, have been under investigation for a number of years.(184,232) Experimental vaccines have been successful in preventing caries in animals. Candidate vaccines include surface adhesins (Ag I/II, antigen B), glycosytransferases (GTF) that synthesize adhesive glucan from sucrose, and glucan-binding proteins. Several small clinical trials have demonstrated the feasibility of similar vaccines in humans. GTF vaccines given orally, intranasally, or topically applied to tonsils have been shown to induce salivary IgA antibody responses in humans, but long-term evaluations of efficacy have not been done. The major reason is that dental caries is not a life-threatening disease, and potential benefits must clearly outweigh even theoretical concerns of safety.
35.10 Unresolved Problems
Despite the availability of antibiotics, the diagnosis and treatment of group A streptococcal pharyngitis continue to pose problems for the clinician. The distinction between infection and carrier state is frequently blurred. The new rapid diagnostic tests make it possible to treat promptly and reduce clinical symptoms, but it is unlikely that changes in clinical practice have influenced the recent resurgence of acute rheumatic fever or of severe invasive streptococcal disease and toxic shock. Further study of epidemiologic factors, pathogenic mechanisms, and host response is clearly needed. Poststreptococcal reactive arthritis and its less certain relationship with cardiac sequelae continues to present a clinical dilemma for clinicians.(208) Group A streptococci, along with staphylococci, have been suggested as an etiology for Kawasaki disease, a vasculitis syndrome that occurs mainly in children. It is hypothesized that staphylococcal toxin TSST-1 or streptococcal exotoxins act as superantigens and cause aberrant amplification of certain T-cell lines implicated in the disease process.(233)
Group B streptococci remain the most common cause of serious bacterial disease in newborn infants in many western countries. Despite similar maternal colonization rates and presumably similar risk of exposure, the disease is infrequent in some areas of Europe and Asia. The reasons for this are not clear but could be of considerable practical importance. Methods for intrapartum antibiotic prophylaxis have been established but remain to be implemented on a wide scale. Meanwhile, we still have little understanding of the local and systemic defense mechanisms required to prevent infection by this usually benign organism. Other streptococci, particularly oral and enteric species, are constant companions that cause disease only under specialized circumstances. It is not clear whether some of these organisms are in fact “virulent” in certain settings, or whether the disease is due mainly to predisposing conditions in the host. The question may be moot, but answers would help us direct attention to better ways of preventing nosocomial and opportunistic infections.
The unanswered questions apparent from the discussions in this chapter remain: how do streptococci cause disease, and why do some individuals become infected while others do not? Many pathogenic strains of group A Streptococcus have been sequenced and genes corresponding to virulence factors have been catalogued. However, the regulation of these genes has not been adequately investigated. In addition, major virulence factors, such as exotoxins, enzymes, M proteins and polysaccharide capsules, have been identified, but the pathophysiologic mechanisms by which they interact with the host remain uncertain and do not completely explain the disease processes. The determinants of colonization, the defenses of the host at the mucosal level, and the development of local and systemic immunity are not well understood. More needs to be learned to facilitate the development of effective vaccines and implement other preventive measures.
References
Quinn R. Streptococcal infections, in: Bacterial Infections in Humans, 1st ed. (AS Evans and HA Feldman, eds.), pp. 525–52, Plenum Press, New York (1982)
Stollerman GH. (editorial) Variation in group A Streptococci and the prevalence of rheumatic fever: a half-century vigil. Ann Intern Med;118:467–9 (1993)
Veasy LG, Tani LY and Hill HR. Persistence of acute rheumatic fever in the intermountain area of the United States. J Pediatr;124:9–16 (1994)
Stevens DL. Invasive group A Streptococcus infections. Clin Infect Dis;14:2–13 (1992)
Lancefield RC, Hare R. The serological differentiation of pathogenic and non-pathogenic strains of hemolytic Streptococci from parturient women. J Exp Med;61:335–49 (1935)
Gray BM, Musher DM. History of pneumococcal infections. in: Pneumococcal Vaccines: The Impact of Conjugate Vaccine, (GR Siber, et al., eds.), The American Society for Microbiology Press, Washington, DC (2008)
Loesche WJ. Role of Streptococcus mutans in human dental decay. Microbiol Rev;50:353–80 (1986)
Caufield PW, Cutter GR, Dasanayake AP. Initial acquisition of mutans streptococci by infants: evidence for a discrete window of infectivity. J Dent Res;72:37–45 (1993)
van Houte J. Role of micro-organisms in caries etiology. J Dent Res;73:672–81 (1994)
Arends JP, Zanen HC. Meningitis caused by Streptococcus suis in humans. Rev Infect Dis;10:131–7 (1988)
Lun ZR, Wang QP, Chen XG, Li AX and Zhu XQ. Streptococcus suis: an emerging zoonotic pathogen. Lancet Infect Dis;7:201–9 (2007)
Zirakzadeh A, Patel R. Vancomycin-resistant enterococci: colonization, infection, detection, and treatment. Mayo Clin Proc;81:529–36 (2006)
O’Loughlin RE, Roberson A, Cieslak PR, et al. The epidemiology of invasive group A streptococcal infection and potential vaccine implications: United States, 2000–2004. Clin Infect Dis;45:853–62 (2007)
