
Abstract
Influenza A(H1N1) is caused by the conflict of interest between giant organisms and microorganisms. Influenza A and B viruses are single stranded RNA envelope virus composed of 890–2,341 nucleic acids in eight segmented genomes. Presently, only the virus subtypes of H1N1 and H3N2 still spread from human to human. The viruses spread and replicate under the following conditions: (1) the viruses enter the human body and duplicate there; (2) the viruses cause diseases; and (3) the viruses can easily spread from person to person. The H1N1 influenza viruses replicate is within only respiratory epithelial cells. The virus entering into the cells causes complex pathological changes of the cells. The columnar epithelial cells stop the self-synthesis of cellular component proteins. Therefore, the cells die due to their lack of necessary cell component proteins.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
- Influenza Virus
- Severe Acute Respiratory Syndrome
- Severe Acute Respiratory Syndrome
- H1N1 Influenza Virus
- Human Influenza Virus
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Overview
Influenza A (H1N1) is caused by the conflict of interest between giant organisms and microorganisms. Influenza A and B viruses are single stranded RNA envelope virus composed of 890–2,341 nucleic acids in eight segmented genomes. Presently, only the virus subtypes of H1N1 and H3N2 still spread from human to human. The viruses spread and replicate under the following conditions: (1) the viruses enter the human body and duplicate there; (2) the viruses cause diseases; and (3) the viruses can easily spread from person to person. The H1N1 influenza viruses replicate is within only respiratory epithelial cells. The virus entering into the cells causes complex pathological changes of the cells. The columnar epithelial cells stop the self-synthesis of cellular component proteins. Therefore, the cells die due to their lack of necessary cell component proteins.
Influenza A (H1N1) spread from person to person by water duplets (>5 μm) coughed or sneezed out from the nose and throat of infected people. These particles cannot stay in the air, but spread the disease by contacts. The contacts can be direct skin contact or indirect respiratory secretions contact, the latter of which refers to touching his/her own eyes, nose or mouth with his/her own contaminated hands. The patients can spread the virus from 2 days prior to symptoms onset to fifth day after symptoms onset. The infection time of swine-origin influenza A virus (S-OIV) during its incubation period is about 2–7 days. According to data analysis, most patients infected by S-OIV may have their symptoms onset 1 day in advance, or 5–7 days after being infected. The infection period may be prolonged in immunocompromised children or patients with severe psychiatric disorders. It has been unknown whether a infected asymptomatic person is the source of infection, which deserves detailed research. Severe cases and death cases are mostly caused by the occurrence of its complications, including primary viral pneumonia and secondary bacterial pneumonia (especially group A streptococcus, Staphylococcus aureus and Streptococcus pneumoniae). Dyspnea, acute respiratory distress syndrome (ARDS) and multiple organs failure are fatal clinical signs of Influenza A (H1N1). The average period from symptoms onset to death is about 9 days.
Influenza A (H1N1) virus is particularly prone to virus variation. Based on the studies about the variation of Influenza A (H1N1) virus, it has been believed that the new human pathogenic mutant has completed its genetic fragments combination in the animal body before its direct invasion into human body. The genetic segments studies of influenza virus from the influenza pandemic in the year of 1918 found genes similar to swine and bird flu viruses. Therefore, it is believed that the influenza A pandemic in 1918 was caused by the integration of human influenza virus to a segment of DNA from swine influenza virus to form H1N1 influenza virus that is affinitive to human body. Based on the belief, experts speculate that the gene recombination of the bird flu virus with human flu virus would cause global influenza pandemic. Other scholars also put forward the theory of twice crossing and the model of birds → human → swine. In this model, the bird flu viruses spreading in poultry animals cross the species boundary to infect other animals, such as pigs, horses, whales or sables. Following the first crossing, the viruses cross the species boundary again to infect human. Some scholars insist on the theory of viruses genes mixer, namely the well-known quick infection of both human flu viruses and bird flu viruses to swine, and swine acts as a viruses genes mixer (to recombinate virus strains from two different species). Therefore, the swine flu virus containing human flu virus gene emerges, which can proliferate in human body and spread from person to person. WHO recommends the real-time quantitative RT-PCR to detect seasonal flu, including seral A, B, H1 genes, proteins H3 and bird flu H5 virus. Using probes and primers to detect A-H1N1 flu virus, nucleotide sequence analysis and systematic culture analysis, the infection of human MDCK cells by Influenza A (H1N1) virus can be confirmed. After reverse transcribed amplification sequencing and following PCR amplification production, the overlapping double-stranded DNA in influenza virus genome can be amplified. Genome degradation and sequence variation of about every 200–500 nucleotides cause prolonged existence of H1N1 influenza virus.
2 Clinical Manifestations
The incubation period of Influenza A (H1N1) viruses is usually about 7 days. The onset of Influenza A (H1N1) is acute, with its symptoms being similar to common influenza, including typical fever, general upset, muscular soreness and pain, sore throat, runny nose and cough, possible eye conjunctivitis, possible nausea, abdominal pain and diarrhea. The cases with persistent high body temperature should be given focused attention. According to the clinical review on 18 cases of S-OIV infection treated in a Mexico hospital, S-OIV infection is a serious illness associated with death. Most patients were previously healthy and suffered from pneumonia from day 5 to 7 after the onset of flu-liked symptoms. In them, seven patients were hospitalized at the day of clinic visit suffering from acute pulmonary impairment or acute respiratory distress. Multiple organs failure occurred in all the seven cases. S-OIV infection commonly occurs in the elderly and children and the ages of more than half of the patients range from 13 to 47 years. The age distribution of S-OIV is similar to that of Mexico influenza epidemic in 1918. Research data of Influenza A (H1N1) indicates that a large number of death is related to bacterial infection. However, the 14 cases with complicated bacterial infections out of 18 cases in Mexico review had no serious outcomes, which may be related to the early use of antibiotics before hospitalization.
3 Laboratory Tests
The etiological detections include isolating Influenza A (H1N1) virus from the respiratory secretions, or detecting H1N1 influenza virus A genes by RT-PCR, or detecting the serum antibodies and increased titer by laboratory tests. Most cases may have decreased white blood cells counts, but occasionally the white blood cells count may increase due to the secondary bacterial infection. Lymphocyte count commonly decreases, with normal count of platelets. Bone marrow puncture shows active cells proliferation, reactive histiocytosis with accompanying hemorrhagic phagocytosis. Patients may have increased ALT. Throat swabs is negative to bacterial culture. The most reliable laboratory evidence is the increased dehydrogenase. Increased lactic dehydrogenase usually indicates myocarditis.
4 Pathogenic Mechanism
The Influenza A (H1N1) virus is the primary cause of pulmonary impairments. The virus may directly impair the epithelial cells of respiratory tract. It can also target on alveoli to cause diffusive fibrosis of the pulmonary tissues and alveolar impairments of congestion, edema, surface exudation of viscous liquid, foam liked exudates in small bronchi and bronchioles and large amount of mixed serofibrin in chest cavity. The pathological examinations of two death cases in Hong Kong showed that the reactive hemophagocytic syndrome is histologically prominent. Other pathological findings include diffusive alveolar impairments with accompanying fibrosis, extensive hepatic centrilobular necrosis, acute renal tubular necrosis, lymphocytes function failure and increased levels of soluble IL-2 receptor, IL-6, γ-interferon. Therefore, it is believed that alveoli are the targets of Influenza A (H1N1) virus. It replicates in the respiratory tract and the high cytokines is produced by reactive hemophagocytic syndrome. The findings suggest that the pathogenic mechanism of Influenza A (H1N1) virus infection may be different from the infection of H1–H3 subtypes of human influenza viruses.
5 Diagnostic Imaging
Diagnostic imaging studies contribute to an objective assessment of pulmonary impairments and early diagnosis of their complications, which is of great importance to the prognosis of patients with Influenza A (H1N1) virus infection. According to overseas research, delayed treatment for patients with Influenza A (H1N1) virus infection may result in serious illness and even death. WHO announced that the global death rate of Influenza A (H1N1) virus infection is up to 6.4 %. Therefore, large scaled clinical research is necessary for understanding the pathological progression of Influenza A (H1N1) and its complications by data analysis of diagnostic imaging. The more knowledge about its pathological progression will facilitate the early diagnosis.
According to a report published by New England Journal of Medicine [1], X-ray of 18 cases of Influenza A (H1N1) had findings of alveolar exudation and fusion (commonly in the pulmonary basal segments) of both lungs, reticular or nodular shadows (interstitial exudation), parenchymal changes and occasional pleural effusions. The abnormal demonstrations usually occur in lower lungs, with alveolar exudation and fusion into blurring cloudy shadows, blurred costophrenic angle. The condition may further pathologically progress into large flaky dense parenchymal shadows. Also in this report, CT scanning found early manifestations of thickened pulmonary markings and punctiform exudates in the right lower pulmonary segment, infused mist liked lobular infiltration. Along with the progression of the condition, large flaky parenchymal shadows in the right lower pulmonary segment was found with involvement of the lung periphery, blurry upper boundary of the diaphragm, the blunt costophrenic angle, increased and blurry bilateral hili. CT scanning of the right lower lung found dense parenchymal shadows, visible lung tissues containing gas shadows with blurry boundaries. After treatment, the foci can be quickly absorbed. Most mild cases have favorable prognosis and for some cases, the disease progresses rapidly. With progressive development of pneumonia, respiratory distress syndrome, respiration failure, heart failure, kidney failure and infectious shock may occur to cause death.
6 Differential Diagnosis
In clinical diagnosis, Influenza A (H1N1) should be differentiated from influenza, the common cold, bacterial pneumonia, the infectious severe acute respiratory syndrome (SARS), the infectious mononucleosis, cytomegalovirus infection, chlamydia pneumonia and the mycoplasma pneumonia.
Generally speaking, the confirmative diagnosis technology for Influenza A (H1N1) is well-developed. The Influenza A (H1N1) virus spreads through the respiratory tract, targeting on alveoli and causing diffusive fibrosis of pulmonary tissues and alveolar impairments. There are alveolar edema, large amounts of lobular inflammatory exudation and fusion. The diagnostic imaging demonstrates flacky blurry shadows. With the progression of the disease, the pulmonary interstitial tissues are involved with decreased gas content in alveoli. Parenchymal changes and fibrosis of pulmonary tissues occur. The diagnostic imaging demonstrates large flaky dense shadows, with blurry surrounding tissues. Based on the diagnostic imaging studies about the pathological progression of Influenza A (H1N1) complicated pulmonary diseases, large scale clinical studies have not been conducted both domestically and internationally. Such research field is still blank domestically. Detailed research in such a field will be beneficial to clinical observation and objective assessment of the progression of Influenza A (H1N1). Therefore, effective control and mortality decrease can be realized. In other words, it is of great significance in improving public health of human being.
7 Cases Reports
Case 11.1
History of Present Illness. A 14-years-old female, with a foreign nationality. She complained of fever and cough for 2 days, with chills, shivers, sore throat and slight cough.
Past History. Not found.
Contact History. Have a history of contact to patients with Influenza A (H1N1).
Signs. Body temperature 38.7 °C. Pharynx congestion and tonsillar enlargement of I degree.
Laboratory Tests
On Nov. 8th, 2009, Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
Routine blood tests found white blood cells count 5.7 × 109/L, lymphocytes 40.3 %, neutrophils 42.1 %.
Diagnostic Imaging. On July 20th, 2009 (Fig. 11.1): chest X-ray demonstrated large flaky blurry shadows in the right middle-superior lung, cloud-mist liked blurry shadows in the left middle-superior lung fields, enlarged and blurry pulmonary hilum.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.1
Case 11.2
Case History. An 8-years-old boy, with a foreign nationality. He complained of fever and slight cough for 3 days, with no chills and fatigue.
Past History. Not found.
Epidemiological History. He was from the epidemic area of Influenza A (H1N1).
Signs. Body temperature 39 °C. Pharynx congestion and tonsillar enlargement of I degree.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests, white blood cells count 5.3 × 109/L, lymphocytes 53.5 %, and neutrophils 34.5 %.
Diagnostic Imaging. On June 25th, 2009 (Fig. 11.2): chest X-ray demonstrated thickened pulmonary markings, flaky and flocky shadows with blurry boundaries, enlarged and thickened pulmonary hilus.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.2
Case 11.3
History of Present Illness. A 12-years-old boy complained of fever for 3 days, with chills and fatigue.
Past History. Not found.
Contact History. The boy had a contact history to patients with Influenza A (H1N1) and he came from the epidemic area of Influenza A (H1N1).
Signs. Body temperature 39.1 °C. Throat red and tonsils no enlarged.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus negative.
By routine blood tests on June 15th, 2009, white blood cells count 4.1 × 109/L, lymphocytes 62.1 % and neutrophils 26.6 %.
By routine blood tests on June 18th, 2009, white blood cells count 5.5 × 109/L, lymphocytes 50.2 % and neutrophils 41.2 %.
Diagnostic Imaging
On June 14th, 2009 (Fig. 11.3a): chest X-ray demonstrated increased and deranged pulmonary markings with punctiform blurry shadows, increased and thickened pulmonary hilus.
On June 15th, 2009 (Fig. 11.3b): chest X-ray demonstrated slightly thickened pulmonary markings of both lungs, no other abnormal density shadows in both lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.3
Case 11.4
History of Present Illness. A 6-years-old girl complained of dry cough and fever for 3 days, with sore throat but no chills, cough, and headache.
Past History. Not found.
Contact History. She had a contact history to patients with Influenza A (H1N1).
Signs. Body temperature 38.3 °C. Pharynx congestion and tonsillar enlargement of I degree.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests, white blood cells count 17.0 × 109/L and neutrophils 95.44 %.
By blood gas analysis, pH 7.395, Pace2 44.6 mmHg (1 mmHg = 0.133 kPa), and PaO2 53.3 mmHg.
By routine blood tests on Nov. 9th, 2009, white blood cells count 13.8 × 109/L and neutrophils 96 %. And by blood gas analysis, pH 7.492, Pace2 39.5 mmHg and PaO2 44.6 mmHg.
By routine blood tests on Nov. 11th, 2009, white blood cells count 4.13 × 109/L, lymphocytes 44.6 % and neutrophils 31.8 %. By blood gas analysis, pH 7.406, Pace2 43.4 mmHg and PaO2 73.9 mmHg.
Diagnostic Imaging
On Nov. 9th, 2009 (Fig. 11.4a): chest X-ray demonstrated stripped and flaky shadows in both lung fields, with blurry boundaries; enlarged and thickened pulmonary hilum.
On Nov. 12th, 2009 (Fig. 11.4b): chest X-ray demonstrated stripped and small flaky shadows in both lung fields, with the sizes obviously decreased.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.4
Case 11.5
History of Present Illness A 2-years-old girl complained of fever and cough with runny nose for 1 day, occasionally with tasteless thin white sputum.
Past History. Not found.