CDC CfDCaP. Early-onset and late-onset neonatal group B streptococcal disease—United States, 1996–2004. MMWR Morb Mortal Wkly Rep;54:1205–8 (2005)
Lexau CA, Lynfield R, Danila R, et al. Changing epidemiology of invasive pneumococcal disease among older adults in the era of pediatric pneumococcal conjugate vaccine. Jama;294:2043–51 (2005)
Trijbels-Smeulders MA, Kollee LA, Adriaanse AH, Kimpen JL and Gerards LJ. Neonatal group B streptococcal infection: incidence and strategies for prevention in Europe. Pediatr Infect Dis J;23:172–3 (2004)
Lamagni TL, Efstratiou A, Vuopio-Varkila J, Jasir A and Schalen C. The epidemiology of severe Streptococcus pyogenes associated disease in Europe. Euro Surveill;10:179–84 (2005)
Pebody RG, Hellenbrand W, D’Ancona F and Ruutu P. Pneumococcal disease surveillance in Europe. Euro Surveill;11:171–8 (2006)
Ekelund K, Skinhoj P, Madsen J and Konradsen HB. Invasive group A, B, C and G streptococcal infections in Denmark 1999–2002: epidemiological and clinical aspects. Clin Microbiol Infect;11:569–76 (2005)
Vlaminckx BJ, van Pelt W, Schouls LM, et al. Long-term surveillance of invasive group A streptococcal disease in The Netherlands, 1994–2003. Clin Microbiol Infect;11:226–31 (2005)
NNIS. National Nosocomial Infections Surveillance (NNIS) System Report, data summary from January 1992 through June 2004, issued October 2004. Am J Infect Control;32:470–85 (2004)
Taranta A, Markowitiz M. Rheumatic Fever, 2nd ed., Kluwer Academic Press, Boston, MA (1989)
Carapetis JR, Steer AC, Mulholland EK and Weber M. The global burden of group A streptococcal diseases. Lancet Infect Dis;5:685–94 (2005)
Facklam R. What happened to the streptococci: overview of taxonomic and nomenclature changes. Clin Microbiol Rev;15:613–30 (2002)
Kohler W. The present state of species within the genera Streptococcus and Enterococcus. Int J Med Microbiol;297:133–50 (2007)
Dillon HC, Jr., Khare S and Gray BM. Group B streptococcal carriage and disease: a 6-year prospective study. J Pediatr;110:31–36 (1987)
Lin FY, Azimi PH, Weisman LE, et al. Antibiotic susceptibility profiles for group B streptococci isolated from neonates, 1995–1998. Clin Infect Dis;31:76–9 (2000)
Schrag S, Gorwitz R, Fultz-Butts K and Schuchat A. Prevention of perinatal group B streptococcal disease. Revised guidelines from CDC. MMWR Recomm Rep;51:1–22 (2002)
de la Rosa-Fraile M, Camacho-Munoz E. Liquid Granada medium for detection of group B streptococci. J Clin Microbiol;43:4303 (2005)
Bisno AL, Gerber MA, Gwaltney JM, Jr., Kaplan EL and Schwartz RH. Practice guidelines for the diagnosis and management of group A streptococcal pharyngitis. Infectious Diseases Society of America. Clin Infect Dis;35:113–25 (2002)
Ascher DP, Wilson S, Mendiola J and Fischer GW. Group B streptococcal latex agglutination testing in neonates. J Pediatr;119:458–60 (1991)
Bergeron MG, Ke D, Menard C, et al. Rapid detection of group B streptococci in pregnant women at delivery. N Engl J Med;343: 175–9 (2000)
Tanna A, Emery M, Dhami C, Arnold E and Efstratiou A. Molecular characterization of clinical isolates of M non-typeable group A streptococci from invasive disease cases. J Med Microbiol;55: 1419–23 (2006)
Johnson D, Kaplan E. A review of the correlation of T-agglutination patterns and M-protein typing and opacity factor production in the identification of group A streptococci. J Med Microbiol;38:311–5 (1993)
Dillon HC, Derrick CW and Dillon MS. M-antigens common to pyoderma and acute glomerulonephritis. J Infect Dis;130:257–67 (1974)
Johnson DR, Stevens DL and Kaplan EL. Epidemiologic analysis of Group A streptococcal serotypes associated with severe systemic infections, rheumatic fever, or uncomplicated pharyngitis. J Infect Dis;166:374–382 (1992)
Colman G, Tanna A, Efstratiou A and Gaworzewska ET. The serotypes of Streptococcus pyogenes present in Britain during 1980–1990 and their association with disease. J Med Microbiol;39:165–78 (1993)
Currie BJ. Group A streptococcal infections of the skin: molecular advances but limited therapeutic progress. Curr Opin Infect Dis;19:132–8 (2006)
Hollingshead SK, Arnold J, Readdy TL and Bessen DE. Molecular evolution of a multi-gene family in group A streptococci. (1993)
Sumby P, Porcella SF, Madrigal AG, et al. Evolutionary origin and emergence of a highly successful clone of serotype M1 group A Streptococcus involved multiple horizontal gene transfer events. J Infect Dis;192:771–82 (2005)
Kratovac Z, Manoharan A, Luo F, Lizano S and Bessen DE. Population genetics and linkage analysis of loci within the FCT region of Streptococcus pyogenes. J Bacteriol;189:1299–310 (2007)
Ryc M, Jelinkova J, Motlova J and Wagner M. Immuno-electronmicroscopic demonstration of capsules on group-B streptococci of new serotypes and type candidates. J Med Microbiol;25: 147–9 (1988)
Slotved HC, Kong F, Lambertsen L, Sauer S and Gilbert GL. Serotype IX, a Proposed New Streptococcus agalactiae Serotype. J Clin Microbiol;45:2929–36 (2007)
Lindahl G, Stalhammar-Carlemalm M and Areschoug T. Surface proteins of Streptococcus agalactiae and related proteins in other bacterial pathogens. Clin Microbiol Rev;18:102–27 (2005)
Park IH, Pritchard DG, Cartee R, Brandao A, Brandileone MC and Nahm MH. Discovery of a new capsular serotype (6C) within serogroup 6 of Streptococcus pneumoniae. J Clin Microbiol;45: 1225–33 (2007)
Raff GW, Gray BM, Torres A, Jr. and Hasselman TE. Aortitis in a child with Abiotrophia defectiva endocarditis. Pediatr Infect Dis J;23:574–6 (2004)
Facklam RR, Carvalho MGS and Teixeira LM. History, taxonomy biochemical characteristics, and antibiotic susceptibility testing of enterococci, in: The Enterococci: Pathogenesis, Molecular Biology, and Antibiotic Resistance, (MS Gilmore, DB Clewell, P Couvalin, et al., eds.), pp. 1–54, American Society for Microbiology, Washington, DC (2002)
Chapin KC, Blake P and Wilson CD. Performance characteristics and utilization of rapid antigen test, DNA probe, and culture for detection of group A streptococci in an acute care clinic. J Clin Microbiol;40:4207–10 (2002)
Messmer TO, Sampson JS, Stinson A, Wong B, Carlone GM and Facklam RR. Comparison of four polymerase chain reaction assays for specificity in the identification of Streptococcus pneumoniae. Diagn Microbiol Infect Dis;49:249–54 (2004)
Facklam R, Beall B, Efstratiou A, et al. emm typing and validation of provisional M types for group A streptococci. Emerg Infect Dis;5:247–53 (1999)
Neal S, Beall B, Ekelund K, et al. International quality assurance study for characterization of Streptococcus pyogenes. J Clin Microbiol;45:1175–9 (2007)
Doktor SZ, Beyer JM, Flamm RK and Shortridge VD. Comparison of emm typing and ribotyping with three restriction enzymes to characterize clinical isolates of Streptococcus pyogenes. J Clin Microbiol;43:150–5 (2005)
Mihaila-Amrouche L, Bouvet A and Loubinoux J. Clonal spread of emm type 28 isolates of Streptococcus pyogenes that are multiresistant to antibiotics. J Clin Microbiol;42:3844–6 (2004)
Blumberg HM, Stephens DS, Licitra C, et al. Molecular epidemiology of group B streptococcal infections: use of restriction endonuclease analysis of chromosomal DNA and DNA restriction fragment length polymorphisms of ribosomal RNA genes (ribotyping). J Infect Dis;166:574–9 (1992)
Martin NJ, Kaplan EL, Gerber MA, et al. Comparison of epidemic and endemic group G Streptococci by restriction and enzyme analysis. J Clin Microbiol;28:1881–6 (1990)
Hermans PWM, Sluijter M, Hoogenboezem T, Heersma H, van Belkum A and de Groot R. Comparative study of five different DNA fingerprint techniques for molecular typing of Streptococcus pneumoniae strains. J Clin Microbiol;33:1606–12 (1995)
Willems RJ, Top J, van Santen M, et al. Global spread of vancomycin-resistant Enterococcus faecium from distinct nosocomial genetic complex. Emerg Infect Dis;11:821–8 (2005)
Dobbs TE, Patel M, Waites KB, Moser SA, Stamm AM and Hoesley CJ. Nosocomial spread of Enterococcus faecium resistant to vancomycin and linezolid in a tertiary care medical center. J Clin Microbiol;44:3368–70 (2006)
Musser JM, Kapur V, Kanjilal S, et al. Geographic and temporal distribution and molecular characterization of two highly pathogenic clones of Streptococcus pyogenes expressing allelic variants of pyrogenic exotoxin A (Scarlet fever toxin). J Infect Dis;167:337–46 (1993)
Maiden MC. Multilocus sequence typing of bacteria. Annu Rev Microbiol;60:561–88 (2006)
Enright MC, Spratt BG, Kalia A, Cross JH and Bessen DE. Multilocus sequence typing of Streptococcus pyogenes and the relationships between emm type and clone. Infect Immun;69:2416–27 (2001)
Jones N, Bohnsack JF, Takahashi S, et al. Multilocus sequence typing system for group B Streptococcus. J Clin Microbiol;41:2530–6 (2003)
Enright MC, Spratt BG. A multilocus sequence typing scheme for Streptococcus pneumoniae: identification of clones associated with serious invasive disease. Microbiology;144 (Pt 11):3049–60 (1998)
King SJ, Leigh JA, Heath PJ, et al. Development of a multilocus sequence typing scheme for the pig pathogen Streptococcus suis: identification of virulent clones and potential capsular serotype exchange. J Clin Microbiol;40:3671–80 (2002)
Homan WL, Tribe D, Poznanski S, et al. Multilocus sequence typing scheme for Enterococcus faecium. J Clin Microbiol;40:1963–71 (2002)
Ramaswamy SV, Ferrieri P, Flores AE and Paoletti LC. Molecular characterization of nontypeable group B Streptococcus. J Clin Microbiol;44:2398–403 (2006)
Hanage WP, Kaijalainen T, Herva E, Saukkoriipi A, Syrjanen R and Spratt BG. Using multilocus sequence data to define the pneumococcus. J Bacteriol;187:6223–30 (2005)
Titze-de-Almeida R, Willems RJ, Top J, et al. Multilocus variable-number tandem-repeat polymorphism among Brazilian Enterococcus faecalis strains. J Clin Microbiol;42:4879–81 (2004)
Koeck JL, Njanpop-Lafourcade BM, Cade S, et al. Evaluation and selection of tandem repeat loci for Streptococcus pneumoniae MLVA strain typing. BMC Microbiol;5:66 (2005)
Top J, Schouls LM, Bonten MJ and Willems RJ. Multiple-locus variable-number tandem repeat analysis, a novel typing scheme to study the genetic relatedness and epidemiology of Enterococcus faecium isolates. J Clin Microbiol;42:4503–11 (2004)
Werner G, Klare I and Witte W. The current MLVA typing scheme for Enterococcus faecium is less discriminatory than MLST and PFGE for epidemic-virulent, hospital-adapted clonal types. BMC Microbiol;7:28 (2007)
Shet A, Kaplan EL. Clinical use and interpretation of group A streptococcal antibody tests: a practical approach for the pediatrician or primary care physician. Pediatr Infect Dis J;21:420–6; quiz 427–30 (2002)
Fishcetti V. Streptococcal M protein: molecular design and biological behavior. Clin Microbiol Rev;2:285–314 (1989)
Stollerman GH. Rheumatogenic streptococci and autoimmunity. Clin Immunol Immunopathol;61:131–42 (1991)
Cunningham MW. Pathogenesis of group A streptococcal infections. Clin Microbiol Rev;13:470–511 (2000)
Sabharwal H, Michon F, Nelson D, et al. Group A Streptococcus (GAS) carbohydrate as an immunogen for protection against GAS infection. J Infect Dis;193:129–35 (2006)
Shulman ST, Stollerman G, Beall B, Dale JB and Tanz RR. Temporal changes in streptococcal M protein types and the near-disappearance of acute rheumatic fever in the United States. Clin Infect Dis;42: 441–7 (2006)
Beachey EH, Courtney HS. Bacterial adherence: the attachment of group A Streptococci to mucosal surfaces. Rev Infect Dis;9:S475–81 (1987)
Yarnall M, Boyle MDP. Isolation and characterization of type IIa and type IIb Fc receptors from a group A Streptococcus. Scand J Immunol;24:549–57 (1986)