Contact History. Not collected.
Signs. Body temperature 39 °C. Throat negative.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus negative.
By routine blood tests, white blood cells count 11.2 × 109/L, lymphocytes 65.4 % and neutrophils 23.8 %.
Diagnostic Imaging
On Oct. 13th, 2009 (Fig. 11.5a): chest X-ray demonstrated enhanced pulmonary markings of both lungs, punctiform blurry shadows of both lungs, enlarged and thickened pulmonary hilum.
On Oct. 19th, 2009 (Fig. 11.5b): chest X-ray demonstrated clear pulmonary markings of both lungs, no abnormal density shadows in both lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.5
Case 11.6
History of Present Illness. A 5-years-old boy complained of fever and cough with sputum, with no chills and shivers but with accompanying general fatigue, muscular soreness and pain, poor appetite.
Past History. No related past history was found.
Contact History. He denied the contact history with Influenza A (H1N1) patients.
Signs. The child is conscious with poor spirituality. He has dyspnea, nasal flaring and frequent rales of both lungs. His breathing rate 40 times/min, heart rate 130 beats/min and a body temperature 39 °C.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests, white blood cells count 1.9 × 109/L, PLT 87 × 109/L, neutrophils 60.9 %, ALT 13.2 U/L and AST 30.9 U/L.
His blood oxygen saturation 79–85 %, heart rate 137 beats/min, blood pressure 96/50 mmHg and breathing rate 50 times/min.
Diagnostic Imaging. On Nov. 12th, 2009 (Fig. 11.6a): chest X-ray demonstrated diffusive dense blurry shadows of both lungs, unclearly defined pulmonary hilum and blurry upper boundary of diaphragm.
Diagnosis. Pneumonia complicating Influenza A (H1N1).
Histopathological Analysis. Figure 11.6b, c demonstrated intraalveolar bleeding and inflammatory cells infiltration.

Fig. 11.6
Case 11.7
History of Present Illness. A 8-years-old boy, a primary school student, complained of fever, cough and being out of breath for 2 days. The fever had no obvious incentives with a body temperature up to 39 °C. The fever showed no regularity, and the cough paroxysmal with a few yellowish thick phlegm, and accompanying out of breath, shortness of breath and chest distress. The boy also suffered from difficulty swallowing and occasional abdominal pain, which was obvious during coughs, especially at periumbilical area.
Past History. The boy was diagnosed as having asthma at the age of 3 years. He has twice episodes of asthma, with favorable outcomes after treatment. His mother had a history of asthma.
Contact History. The boy had a contact history with suspected cases of fever. Had a contact history with Influenza A (H1N1) patients. There were several definitive cases of Influenza A (H1N1) in the school he was studying in.
Signs. Body temperature 37.9 °C, heart rate 117 beats/min, breathing rate 33 times/min, blood pressure 105/60 mmHg. His lips no cyanosis and pharynx obviously congested. The posterior wall of pharynx without follicles hyperplasia and no leukoplakia. Both antiadoncus to II degrees. Auscultation of both lungs found occasional fine moist rales and wheezing sound.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests, Hb 118 g/L, white blood cells count 6.69 × 109/L, neutrophils 78.1 %, lymphocytes 12.7 % and mononuclear cells 7 %. By blood biochemistry, CK 2022.5 U/L, CK-MB 35.1 U/L, AST 52.5 U/L, muscle calcium protein 1.08 ng/mL, CD3+T lymphocytes 332/μL, CD4+T lymphocytes 173/μL, CD8+T lymphocytes 106/μL and CD4+/CD8+ 1.64.
By blood gas analysis, pH 7.4, Pace2 35.7 mmHg, PaO2 109 mmHg, AB 21.6 mmol/L and BE −3.7 mmol/L.
Diagnostic Imaging
On Nov. 11th, 2009 (Fig. 11.7a): chest X-ray demonstrated increased pulmonary markings of both lungs, diffusive flaky dense shadows with blurry boundaries in the left middle-inferior lung.
On Nov. 12th, 2009 (Fig. 11.7b–e): chest X-ray demonstrated flaky dense foci in the left lower lung, dense shadows with blurry boundaries, increased and thickened pulmonary hilum.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.7
Case 11.8
History of Present Illness. A 10-years-old girl, with chief complaints of dry cough and mild cough.
Past History. No related past illnesses.
Contact History. She had a history of contact with Influenza A (H1N1) patients.
Signs. Pharyngeal congestion, with no enlargement of tonsils.
Laboratory Tests
By throat swabs, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Aug. 3rd, 2009, leukocyte count 5.1 × 109/L, lymphocyte 41.7 % and neutrophil 43.2 %.
Diagnostic Imaging
On July 29th, 2009 (Fig. 11.8): chest X-ray demonstrated flaky blurry dense shadows in both lungs, blurry structure of both pulmonary hilum.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.8
Case 11.9
History of Present Illness. A 10-years-old boy complained of fever for 3 days, with slight cough with no sputum, vomiting, no chills and fatigue.
Past History. No related illnesses in the past.
Contact History. He had a history of contact with Influenza A (H1N1) patients.
Signs. Body temperature 39 °C, pharynx congestion, tonsillar enlargement of I degree.
Laboratory Tests
By throat swabs, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 1st, 2009, leukocyte count 13.39 × 109/L, neutrophil 84.1 %.
By routine blood tests on Nov. 10th, 2009, leukocyte count 7.62 × 109/L, lymphocyte 7.6 % and neutrophil 90.7 %.
By routine blood tests on Nov. 11th, 2009, leukocyte count 4.68 × 109/L, lymphocyte 22.2 % and neutrophil 67.1 %.
By routine blood tests on Nov. 14th, 2009, leukocyte count 7.36 × 109/L, lymphocyte 17.8 % and neutrophil 70.3 %.
Diagnostic Imaging
On Oct. 31st, 2009 (Fig. 11.9a): chest X-ray demonstrated diffusive flocculent shadows in both lungs, decreased transparency of both lungs, and blurry structure of both pulmonary hila.
On Nov. 1st, 2009 (Fig. 11.9b): chest X-ray demonstrated cloud-mist liked blurry dense shadows of both lungs and further decreased transparency of both lungs.
On Nov. 3rd, 2009 (Fig. 11.9c): chest X-ray demonstrated blurry pulmonary markings of both lungs, commonly increased density within both lungs, and generally the same conditions with previous imaging results.
On Nov. 5th, 2009 (Fig. 11.9d): chest X-ray demonstrated blurry pulmonary markings of both lungs, diffusive spotty shadows in both lungs, decreased transparency of both lungs and the conditions progressed compared to the previous imaging results.
On Nov. 7th, 2009 (Fig. 11.9e): chest X-ray demonstrated blurry pulmonary markings of both lungs, almost the same as the previous imaging results.
On Nov. 10th, 2009 (Fig. 11.9f): chest X-ray demonstrated increased pulmonary markings of both lungs, blurry pulmonary markings of the right lower lung, and improved conditions compared to the previous imaging findings.
On Nov. 17th, 2009 (Fig. 11.9g): chest X-ray demonstrated no obvious abnormities in cardiopulmonary diaphragm.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.9
Case 11.10
History of Present Illness. A 6-years-old boy complained of fever and cough for 6 days and worsened fever and cough for 3 days. The body temperature 38.9 °C with dry cough. Six days ago, his clinic visit was for acute urticaria. The high fever still persisted after rashes healed. He coughed with sputum but with difficulty coughing up, with accompanying shortness of breath. During inspiration, three depression sign occurred.