Nizet V. Streptococcal beta-hemolysins: genetics and role in disease pathogenesis. Trends Microbiol;10:575–80 (2002)
Michos A, Gryllos I, Hakansson A, Srivastava A, Kokkotou E and Wessels MR. Enhancement of streptolysin O activity and intrinsic cytotoxic effects of the group A streptococcal toxin, NAD-glycohydrolase. J Biol Chem;281:8216–23 (2006)
Datta V, Myskowski SM, Kwinn LA, et al. Mutational analysis of the group A streptococcal operon encoding streptolysin S and its virulence role in invasive infection. Mol Microbiol;56:681–95 (2005)
Sumby P, Barbian KD, Gardner DJ, et al. Extracellular deoxyribonuclease made by group A Streptococcus assists pathogenesis by enhancing evasion of the innate immune response. Proc Natl Acad Sci U S A;102:1679–84 (2005)
Starr CR, Engleberg NC. Role of hyaluronidase in subcutaneous spread and growth of group A Streptococcus. Infect Immun;74:40–8 (2006)
Ohkuni H, Todome Y, Suzuki H, et al. Immunochemical studies and complete amino acid sequence of the streptokinase from Streptococcus pyogenes (group A) M type 12 Strain A374. Infect Immun;60:278–83 (1992)
Stevens DL, Salmi DB, McIndoo ER and Bryant AE. Molecular epidemiology of nga and NAD glycohydrolase/ADP-ribosyltransferase activity among Streptococcus pyogenes causing streptococcal toxic shock syndrome. J Infect Dis;182:1117–28 (2000)
Collin M, Olsen A. Extracellular enzymes with immunomodulating activities: variations on a theme in Streptococcus pyogenes. Infect Immun;71:2983–92 (2003)
Bisno AL, Brito MO and Collins CM. Molecular basis of group A streptococcal virulence. Lancet Infect Dis;3:191–200 (2003)
Proft T, Fraser JD. Streptococcal superantigens. Chem Immunol Allergy;93:1–23 (2007)
Hakansson S, Granlund-Edstedt M, Sellin M and Holm SE. Demonstration and characterization of buoyant-density subpopulations of group B Streptococcus type III. J Infect Dis;161:741–6 (1990)
Gray BM, Pritchard DG. Phase variation in the pathogenesis of group B streptococcal infections, in: New Perspectives on Streptococci and Streptococcal Infections, (G Orifici, ed.), Zbl Bakt;Suppl 22:452–4 (1992)
Doran KS, Nizet V. Molecular pathogenesis of neonatal group B streptococcal infection: no longer in its infancy. Mol Microbiol; 54:23–31 (2004)
Raff HV, Siscoe PJ, Wolff EA, Maloney G and Shuford W. Human monoclonal antibodies to group B Streptococcus reactivity and in vivo protection against multiple serotypes. J Exp Med;168:905–17 (1988)
Lancefield RC, McCarty M and Everly WN. Multiple mouse-protective antibodies directed against group B Streptococci. J Exp Med;142:165–79 (1975)
Baron MJ, Filman DJ, Prophete GA, Hogle JM and Madoff LC. Identification of a glycosaminoglycan binding region of the alpha C protein that mediates entry of group B Streptococci into host cells. J Biol Chem;282:10526–36 (2007)
Henneke P, Berner R. Interaction of neonatal phagocytes with group B Streptococcus: recognition and response. Infect Immun;74: 3085–95 (2006)
Pritchard DG, Lin B, Willingham TR and Baker JR. Characterization of the group B streptococcal hyaluronate lyase. Arch Biochem Biophys;315:431–7 (1994)
Hensler ME, Quach D, Hsieh CJ, Doran KS and Nizet V. CAMP factor is not essential for systemic virulence of Group B Streptococcus. Microb Pathog (2007)
Bohnsack JF, Zhou X, Williams PA, Cleary PP, Parker CJ and Hill HR. Purification of the proteinase of group B streptococci that inactivates human C5a. Biochim Biophys Acta;1079:222–8 (1991)
Schlievert PM, Gocke JE and Deringer JR. Group B streptococcal toxic shock-like syndrome: report of a case and purification of an associated pyrogenic toxin. Clin Infect Dis;17:26–31 (1993)
Bogaert D, Hermans PW, Adrian PV, Rumke HC and de Groot R. Pneumococcal vaccines: an update on current strategies. Vaccine;22:2209–20 (2004)
Vitharsson G, Jonsdottir I, Jonsson S and Valdimarsson H. Opsonization and antibodies to capsular and cell wall polysaccharides of Streptococcus pneumoniae. J Infect Dis;170:592–9 (1994)
Ogunniyi AD, Grabowicz M, Briles DE, Cook J and Paton JC. Development of a vaccine against invasive pneumococcal disease based on combinations of virulence proteins of Streptococcus pneumoniae. Infect Immun;75:350–7 (2007)
McCoy HE, Broder CC and Lottenberg R. Streptokinases produced by pathogenic group C streptococci demonstrate species-specific plasminogen activation. J Infect Dis;164:515–21 (1991)
Gnann JW, Gray BM, Griffin FM, Jr. and Dismukes WE. Acute glomerulonephritis following group G streptococcal infection. J Infect Dis;156:411–2 (1987)
Kanamori S, Kusano N, Shinzato T and Saito A. The role of the capsule of the Streptococcus milleri group in its pathogenicity. J Infect Chemother;10:105–9 (2004)
Napimoga MH, Hofling JF, Klein MI, Kamiya RU and Goncalves RB. Transmission, diversity and virulence factors of Sreptococcus mutans genotypes. J Oral Sci;47:59–64 (2005)
Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America. Circulation;111:e394–434 (2005)
Gerber MA, Tanz RR, Kabat W, et al. Potential mechanisms for failure to eradicate group A streptococci from the pharynx. Pediatrics;104:911–7 (1999)
Shulman ST, Gerber MA. So what’s wrong with penicillin for strep throat? Pediatrics;113:1816–9 (2004)
Brook I. Failure of penicillin to eradicate group A beta-hemolytic streptococci tonsillitis: causes and management. J Otolaryngol; 30:324–9 (2001)
Tanz RR, Shulman ST, Sroka PA, Marubio S, Brook I and Yogev R. Lack of influence of beta-lactamase-producing flora on recovery of group A streptococci after treatment of acute pharyngitis. J Pediatr;117:859–63 (1990)
Molinari G, Chhatwal GS. Invasion and survival of Streptococcus pyogenes in eukaryotic cells correlates with the source of the clinical isolates. J Infect Dis;177:1600–7 (1998)
Green MD, Beall B, Marcon MJ, et al. Multicentre surveillance of the prevalence and molecular epidemiology of macrolide resistance among pharyngeal isolates of group A streptococci in the USA. J Antimicrob Chemother;57:1240–3 (2006)
Gagliotti C, Nobilio L, Milandri M and Moro ML. Macrolide prescriptions and erythromycin resistance of Streptococcus pyogenes. Clin Infect Dis;42:1153–6 (2006)
Bergman M, Huikko S, Huovinen P, Paakkari P and Seppala H. Macrolide and azithromycin use are linked to increased macrolide resistance in Streptococcus pneumoniae. Antimicrob Agents Chemother; 50:3646–50 (2006)
Pelton SI, Huot H, Finkelstein JA, et al. Emergence of 19A as virulent and multidrug resistant Pneumococcus in Massachusetts following universal immunization of infants with pneumococcal conjugate vaccine. Pediatr Infect Dis J;26:468–72 (2007)
Betriu C, Gomez M, Sanchez A, Cruceyra A, Romero J and Picazo JJ. Antibiotic resistance and penicillin tolerance in clinical isolates of group B streptococci. Antimicrob Agents Chemother;38:2183–6 (1994)
DiPersio LP, DiPersio JR. High rates of erythromycin and clindamycin resistance among OBGYN isolates of group B Streptococcus. Diagn Microbiol Infect Dis;54:79–82 (2006)
Ono S, Muratani T and Matsumoto T. Mechanisms of resistance to imipenem and ampicillin in Enterococcus faecalis. Antimicrob Agents Chemother;49:2954–8 (2005)
Bonten MJ, Willems R and Weinstein RA. Vancomycin-resistant enterococci: why are they here, and where do they come from? Lancet Infect Dis;1:314–25 (2001)
Danchin MH, Rogers S, Kelpie L, et al. Burden of acute sore throat and group A streptococcal pharyngitis in school-aged children and their families in Australia. Pediatrics;120:950–7 (2007)
Veasy LG, Tani LY, Daly JA, et al. Temporal association of the appearance of mucoid strains of Streptococcus pyogenes with a continuing high incidence of rheumatic fever in Utah. Pediatrics; 113:e168–72 (2004)
Marijon E, Ou P, Celermajer DS, et al. Prevalence of rheumatic heart disease detected by echocardiographic screening. N Engl J Med;357:470–6 (2007)
McLaren MJ, Markowitz M and Gerber MA. Rheumatic heart disease in developing countries: the consequences of inadequate prevention. Ann Intern Med;120:243–5 (1994)
Ferguson GW, Shultz JM and Bisno AL. Epidemiology of acute rheumatic fever in a multiethnic, multiracial urban community: the Miami-Dade County experience. J Infect Dis;164:720–5 (1991)
Marcus RH, Sareli P, Pocock WA and Barlow JB. The spectrum of severe rheumatic mitral valve disease in a developing country. Ann Intern Med;120:177–83 (1994)
Sharkawy A, Low DE, Saginur R, et al. Severe group A streptococcal soft-tissue infections in Ontario: 1992–1996. Clin Infect Dis;34: 454–60 (2002)
Moses AE, Goldberg S, Korenman Z, Ravins M, Hanski E and Shapiro M. Invasive group A streptococcal infections, Israel. Emerg Infect Dis;8:421–6 (2002)
Patel RA, Binns HJ and Shulman ST. Reduction in pediatric hospitalizations for varicella-related invasive group A streptococcal infections in the varicella vaccine era. J Pediatr;144:68–74 (2004)
Kuusi M, Lahti E, Virolainen A, et al. An outbreak of Streptococcus equi subspecies zooepidemicus associated with consumption of fresh goat cheese. BMC Infect Dis;6:36 (2006)
Gray BM, Rodriguez Arnavielhe S. Streptococcus spp, in: International Handbook of Food Pathogens, (J Bier and MD Miliotis, eds.), pp. 375–405, Marcel Dekker, New York (2003)
Boyer KM, Gadzala CA, Burd LI, Fisher DE, Paton JB and Gotoff SP. Selective intrapartum chemoprophylaxis of neonatal group B streptococcal early-onset disease. I. Epidemiologic rationale. J Infect Dis;147:795–801 (1983)
Schrag SJ, Zell ER, Lynfield R, et al. A population-based comparison of strategies to prevent early-onset group B streptococcal disease in neonates. N Engl J Med;347:233–9 (2002)
Bertini G, Dani C, Cianciulli D, Rubaltelli FF and Nicoletti P. A trial of preventing early- and late-onset Group B streptococcal sepsis with combined intrapartum chemoprophylaxis and universal neonatal screening. J Perinat Med;34:420–4 (2006)
Trijbels-Smeulders M, de Jonge GA, Pasker-de Jong PC, et al. Epidemiology of neonatal group B streptococcal disease in the Netherlands before and after introduction of guidelines for prevention. Arch Dis Child Fetal Neonatal Ed;92:F271–6 (2007)
Gray KJ, Bennett SL, French N, Phiri AJ and Graham SM. Invasive group B streptococcal infection in infants, Malawi. Emerg Infect Dis;13:223–9 (2007)
Lin FY, Weisman LE, Troendle J and Adams K. Prematurity is the major risk factor for late-onset group B Streptococcus disease. J Infect Dis;188:267–71 (2003)
Berardi A, Lugli L, Baronciani D, et al. Group B streptococcal infections in a northern region of Italy. Pediatrics;120:e487–93 (2007)
Pass MA, Gray BM and Dillon HC, Jr. Puerperal and perinatal infections with group B streptococci. Am J Obstet Gynecol;143:147–52 (1982)
Locksmith GJ, Clark P and Duff P. Maternal and neonatal infection rates with three different protocols for prevention of group B streptococcal disease. Am J Obstet Gynecol;180:416–22 (1999)
Farley MM. Group B streptococcal disease in nonpregnant adults. Clin Infect Dis;33:556–61 (2001)
Edwards MS, Baker CJ. Group B streptococcal infections in elderly adults. Clin Infect Dis;41:839–47 (2005)
Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP and Edmond MB. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis;39:309–17 (2004)
Camins BC, Farley MM, Jernigan JJ, Ray SM, Steinberg JP and Blumberg HM. A population-based investigation of invasive vancomycin-resistant Enterococcus infection in metropolitan Atlanta, Georgia, and predictors of mortality. Infect Control Hosp Epidemiol;28:983–91 (2007)
Marthaler TM. Changes in dental caries 1953–2003. Caries Res;38:173–81 (2004)