Past History. None related to the present illness.
Contact History. He had a history of contact with Influenza A (H1N1) patients.
Signs. Throat red and swollen, with moist rale and occasional wheezing sound by auscultation of both lungs.
Laboratory Tests
By throat swabs, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By blood gas analysis on Nov. 21st, 2009, pH 7.448, PaCO2 42.6 mmHg, PaO2 86.5 mmHg. By liver function tests, AST 42.4 U/L, LDH 323.4 U/L, HBDH 239.2 U/L and CK 197 U/L. By ECG, sinus arrhythmia, unspecific ST elevation, borderline ECG.
By blood gas analysis on Nov. 23rd, 2009, pH 7.434, PaCO2 43 mmHg, PaO2 89.1 mmHg. By liver function tests, AST 32.4 U/L, LDH 230.3 U/L, HBDH 192.6 U/L and CK 36.4 U/L.
Diagnostic Imaging
On Oct. 21st, 2009 (Fig. 11.10a): chest X-ray demonstrated blurry pulmonary markings with flaky blurry shadows of both lungs, being more obvious in the right lungs.
On Oct. 23rd, 2009 (Fig. 11.10b): chest X-ray demonstrated blurry pulmonary markings and improved conditions than previous imaging results.
On Oct. 26th, 2009 (Fig. 11.10c): chest X-ray demonstrated normal lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.10
Case 11.11
History of Present Illness. A 13-years-old boy complained of fever and cough for 1 day. The patient self reported fever without obvious causes since Nov. 8th, 2009. The highest body temperature reached 38.1 °C, irregular fever, with accompanying headache and fatigue. No chills, but with paroxysmal cough, chest distress palpitation and dyspnea.
Past History. None related to the present illness.
Contact History. He had a history of contact to suspected cases of fever. The school he was studying in had some students with fever, being classified into social onset. A few of the students with fever were definitively diagnosed as having Influenza A (H1N1).
Signs. Body temperature 37.8 °C, heart rate 120 beats/min, breathing rate 22 times/min, blood pressure 118/72 mmHg. No lips cyanosis. Pharynx slight congestion slightly, swollen tonsils of I degree with no abscess.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 9th, 2009, hemoglobin 142.9 g/L, leukocyte count 7.6 × 109/L, neutrophils 66.1 %, lymphocyte 14.7 %, mononuclear cells 13.9 % and eosinophil 1.2 %. By blood gas analysis, pH 7.42, PaCO2 32.4 mmHg, PaO2 80.6 mmHg, AB 20.5 mmHg, BE -4.00 mmol/L. By ECG, sinus heart rate, right axis deviation and slight ST-T changes.
Diagnostic Imaging
On Nov. 9th, 2009 (Fig. 11.11a): chest X-ray demonstrated increased and blurry pulmonary markings of the left lower lung, flaky dense shadows with blurry boundaries.
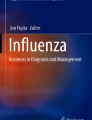
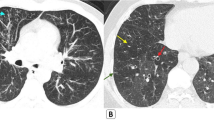
On Nov. 9th, 2009 (Fig. 11.11b–d): CT scanning demonstrated ground glass liked shadows in both lower lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.11
Case 11.12
History of Present Illness. A 10-years-old boy complained of cough, spasmodic breathing with accompanying fever, sore throat and headache for 3 days.
Past History. He was diagnosed as having bronchial asthma 4 years ago.
Contact History. He had a history of contact with Influenza A (H1N1) patients.
Signs. Pharyngeal congestion obvious, body temperature 37.7 °C, heart rate 156 beats/min, blood pressure 135/65 mmHg. Slow reaction, slight irritation, tachypnea, slight cyanosis on face and lips.
Nasal flaring and three depressions sign positive, coarse breathing sounds, occasional wheezing, and fine bubbling from the right side.
Laboratory Tests
By throat swabs, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 30th, 2009, leukocyte count 7.77 × 109/L, neutrophils 91.4 % and lymphocyte 5.5 %.
By blood gas analysis, pH 7.306, PaCO2 49.9 mmHg, PaO2 51.9 mmHg, \( {\text{HCO}}_{3}^{-}\) 24.2 mmol/L, BE 1.3 mmol/L, myocardial enzyme spectrum CK 1,591 U/L with obvious increase.
By blood biochemistry, K+ 3.7 mmol/L, Na+ 132 mmol/L, free Ca2+ 1.15 mmol/L, Cl− 109 mmol/L, blood glucose 9.2 mmol/L, CPR 20 mg/L, mechanical ventilation.
Diagnostic Imaging
On Oct. 30th, 2009 (Fig. 11.12): chest X-ray demonstrated small flaky shadows with uneven densities in the left upper lung, the shadows connecting to the upmost of the left pulmonary hilum, increased density of the left pulmonary hilum, thickened and increased pulmonary markings of both lungs that were blurry, occasional reticular shadows of both lungs and slightly increased transparency of both lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.12
Case 11.13
History of Present Illness. A 10-years-old boy complained of fever for 30 h without obvious causes, with accompanying nausea.
Past History. None related to present illness.
Contact History. He had a history of contact with Influenza A (H1N1) patients.
Signs. Body temperature 39 °C, heart rate 138 beats/min, blood pressure 129/75 mmHg. Respiratory sounds of lungs weak, with occasional fine moist rales. Three depressions sign positive, with no cyanosis.
Laboratory Tests
By throat swabs, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests, leukocyte count 10.20 × 109/L, neutrophils 93.3 %, lymphocyte 5.6 %, hemoglobin 147 g/L, CPR 47 mg/L.
By blood gas analysis, pH 7.45, PaCO2 37.2 mmHg, PaO2 57 mmHg, \( {\text{HCO}}_{3}^{-}\) 26.1 mmol/L and BE 2 mmol/L.
By blood biochemistry, K+ 4.8 mmol/L, Na+ 132 mmol/L, Ca2+ 1.13 mmol/L, blood glucose 7.3 mol/L, with improvement after mechanical ventilation.
Diagnostic Imaging. On Oct. 26th, 2009 (Fig. 11.13): the diagnostic imaging demonstrated obviously thickened pulmonary markings of both lungs, with accompanying flaky shadows, enlarged and thickened pulmonary hilum.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.13
Case 11.14
History of Present Illness. A 6-years-old boy with acute onset and quick progression. He complained of fever, cough, headache, vomiting, dyspnea; being unable to lie on his back, with unconsciousness and no responses to verbal commands.
Past History. None related to the present illness.
Contact History. He had a history of contact with Influenza A (H1N1) patients.
Signs. Shallow and short breathing, slight cyanosis on face and lips. Throat congestion. The pupils in the same size with slight sluggish reaction to light. Three depressions sign positive. Respiratory sounds of both lungs coarse, with weaker respiration sounds of the left lung and wheezing, dry and moist rales of both lungs. Body temperature 38.2 °C, heart rate 178 beats/min, blood pressure 150/76 mmHg.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests, leukocyte count 28.85 × 109/L, neutrophils 86 %, lymphocytes 6.6 %, hemoglobin 119 g/L.
By blood gas analysis, PaCO2 66.4 mmHg, PaO2 33.1 mmHg, \( {\text{HCO}}_{3}^{-}\) 20.4 mmol/L and BE 7.7 mmol/L.
By blood biochemistry, K+ 4.9 mmol/L, Na+ 129 mmol/L, Ca2+ 1.26 mmol/L and blood glucose 8.6 mol/L.