Lewis DW, Ismail AI and Examination TCTFotPH. Periodic health examination, 1995 update: 2. prevention of dental caries. Can Med Assoc J;152:836–46 (1995)
Pine CM, Adair PM, Nicoll AD, et al. International comparisons of health inequalities in childhood dental caries. Community Dent Health;21:121–30 (2004)
Beltran-Aguilar ED, Barker LK, Canto MT, et al. Surveillance for dental caries, dental sealants, tooth retention, edentulism, and enamel fluorosis—United States, 1988–1994 and 1999–2002. MMWR Surveill Summ;54:1–43 (2005)
Leclercq MH, Barmes DE and Sardo Infirri J. Oral health: global trends and projections. World Health Stat Q;40:116–28 (1987)
Pitts NB. Modern concepts of caries measurement. Dent Res;83 Spec No C:C43–7 (2004)
Yabao RN, Duante CA, Velandria FV, et al. Prevalence of dental caries and sugar consumption among 6–12-y-old schoolchildren in La Trinidad, Benguet, Philippines. Eur J Clin Nutr;59:1429–38 (2005)
Cleaton-Jones P, Fatti P and Bonecker M. Dental caries trends in 5- to 6-year-old and 11- to 13-year-old children in three UNICEF designated regions—Sub Saharan Africa, Middle East and North Africa, Latin America and Caribbean: 1970–2004. Int Dent J;56:294–300 (2006)
Whelton H. Overview of the impact of changing global patterns of dental caries experience on caries clinical trials. J Dent Res;83 Spec No C:C29–34 (2004)
Ruiz Miravet A, Montiel Company JM and Almerich Silla JM. Evaluation of caries risk in a young adult population. Med Oral Patol Oral Cir Bucal;12:E412–8 (2007)
Daneman N, Green KA, Low DE, et al. Surveillance for hospital outbreaks of invasive group A streptococcal infections in Ontario, Canada, 1992 to 2000. Ann Intern Med;147:234–41 (2007)
Gunzenhauser JD, Longfield JN, Brundage JF, Kaplan EL, Miller RN and Brandt CA. Epidemic streptococcal disease among Army trainees, July 1989 through June 1991. J Infect Dis;172:124–31 (1995)
Brunton WAT. Infection and hospital laundry. Lancet;345:1574–5 (1995)
Petersen JP, Kaltoft MS, Misfeldt JC, Schumacher H and Schonheyder HC. Community outbreak of perianal group A streptococcal infection in Denmark. Pediatr Infect Dis J;22:105–9 (2003)
Wilson KS, Maroney SA and Gander RM. The family pet as an unlikely source of group A beta-hemolytic streptococcal infection in humans. Pediatr Infect Dis J;14:372–5 (1995)
Tanz RR, Shulman ST. Chronic pharyngeal carriage of group A streptococci. Pediatr Infect Dis J;26:175–6 (2007)
Muller AE, Oostvogel PM, Steegers EA and Dorr PJ. Morbidity related to maternal group B streptococcal infections. Acta Obstet Gynecol Scand;85:1027–37 (2006)
Pyati SP, Pildes RS, Jacobs NM, et al. Penicillin in infants weighing two kilograms or less with early-onset group B streptococcal disease. N Engl J Med;308:1383–9 (1983)
Hodges RG, MacLeod CM. Epidemic pneumococcal pneumonia. Am J Hyg;44:183–243 (1946)
Gray BM, Converse GM, III and Dillon HC, Jr. Epidemiologic studies of Streptococcus pneumoniae in infants: acquisition, carriage, and infection during the first 24 months of life. J Infect Dis;142:923–33 (1980)
Syrjanen RK, Auranen KJ, Leino TM, Kilpi TM and Makela PH. Pneumococcal acute otitis media in relation to pneumococcal nasopharyngeal carriage. Pediatr Infect Dis J;24:801–6 (2005)
Talbot TR, Poehling KA, Hartert TV, et al. Seasonality of invasive pneumococcal disease: temporal relation to documented influenza and respiratory syncytial viral circulation. Am J Med;118:285–91 (2005)
Greenwood B. Pneumococcal meningitis epidemics in Africa. Clin Infect Dis;43:701–3 (2006)
Martin JM, Green M, Barbadora KA and Wald ER. Group A streptococci among school-aged children: clinical characteristics and the carrier state. Pediatrics;114:1212–9 (2004)
Whitney CG, Farley MM, Hadler J, et al. Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugate vaccine. N Engl J Med;348:1737–46 (2003)
Musher DM. Pneumococcal vaccine—direct and indirect (“herd”) effects. N Engl J Med;354:1522–4 (2006)
Foxman B, Gillespie B, Manning SD, et al. Incidence and duration of group B Streptococcus by serotype among male and female college students living in a single dormitory. Am J Epidemiol;163:544–51 (2006)
Phillips G, Efstratiou A, Tanna A, Beall B, Ferguson J and Roworth M. An outbreak of skin sepsis in abattoir workers caused by an ‘unusual’ strain of Streptococcus pyogenes. J Med Microbiol;49: 371–4 (2000)
Bohnsack JF, Whiting AA, Martinez G, et al. Serotype III Streptococcus agalactiae from bovine milk and human neonatal infections. Emerg Infect Dis;10:1412–9 (2004)
Thigpen MC, Thomas DM, Gloss D, et al. Nursing home outbreak of invasive group A streptococcal infections caused by 2 distinct strains. Infect Control Hosp Epidemiol;28:68–74 (2007)
Nuorti JP, Butler JC, Crutcher JM, et al. An outbreak of multidrug-resistant pneumococcal pneumonia and bacteremia among unvaccinated nursing home residents. N Engl J Med;338:1861–8 (1998)
Crum NF, Russell KL, Kaplan EL, et al. Pneumonia outbreak associated with group A Streptococcus species at a military training facility. Clin Infect Dis;40:511–8 (2005)
Gray GC, Escamilla J, Hyams KC, Struewing JP, Kaplan EL and Tupponce AK. Hyperendemic Streptococcus pyogenes infection despite prophylaxis with penicillin G benzathine. N Engl J Med;325:92–7 (1991)
Price VE, Dutta S, Blanchette VS, et al. The prevention and treatment of bacterial infections in children with asplenia or hyposplenia: practice considerations at the Hospital for Sick Children, Toronto. Pediatr Blood Cancer;46:597–603 (2006)
Klugman KP, Madhi SA and Feldman C. HIV and pneumococcal disease. Curr Opin Infect Dis;20:11–5 (2007)
Snellman LW, Stang HJ, Stang JM, Johnson DR and Kaplan EL. Duration of positive throat cultures for group A streptococci after initiation of antibiotic therapy. Pediatrics;91:1166–70 (1993)