Diagnostic Imaging
On Oct. 24th, 2009 (Fig. 11.14a): chest X-ray demonstrated irregular patchy shadows with slightly higher density in the left intrapulmonary strip, with blurry boundaries and partially undisplayed heart margin and mediastinum. Increased pulmonary markings in the right intrapulmonary strip and the right pulmonary hilum. Occasional granular reticular shadows in the right pulmonary inner-middle strip. Increased transparency of both lungs. Blunt diaphragmatic angle.
On Oct. 24th, 2009 (Fig. 11.14b): chest X-ray demonstrated increased size of foci in the left intrapulmonary strip. Further increased transparency of both lungs, further obvious granular reticular shadows, blunt diaphragmatic angle. The bottom of trachea intubation at the level of T4.
On Oct. 25th, 2009 (Fig. 11.14c): chest X-ray demonstrated decreased size of patchy shadows in the inner strip of the left middle-lower lung. Not obvious change of foci in the left upper lung. Further increased transparency of both lungs. No changes of granular reticular shadows. The diaphragmatic angle had a small liquid level.
On Oct. 27th, 2009 (Fig. 11.14d): chest X-ray demonstrated absorbed foci in the inner strip of left middle-lower lung, decreased lesion area in the left upper lung.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.14
Case 11.15
History of Present Illness. A 14-years-old boy complained of recurrent fever, cough and runny nose for 15 days. Body temperature 39.1 °C, with chills, cough and occasional yellowish thick sputum or slight yellowish mucoid sputum. Nasal mucus clear and fatigue.
Past History. None related to the present illness.
Contact History. He had a history of contact with Influenza A (H1N1) patients.
Signs. Body temperature 36.9 °C, heart rate 100 beats/min, breathing rate 22 times/min and blood pressure 118/88 mmHg. Pharynx obviously congested. The posterior wall of pharynx had follicles hyperplasia. The right tonsil swollen to II degrees. Coarse respiration sounds of both lungs. Occasional moist rales in the right lower lung with rare wheezing rales.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 3rd, 2009, hemoglobin 130.3 g/L, leukocyte count 26.03 × 109/L, erythrocyte count 4.67 × 1012/L, neutrophils 75.9 %, lymphocytes 14.30 % and mononuclear cells 7.5 %.
Diagnostic Imaging
On Nov. 3rd, 2009 (Fig. 11.15a, b): chest X-ray demonstrated small patchy light shadows in the right lower lung, with blurry boundaries. Enhanced and deranged pulmonary markings of both lungs. Enlarged and thickened pulmonary hili of both lungs.
On Nov. 3rd, 2009 (Fig. 11.15c–f): chest CT scanning demonstrated patchy foci with high density in the right lower lung, with unclear boundaries.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.15
Case 11.16
History of Present Illness. A 2-years-old girl with chief complaints of fever for 6 days and accompanying chills.
Past History. None related to the present illness.
Contact History. The patient denied any contact with Influenza A (H1N1) patients.
Signs. Body temperature 39.8 °C. Pharyngeal congestion. No swollen tonsils.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 8th, 2009, leukocyte count 0.6 × 109/L and neutrophils 30 %.
By routine blood tests on Nov. 9th, 2009, leukocyte count 1.01 × 109/L, lymphocytes 73.3 % and neutrophils13.8 %.
By routine blood tests on Nov. 10th, 2009, leukocyte count 1.06 × 109/L, lymphocytes 41.5 % and neutrophils 43.4 %.
By routine blood tests on Nov. 11th, 2009, leukocyte count 1.63 × 109/L, lymphocytes 49.1 % and neutrophils 35.6 %.
Blood was transfused to increase leukocyte.
By routine blood tests on Nov. 12th, 2009, leukocyte count 10.93 × 109/L, lymphocytes 21.3 % and neutrophils 45.4 %.
By routine blood tests on Nov. 13th, 2009, leukocyte count 14.06 × 109/L, lymphocytes 15.5 % and neutrophils 62.8 %.
Diagnostic Imaging. On Nov. 10th, 2009 (Fig. 11.16): chest X-ray demonstrated blurry pulmonary marking of both lungs, small spotty shadows distributing along with pulmonary markings of both lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.16
Case 11.17
History of Present Illness. A 9-years-old boy complained of fever, cough and sore throat for 4 days. His highest body temperature 38 °C, with irregular temperature changes. Coughs paroxysmal, with more yellowish thick phlegm. Sore throat, with foreign body sensation during swallowings. The body temperature 40 °C on the next day.
Past History. None related to the present illness.
Contact History. He had a history of contact to fever liked cases. Several fever cases occurred in the school he was studying in and three were definitively diagnosed as having Influenza A (H1N1).
Signs. Body temperature 36.5 °C, heart rate 120 beats/min, breathing rate 20 times/min, blood pressure 117/73 mmHg. No lips cyanosis. Pharyngeal congestion obvious. No follicles hyperplasia on the posterior wall of pharynx. No leukoplakia. The left tonsil swollen of II degrees and the right tonsil swollen of III degrees, with no pus. No abnormalities in heart, lungs, abdomen and the nervous system.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 13th, 2009, Hb 114.3 g/L, leukocyte count 8.0 × 109/L, neutrophils 63.9 % and lymphocytes 16.9 %.
By blood gas analysis, pH 7.42, PaCO2 41.40 mmHg, PaO2 83.50 mmHg, AB 26.30 mmol/L and BE 1.90 mmol/L.
By routine blood tests on Nov. 15th, 2009, Hb 115.5 g/L, leukocyte count 5.63 × 109/L, neutrophils 46.5 % and lymphocytes 41.2 %.
Diagnostic Imaging
On Nov. 13th, 2009 (Fig. 11.17): chest X-ray demonstrated flaky light thin shadows in the right lower lung. Enhanced and thickened pulmonary markings of both lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.17
Case 11.18
History of Present Illness. A 7-months-old boy with complaints of fever and cough for 2 days. Body temperature 39.2 °C, with coughing up phlegm and runny nose.
Past History. None related to the present illness.
Contact History. He had a history of fever.
Signs. Pharyngeal congestion, with no tonsillar enlargement. Moist rale in both lungs.
Laboratory Tests
By throat swabs on Oct. 27th, 2009, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
Liver function tests on Oct. 31st, 2009, ALT 81.3 U/L and AST 166.6 U/L.
By routine blood tests, leukocyte count 4.5 × 109/L and lymphocytes 67 %.
Diagnostic Imaging. On Nov. 1st, 2009 (Fig. 11.18): chest X-ray demonstrated blurry cloud-mist liked shadows with increased density of both lungs, with enlarged and thickened pulmonary hila.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.18
Case 11.19
History of Present Illness. A 3-years-old boy with chief complaints of fever, cough and shortness of breath for 6 days. He suffered from fever 6 days ago, with accompanying cough, sputum and shortness of breath after activities. In the local hospital, he was diagnosed as tonsillitis and received double coptis chinensis for 1 day. He still had fever, cough, more severe shortness of breath and dyspnea. On d 6, throat swabs found Influenza A (H1N1) positive and the patient was transferred to You’an Hospital in Beijing.
Past History. None related to the present illness.
Contact History. Several children had fever in the kindergarten he was studying in.
Signs. Body temperature 39 °C, Pharyngeal congestion, with tonsils swollen to I degree. Shortness of breath, coarse respiration sound of both lungs, fine moist rale in the left lower lung, frequent wheezing in the right lung. Heart beats 118/min, palpable liver at 1 cm below the rib.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 12th, 2009, leukocyte count 11.58 × 109/L, neutrophils 71.97 % and lymphocytes 19.24 %.
By routine blood tests on Nov. 14th, 2009, leukocyte count 9.73 × 109/L, neutrophils 30.64 % and lymphocytes 31.14 %.
By blood biochemistry on Nov. 14th, 2009, TP 70 g/L, A 32 g/L, AST 42 U/L, ALT 21 U/L. BUN within normal limits. Uric acid 173 μmol/L, electrolyte Na+ 133 mmol/L, Cl− 97 mmol/L, Ca2+ 2.41 mmol/L, ALP 147 U/L, cholinesterase within normal limits, CK within normal limits and LDH 274 U/L.
By routine blood tests on Nov. 17th, 2009, leukocyte count 8.2 × 109/L, neutrophils 36.14 % and lymphocytes 23.44 %.
By blood biochemistry on Nov. 17th, 2009, TP 81 g/L, A 35 g/L, AST 42 U/L, ALT 54 U/L, BUN 2.9 mmol/L, Cr 43 μmol/L, uric acid 190 μmol/L, electrolyte Na+ within normal limits, Na+ 126 mmol/L, Cl− 91 mmol/L, Ca2+ 1.952 mmol/L, cholinesterase within normal limits, CK 63 U/L and LDH 289 U/L.
By HBV-M, HBsAb (+), HBcAb (+); HCVAb (−), HIVAb (−), HIVIgM (−), syphilis (−).
Diagnostic Imaging. On Nov. 13th, 2009 (Fig. 11.19): chest X-ray demonstrated large flaky blurry shadows with increased density in the right lower lung, enlarged and thickened hilum, increased and thickened pulmonary markings.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.19
Case 11.20
History of Present Illness. A 2.5-years-old boy with chief complaints of fever and cough for 8 days. He suffered from fever and cough 8 days ago. In a nearby clinic, the cephalosporin antibiotics and double coptis chinensis were administered for 2 days with no improved conditions. He had a poor appetite, aggravated cough, poor spirituality and erosive mouth corners. He was suspected as having measles and transferred to You’an Hospital in Beijing.
Past History. None related to present illness.
Contact History. No definitive contact to Influenza A (H1N1) patients.
Signs. Body temperature 38.7 °C. Mouth corners erosive and scattered spotty leukoplakia on oral mucosa. The respiration sound coarse, with frequent moist rales. Heartbeat 130/min.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Dec. 15th, 2009, leukocyte count 1.5 × 109/L, neutrophils 47.34 %, lymphocytes 41.3 %, erythrocyte count 5.03 × 1012/L and Hb 130 g/L.
By blood biochemistry on Dec. 15th, 2009, TP 50 g/L, A 24 g/L, ALT 32 U/L, AST 143 U/L, BUN 7.6 mmol/L, Cr 61 μmol/L, uric acid 357 μmol/L, electrolyte within normal limits, Cl− 91 mmol/L, Ca2+ 1.952 mmol/L, alkaline phosphatase 153 U/L, cholinesterase within normal limits, CK 63 U/L and LDH 289 U/L.
By HBV-M, HBsAb (+), HBcAb (+), HCVAb (−), HAVIgM (−), HIVAb (−), syphilis (−).
Diagnostic Imaging
On Nov. 11th, 2009 (Fig. 11.20a): chest X-ray demonstrated flaky blurry shadows of both lungs, with increased and thickened pulmonary markings.
On Nov. 11th, 2009 (Fig. 11.20b–l): chest CT scanning demonstrated large flaky blurry parenchymal shadows of both lungs, mostly in basal posterior segments with uneven densities. The shadows had air bronchogram. Bilateral pleura unsmooth.
Diagnosis. Pneumonia complicating Influenza A (H1N1).



Fig. 11.20
Case 11.21
History of Present Illness. A 6-years-old boy with chief complaints of fever and cough with wheezing for 2 days. He also had dry cough and fatigue.
Past History. None related to the present illness.
Contact History. He denied contacts with Influenza A (H1N1) patients.
Signs. Body temperature 39.4 °C. Pharyngeal congestion. Tonsils swollen of II degree.
Laboratory Tests
By throat swabs, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests, on Nov. 3rd, 2009, leukocyte count 3.82 × 109/L, lymphocytes 46.1 % and neutrophils 23.8 %.
By liver function tests, ALT 39.6 U/L and AST 53.2 U/L.
By routine blood tests on Nov. 6th, 2009, leukocyte count 6.57 × 109/L, lymphocytes 50.8 % and neutrophils 32.2 %.
By liver function tests, ALT 25.56 U/L and AST 30.2 U/L.
Diagnostic Imaging
On Nov. 1st, 2009 (Fig. 11.21): chest X-ray demonstrated flaky and flocculent shadows in both lungs, being more obvious in the right lower lung. Pulmonary markings deranged. Pulmonary hila unclear. The chest and neck have subcutaneous gas density shadows.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.21
Case 11.22
History of Present Illness. A 14-years-old boy, complained of fever and dry cough for 1 day, with runny nose of watery rhinorrhea.
Past History. None related to the present illness.
Contact History. He reported a history of contacts with Influenza A (H1N1) patients.
Signs. Pharyngeal congestion. The highest body temperature 39.2 °C.
Laboratory Tests
Throat swabs by CDC on Nov. 5th, 2009 found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
On Nov. 5th, 2009, blood sugar 8.73 mmol/L.
By routine blood tests on Nov. 5th, 2009, leukocyte count 4.95 × 109/L, lymphocytes and neutrophils normal.
Diagnostic Imaging. On Nov. 5th, 2009 (Fig. 11.22): chest X-ray demonstrated thickened pulmonary marking of both lungs, accompanying spotty blurry shadows, enlarged and thickened pulmonary hila.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.22
Case 11.23
History of Present Illness. A 12-years-old boy, complained of cough and expectoration for 2 weeks; aggravated conditions and fever for 3 days. He also had fatigue, poor appetite, runny nose and muscle soreness.
Past History. None related to the present illness.
Contact History. He reported a history of contact to Influenza A (H1N1) patients.
Signs. Body temperature 39.8 °C. Pharyngeal congestion. Tonsils not enlarged.
Laboratory Tests
Throat swabs by CDC on Oct. 27th, 2009 found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Oct. 30th, 2009, leukocyte count 3.8 × 109/L, lymphocytes 54.1 % and neutrophils 23.4 %.
By blood gas analysis on Nov. 1st, 2009, pH 7.513, PaCO2 34.9 mmHg, PaO2 77.9 mmHg.
By blood gas analysis on Nov. 3rd, 2009, pH 7.46, PaCO2 26 mmHg, PaO2 56.9 mmHg.
By blood gas analysis on Nov. 4th, 2009, pH 7.437, PaCO2 43.4 mmHg, PaO2 129.7 mmHg.
By blood gas analysis, pH 7.485, PaCO2 34.6 mmHg, PaO2 54.8 mmHg.
Diagnostic Imaging
On Oct. 30th, 2009 (Fig. 11.23a): chest X-ray demonstrated multiple flaky blurry shadows in the right lung, with enlarged and thickened hilum.
On Oct. 31st, 2009 (Fig. 11.23b): chest X-ray demonstrated progressed inflammation in the right lung, with enlarged inflammatory area.
On Nov. 2nd, 2009 (Fig. 11.23c): chest X-ray demonstrated enlarged inflammatory area.
On Nov. 4th, 2009 (Fig. 11.23d): chest X-ray demonstrated enlarged foci, diffusive cloud mist liked shadows with increased density of the left lung.
On Nov. 7th, 2009 (Fig. 11.23e): chest X-ray demonstrated patchy shadows in the right lung and the inflammation obviously absorbed.