Kim PE, Musher DM, Glezen WP, Rodriguez-Barradas MC, Nahm WK and Wright CE. Association of invasive pneumococcal disease with season, atmospheric conditions, air pollution, and the isolation of respiratory viruses. Clin Infect Dis;22:100–6 (1996)
Byrne PA, Miller C and Justus K. Neonatal group B streptococcal infection related to breast milk. Breastfeed Med;1:263–70 (2006)
Koga T, Oho T, Shimazaki Y and Nakano Y. Immunization against dental caries. Vaccine;20:2027–44 (2002)
Stevens DL. Streptococcal toxic-shock syndrome: spectrum of disease, pathogenesis, and new concepts in treatment. Emerg Infect Dis;1:69–78 (1995)
Chuang YY, Huang YC and Lin TY. Toxic shock syndrome in children: epidemiology, pathogenesis, and management. Paediatr Drugs;7:11–25 (2005)
Henneke P, Berner R. SIRS and group-B streptococcal sepsis in newborns: pathogenesis and perspectives in adjunctive therapy. Semin Fetal Neonatal Med;11:333–42 (2006)
Soriani M, Santi I, Taddei A, Rappuoli R, Grandi G and Telford JL. Group B Streptococcus crosses human epithelial cells by a paracellular route. J Infect Dis;193:241–50 (2006)
Eriksson BK, Andersson J, Holm SE and Norgren M. Invasive group A streptococcal infections: T1M1 isolates expressing pyrogenic exotoxins A and B in combination with selective lack of toxin-neutralizing antibodies are associated with increased risk of streptococcal toxic shock syndrome. J Infect Dis;180:410–8 (1999)
Marsh PD. Are dental diseases examples of ecological catastrophes? Microbiology;149:279–94 (2003)
Baker CJ, Edwards MS and Kasper DL. Role of antibody to native type III polysaccharide of group B Streptococcus in infant infection. Pediatrics;68:544–9 (1981)
Lin FY, Philips JB, 3rd, Azimi PH, et al. Level of maternal antibody required to protect neonates against early-onset disease caused by group B Streptococcus type Ia: a multicenter, seroepidemiology study. J Infect Dis;184:1022–8 (2001)
Lin FY, Weisman LE, Azimi PH, et al. Level of maternal IgG anti-group B Streptococcus type III antibody correlated with protection of neonates against early-onset disease caused by this pathogen. J Infect Dis;190:928–34 (2004)
Davies HD, Adair C, McGeer A, et al. Antibodies to capsular polysaccharides of group B Streptococcus in pregnant Canadian women: relationship to colonization status and infection in the neonate. J Infect Dis;184:285–91 (2001)
Silver HM, Gibbs RS, Gray BM and Dillon HC. Risk factors for perinatal group B streptococcal disease after amniotic fluid colonization. Am J Obstet Gynecol;163:19–25 (1990)
Balmer P, Cant AJ and Borrow R. Anti-pneumococcal antibody titre measurement: what useful information does it yield? J Clin Pathol;60:345–50 (2007)
The_Working_Group_on_Severe_Streptococcal_Infections. Defining the group A streptococcal toxic shock syndrome. Rationale and consensus definition. Jama;269:390–1 (1993)
Special Writing Group of the committee on Rheumatic Fever E, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young of the American Heart Association. Guidelines for the diagnosis of rheumatic fever: Jones criteria, 1992 update. JAMA;268: 2069–73 (1992)
Colford JM, Mohle-Boetani J and Vosti KL. Group B streptococcal bacteremia in adults: five years’e experience and a review of the literature. Medicine;74:176–90 (1995)
Turner JC, Fox A, Fox K, et al. Role of group C beta-hemolytic streptococci in pharyngitis: epidemiologic study of clinical features associated with isolation of group C streptococci. J Clin Microbiol;31:808–11 (1993)
Lindbaek M, Hoiby EA, Lermark G, Steinsholt IM and Hjortdahl P. Clinical symptoms and signs in sore throat patients with large colony variant beta-haemolytic streptococci groups C or G versus group A. Br J Gen Pract;55:615–9 (2005)
Shulman ST, Gerber MA, Tanz RR and Markowitz M. Streptococcal pharyngitis: the case for penicillin therapy. Pediatr Infect Dis J;13: 1–7 (1994)
Tanz RR, Poncher JR, Corydon KE, Kabat K, Yogev R and Shulman ST. Clindamycin treatment of chronic pharyngeal carriage of Group A streptococci. J Pediatr;119:123–8 (1991)
Mahakit P, Vicente JG, Butt DI, Angeli G, Bansal S and Zambrano D. Oral clindamycin 300 mg BID compared with oral amoxicillin/clavulanic acid 1 g BID in the outpatient treatment of acute recurrent pharyngotonsillitis caused by group A beta-hemolytic streptococci: an international, multicenter, randomized, investigator-blinded, prospective trial in patients between the ages of 12 and 60 years. Clin Ther;28:99–109 (2006)
Lue HC, Wu MH, Wang JK, Wu FF and Wu YN. Three- versus four-week administration of benzathine penicillin G: effects on incidence of streptococcal infections and recurrences of rheumatic fever. Pediatrics;97:984–8 (1996)
Robertson KA, Volmink JA and Mayosi BM. Antibiotics for the primary prevention of acute rheumatic fever: a meta-analysis. BMC Cardiovasc Disord;5:11 (2005)
Berrios X, del Campo E, Guzman B and Bisno AL. Discontinuing rheumatic fever prophylaxis in selected adolescents and young adults. Ann Intern Med;118:401–6 (1993)
Shulman ST, Ayoub EM. Poststreptococcal reactive arthritis. Curr Opin Rheumatol;14:562–5 (2002)
Maddox JS, Ware JC and Dillon HC, Jr. The natural history of streptococcal skin infection: prevention with topical antibiotics. J Am Acad Dermatol;13:207–12 (1985)
Hood R, Shermock KM and Emerman C. A prospective, randomized pilot evaluation of topical triple antibiotic versus mupirocin for the prevention of uncomplicated soft tissue wound infection. Am J Emerg Med;22:1–3 (2004)
Smith A, Lamagni TL, Oliver I, Efstratiou A, George RC and Stuart JM. Invasive group A streptococcal disease: should close contacts routinely receive antibiotic prophylaxis? Lancet Infect Dis;5:494–500 (2005)
Paradise JL, Bluestone CD, Bachman RZ, et al. Efficacy of tonsillectomy for recurrent throat infection in severely affected children. Results of parallel randomized and nonrandomized clinical trials. N Engl J Med;310:674–83 (1984)
Westling K, Aufwerber E, Ekdahl C, et al. Swedish guidelines for diagnosis and treatment of infective endocarditis. Scand J Infect Dis;39:929–46 (2007)
No_author_listed. German guidelines for the diagnosis and management of infective endocarditis. Int J Antimicrob Agents;9:643–57 (2007)
Gould FK, Elliott TS, Foweraker J, et al. Guidelines for the prevention of endocarditis: report of the Working Party of the British Society for Antimicrobial Chemotherapy. J Antimicrob Chemother;57: 1035–42 (2006)
Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. (Simultaneously published in J Am Dent Assoc 138:739–45, 747–60 (2007). Circulation;116:1736–54 (2007)
Facchinetti F, Piccinini F, Mordini B and Volpe A. Chlorhexidine vaginal flushings versus systemic ampicillin in the prevention of vertical transmission of neonatal group B Streptococcus, at term. J Matern Fetal Neonatal Med;11:84–8 (2002)
Stade B, Shah V and Ohlsson A. Vaginal chlorhexidine during labour to prevent early-onset neonatal group B streptococcal infection. Cochrane Database Syst Rev:CD003520 (2004)
Orange JS, Hossny EM, Weiler CR, et al. Use of intravenous immunoglobulin in human disease: a review of evidence by members of the Primary Immunodeficiency Committee of the American Academy of Allergy, Asthma and Immunology. J Allergy Clin Immunol;117:S525–53 (2006)
Bisno AL, Rubin FA, Cleary PP and Dale JB. Prospects for a group A streptococcal vaccine: rationale, feasibility, and obstacles—report of a National Institute of Allergy and Infectious Diseases workshop. Clin Infect Dis;41:1150–6 (2005)
McNeil SA, Halperin SA, Langley JM, et al. Safety and immunogenicity of 26-valent group A Streptococcus vaccine in healthy adult volunteers. Clin Infect Dis;41:1114–22 (2005)
Guilherme L, Fae KC, Higa F, et al. Towards a vaccine against rheumatic fever. Clin Dev Immunol;13:125–32 (2006)
Olive C, Hsien K, Horvath A, et al. Protection against group A streptococcal infection by vaccination with self-adjuvanting lipid core M protein peptides. Vaccine;23:2298–303 (2005)
Terao Y, Okamoto S, Kataoka K, Hamada S and Kawabata S. Protective immunity against Streptococcus pyogenes challenge in mice after immunization with fibronectin-binding protein. J Infect Dis;192:2081–91 (2005)
Cleary PP, Matsuka YV, Huynh T, Lam H and Olmsted SB. Immunization with C5a peptidase from either group A or B streptococci enhances clearance of group A streptococci from intranasally infected mice. Vaccine;22:4332–41 (2004)
Paoletti LC, Madoff LC. Vaccines to prevent neonatal GBS infection. Semin Neonatol;7:315–23 (2002)
Sinha A, Lieu TA, Paoletti LC, Weinstein MC and Platt R. The projected health benefits of maternal group B streptococcal vaccination in the era of chemoprophylaxis. Vaccine;23:3187–95 (2005)
Johri AK, Paoletti LC, Glaser P, et al. Group B Streptococcus: global incidence and vaccine development. Nat Rev Microbiol;4:932–42 (2006)
Patten S, Vollman AR, Manning SD, Mucenski M, Vidakovich J and Davies HD. Vaccination for Group B Streptococcus during pregnancy: attitudes and concerns of women and health care providers. Soc Sci Med;63:347–58 (2006)
Musher DM, Rueda-Jaimes AM, Graviss EA and Rodriguez-Barradas MC. Effect of pneumococcal vaccination: a comparison of vaccination rates in patients with bacteremic and nonbacteremic pneumococcal pneumonia. Clin Infect Dis;43:1004–8 (2006)
Briles DE, Hollingshead SK, King J, et al. Immunization of humans with recombinant pneumococcal surface protein A (rPspA) elicits antibodies that passively protect mice from fatal infection with Streptococcus pneumoniae bearing heterologous PspA. J Infect Dis;182:1694–701 (2000)
Russell MW, Childers NK, Michalek SM, Smith DJ and Taubman MA. A caries vaccine? The state of the science of immunization against dental caries. Caries Res;38:230–5 (2004)
Matsubara K, Fukaya T. The role of superantigens of group A Streptococcus and Staphylococcus aureus in Kawasaki disease. Curr Opin Infect Dis;20:298–303 (2007)
US Bureau of the Census. Historical Statistics of the United States: Colonial Times to 1970, (Bicentennial ed.), Part I, p. 77, Government Printing Office, Washington, DC (1975)
National Office of Vital Statistics. Vital Stat Rep;37(9) (1920–1950)
Centers for Disease Control. MMWR; Annu Suppl (1960 and 1970)
Centers for Disease Control and Prevention. Prevention of perinatal group B streptococcal disease. MMWR;51(RR-11):8 (2002)
Suggested Reading
Stevens DL, Kaplan EL, eds. Streptococcal Infections, Oxford University Press, New York (2000)
Facklam RR, Carvalho MGS and Teixeira LM. History, taxonomy biochemical characteristics, and antibiotic susceptibility testing of enterococci, in: The Enterococci: Pathogenesis, Molecular Biology, and Antibiotic Resistance, (MS Gilmore, DB Clewell, P Couvalin, et al., eds.), pp. 1–54, American Society for Microbiology, Washington, DC (2002)
Gray BM, Musher DM. History of pneumococcal infections, in: Pneumococcal Vaccines: The Impact of Conjugate Vaccine, (GR Siber, et al., eds.), The American Society for Microbiology Press, Washington, DC (2008)
Fischetti VA, Novick RP, Ferretti JJ, Portnoy DA and Rood JI, eds. Gram-Positive Pathogens, 2nd ed., American Society for Microbiology, Washington, DC (2006)
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2009 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Gray, B.M., Stevens, D.L. (2009). Streptococcal Infections. In: Brachman, P., Abrutyn, E. (eds) Bacterial Infections of Humans. Springer, Boston, MA. https://doi.org/10.1007/978-0-387-09843-2_35
Download citation
DOI: https://doi.org/10.1007/978-0-387-09843-2_35
Published:
Publisher Name: Springer, Boston, MA
Print ISBN: 978-0-387-09842-5
Online ISBN: 978-0-387-09843-2
eBook Packages: MedicineMedicine (R0)