Diagnosis . Pneumonia complicating Influenza A (H1N1).


Fig. 11.23
Case 11.24
Medical History. A 14-years-old boy, complained of fever and cough for 4 days.
On Nov. 6th, 2009, The patient fever without obvious causes, with a body temperature of 37.5 °C, which was irregular. He also had fatigue, paroxysmal cough occasionally with yellowish phlegm.
On Nov. 9th, 2009, The patient recurrent fever without obvious causes, with a body temperature of 39.0 °C. He also had chills, chest distress, dizziness, headache, general fatigue and muscle soreness. No runny nose and nasal obstruction. No chest pain, shortness of breath, palpitation, coughing up blood and dyspnea. He had a sore throat, foreign-body sensation during swallowing with accompanying nausea.
Past History. None related to the present illness.
Contact History. He reported a history of contacting with suspected patients with fever and a history of contacting with Influenza A (H1N1) patients. The school he was studying in was an epidemic area of Influenza A (H1N1).
Signs. Body temperature 37.3 °C, heart rate 108 beats/min. Breathing rate 22 times/min and blood pressure 102/63 mmHg. No lips cyanosis. Pharyngeal congestion. Follicles hyperplasia in the posterior wall of pharynx, no leukoplakia. Bilateral tonsils swollen to III degree. Respiratory sounds coarse in both lungs, with occasional fine dry and moist rales in both lungs.
Laboratory Tests
Throat swabs by CDC on Nov. 27th, 2009 found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 10th, 2009, Hb 140.9 g/L, leukocyte count 15.31 × 109/L, platelet counts 144.0 × 1012/L and neutrophils 82 %.
Diagnostic Imaging
On Nov. 10th, 2009 (Fig. 11.24a): chest X-ray demonstrated increased pulmonary markings, accompanying flaky blurry shadows.
On Nov. 10th, 2009 (Fig. 11.24b–g): chest CT scanning demonstrated scattered spotty and flaky foci with increased density and ground glass liked shadows with increased density, with unclearly defined boundaries.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.24
Case 11.25
History of Present Illness. A 6.5-years-old girl, complained of fever and cough for 6 days.
Past History. None related to the present illness.
Contact History. Self-reports of no history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39.7 °C, with pharyngeal congestion and tonsils swollen to II degree. Coarse respiration sounds of both lungs, with occasional coarse moist rales but none after cough.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Oct. 24th, 2009, leukocyte count 7.04 × 109/L, neutrophils 71.0 %, lymphocytes 22.3 %, erythrocyte count 4.03 × 1012/L, Hb 115 g/L and platelets count 193 × 109/L.
By routine blood tests on Oct. 28th, 2009, leukocyte count 3.16 × 109/L, neutrophils 72.81 %, lymphocytes 23.40 %, erythrocytes count 4.17 × 1012/L, Hb 108 g/L and platelets count 164 × 109/L.
By routine blood tests on Oct. 29th, 2009, leukocytes count 4.09 × 109/L, neutrophils 67.80 %, lymphocytes 22.50 %, erythrocytes count 4.04 × 1012/L, Hb 106 g/L and platelets count 166 × 109/L.
By routine blood tests on Nov. 11th, 2009, leukocytes count 4.86 × 109/L, neutrophils 60.74 %, lymphocytes 27.44 %, erythrocytes count 3.76 × 1012/L, Hb 99 g/L and platelets count 304 × 109/L.
By blood biochemistry on Oct. 28th, 2009, liver function normal; renal function tests results of BUN 4.1 mmol/L, Cr 59 μmol/L, uric acid 195 μmol/L, electrolytes normal, cholinesterase 5,624 U/L, CK 621 U/L and LDH 363 U/L.
By blood biochemistry on Nov. 1st, 2009, TP 61 g/L, A 28 g/L, ALT and AST normal, cholinesterase 4,284 U/L, CK 18 U/L and LDH 338 U/L.
By HBV-M, all indices negative; with HCVAb (−), HAVIgM (−), HIVAb (−), and syphilis (−).
By blood MycoDotTM, indices negative.
Erythrocyte sedimentation rate (ESR) 40 mm/h.
By sputum culture, pathogenic bacteria negative.
ECG. Sinus tachycardia and T-wave inversed.
Diagnostic Imaging
On Oct. 28th, 2009 (Fig. 11.25a): chest X-ray demonstrated flaky shadows of the right upper lung and increased pulmonary markings of both lungs.
On Oct. 30th, 2009 (Fig. 11.25b–f): chest CT scanning demonstrated large flaky parenchymal shadows with blurry boundaries in the right upper lung; visible bronchial congestion signs in the foci which were uneven in density. Lymph nodes enlargement visible before the trachea carina in the mediastinum; a little effusion in the right pleural cavity.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.25
Case 11.26
History of Present Illness. A 7-years-old boy, complained of fever and cough for 4 days. He coughed up a little whitish thick phlegm and occasional yellowish thick phlegm, with the fever and cough recurrent; increased and non-improved cough and expectoration.
Past History. None related to the present illness.
Contact History. Self reported a history of contacting closely with suspected fever patients.
Signs. Body temperature 38.2 °C, with the highest being 39.2 °C. Breathing rate 22 times/min; heart rate 105 beats/min; blood pressure 90/62 mmHg. Pharyngeal congestion, with bilateral tonsils swollen to II degree, but no suppuration. Respiratory sound coarse of both lungs.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 1st, 2009, leukocytes count 5.67 × 109/L, neutrophils 73.2 %, lymphocytes 22.3 %, erythrocytes count 4.17 × 1012/L, hemoglobin 124.7 g/L and platelets count 114 × 109/L.
Diagnostic Imaging
On Nov. 1st, 2009 (Fig. 11.26): chest X-ray demonstrated large flaky ground glass liked shadows of increased density in both lower lobe in lungs; enlarged and thickened pulmonary hila with the right hilum more obvious.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.26
Case 11.27
History of Present Illness. A 2-years-old boy, with chief complaints of fever and cough for 2 days, with accompanying runny nose. No chills and fatigue.
Past History. None related to the present illness.
Contact History. Self-reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39.6 °C, with pharyngeal congestion. Tonsils swollen to I degree.
Laboratory Tests
Throat swabs on Oct. 14th, 2009, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests, leukocytes count 5.9 × 109/L, lymphocytes 51.6 %, neutrophils 42.6 % and platelets count 190 × 109/L.
Diagnostic Imaging
On Oct. 14th, 2009 (Fig. 11.27): chest X-ray demonstrated diffusive patchy shadows of both lungs, with blurry pulmonary markings and the right lung more obvious.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.27
Case 11.28
History of Present Illness. A 12-years-old boy, complained of fever and cough for 5 days at clinic visit. He suffered from fever 5 days ago, with a body temperature of 39.7 °C and accompanying cough with whitish thick phlegm. No chills, convulsions, sore throat, nasal obstruction, runny nose, chest pain and diarrhea. In the local hospital, he received therapies of cefoperazone, Qingkailing, and Azithromycin for 4 days, with his body temperature still above 39 °C. At the day 5 of fever, he was found throat swabs positive and was then transferred to You’an Hospital in Beijing.
Past History. Self-report of myocarditis 8 years ago, cured. And self report a history of encephalitis 4 years ago.
Contact History. Self report with a history of contacting closely with Influenza A (H1N1) patients.
Signs. Pharyngeal congestion, with tonsils swollen to I degree. Respiration sounds coarse of both lungs, with no moist rales.
Laboratory Tests
By throat swabs, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 9th, 2009, leukocytes count 3.47 × 109/L, neutrophils 24.72 %, lymphocytes 63.41 %, erythrocytes count 4.81 × 1012/L, hemoglobin 139 g/L and platelets count 220 × 109/L.
By routine blood tests, on Nov. 14th, 2009, leukocytes count 6.55 × 109/L, neutrophils 37.10 %, lymphocytes 52.81 %, erythrocytes count 4.51 × 1012/L, hemoglobin 131 g/L, platelets count 286 × 109/L.
By blood biochemistry on Nov. 9th, 2009, liver function normal, kidney function normal, electrolytes normal, ALP 400 U/L, cholinesterase normal, and myocardial enzymes normal.
All HBV-M indices negative; HBsAb (+), HCVAb (−), HAVIgM (−), HIVAb (−) and syphilis (−).
By blood MycoDotTM, TB-check (−), TB-DOT weak positive and TB-Ab weak positive.
ESR 5 mm/h.
ECG. On Nov. 9th, 2009, sinus tachycardia and T-wave inversed.
Diagnostic Imaging
On Nov. 8th, 2009 (Fig. 11.28a): chest X-ray demonstrated increased density shadows of the left pulmonary hilum and slightly increased cardiac shadow.
On Nov. 9th, 2009 (Fig. 11.28b–f): chest CT scanning demonstrated patchy and cord liked shadows with increased density in the right upper lung and the left lung, with blurry boundaries but adhesion to pleura; no calcified foci.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.28
Case 11.29
History of Present Illness. A 5-years-old boy, complained of fever and cough for 5 days and hospitalized. He suffered from fever 5 days ago, with obvious paroxysmal cough. After therapies of Cefoperazone and Azithromycin, fever did not subside with a maintained body temperature of 36.6–39.5 °C. He also had nasal obstruction and runny nose. On the day of clinic visit, the throat swabs positive.
Past History. A reported past history of bronchial pneumonia 12 days ago.
Contact History. Not reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39.2 °C. Pharyngeal congestion, tonsils swollen to I degree. Respiration sounds of both lungs coarse, with occasional wheezing. Heart rate 128 beats/min.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 11th, 2009, leukocytes count 6.63 × 109/L, neutrophils 70.9 %, lymphocytes 20.8 %, erythrocytes count 3.7 × 1012/L, hemoglobin 116 g/L, platelets count 157 × 109/L and CRP 1.6 mg/L.
By routine blood tests on Nov. 15th, 2009, leukocytes count 5.83 × 109/L, neutrophils 19.62 %, lymphocytes 58.31 %, erythrocytes count 3.45 × 1012/L, hemoglobin 113 g/L and platelets count 132 × 109/L.
By blood biochemistry on Nov. 15th, 2009, TP 64 g/L, A 33 g/L, AST 46 U/L, ALT 56 U/L, renal functional BUN 1.6 mmol/L, uric acid 150 μmol/L, electrolytes normal, cholinesterase normal, CK 68/L, LDH 240 U/L, alkaline phosphatase 160 U/L and γ-GT16U/L.
By HBV-M, HBeAb (+), HCVAb (−), HAVIgM (−), HIVAb (−) and syphilis (−).
Diagnostic Imaging
On Nov. 11th, 2009 (Fig. 11.29a): chest X-ray demonstrated large flaky blurry shadows with increased density in the right lower lobe, enlarged and thickened pulmonary hilum.
On Nov. 16th, 2009 (Fig. 11.29b, c): chest CT scanning demonstrated cloud mist liked blurry shadows in both lower lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.29
Case 11.30
History of Present Illness. A 9-years-old boy, with chief complaints of fever, cough and expectoration for 3 days. He also suffered from chills, nasal obstruction, runny nose and slight cough with a little yellowish phlegm.
Past History. None related to the present illness.
Contact History. Self reported a history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 38.5 °C, with pharyngeal congestion and tonsils swollen to I degree. Respiration sound of both lungs clear.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 11th, 2009, leukocytes count 4.1 × 109/L, lymphocytes 49.7 % and neutrophils 38.3 %.
Diagnostic Imaging. On Sep. 30th, 2009 (Fig. 11.30): chest X-ray demonstrated increased pulmonary markings and small spotty and flaky blurry shadows of both lungs, increased and thickened pulmonary hila.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.30
Case 11.31
History of Present Illness. A 7-years-old boy, complained of fever and cough for 2 days, with accompanying chills, slight cough with no phlegm, no nasal obstruction and runny nose.
Contact History. Self report of coming from epidemic area.
Past History. None related to the present illness.
Signs. Body temperature 39.4 °C, with pharyngeal congestion and tonsils swollen to II degree.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on June 7th, 2009, leukocytes count 6.92 × 109/L, lymphocytes 15.7 % and neutrophils 65.4 %.
By routine blood tests on June 7th, 2009, leukocytes count 11.4 × 109/L, lymphocytes 22 % and neutrophils 58 %.
By routine blood tests on June 29th, 2009, leukocytes count 5.2 × 109/L, lymphocytes 23.1 % and neutrophils 57.2 %.
Diagnostic Imaging
On June 28th, 2009 (Fig. 11.31a): chest X-ray demonstrated large flaky blurry shadows of middle-lateral peripheries in the right lower lung; unclearly demonstrated right lateral diaphragmatic surface and costophrenic angle.
On July 2nd, 2009 (Fig. 11.31c–f): chest CT scanning demonstrated large flaky parenchymal shadows of the right lower lung, with an upper boundary at the right oblique fissure.
Figure 11.31g–i: Pulmonary parenchymal shadows in mediastinal window.
On July 5th, 2009 (Fig. 11.31b): chest X-ray demonstrated increased and blurry pulmonary markings of both lungs; flaky limited shadows with increased density in the right middle-lower lung.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.31
Case 11.32
History of Present Illness. A 18-years-old man, complained of fever, cough and expectoration for 4 days, with accompanying runny nose.
Past History. None related to the present illness.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 40.1 °C, with pharyngeal congestion but no tonsils not enlarged. Moist rales of both lungs.
Laboratory Tests
Throat swabs by CDC on Oct. 27th, 2009 found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Oct. 30th, 2009, leukocytes count 10.8 × 109/L, lymphocytes 81.0 % and neutrophils 9.8 %.
On Oct. 30th, 2009, throat swabs negative.
Diagnostic Imaging
On Oct. 30th, 2009 (Fig. 11.32): chest X-ray demonstrated flocculent patchy shadows in cardiophrenic angle of the right lower lung.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.32
Case 11.33
History of Present Illness. A 16-years-old boy, complained of fever for 4 days and the right chest pain for 3 days. He also suffered from chills, runny nose, cough with whitish phlegm. Three days before hospitalized he started feeling distending and persistent right chest pain, with bloody phlegm and shortness of breath.
Past History. None related to the present illness.
Contact History. Self reported history of contacting closely with Influenza A (H1N1) patients.
Signs. Body temperature 36.9 °C, heart rate 76 beats/min, breathing rate 20 times/min and blood pressure 115/65 mmHg.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus negative, the universal gene (NP gene) of H1N1 swine flu virus negative, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 21st, 2009, leukocytes count 24.4 × 109/L and neutrophils 90.7 %.
By blood biochemistry, K+ 4.3 mmol/L, Na+ 136.5 mmol/L, Cl− 96.1 mmol/L, pH 7.47, PaO2 35.5 mmHg, PaCO2 109.7 mmHg. HcT 62.1 %, \( {\text{HCO}}_{3}^{-}\)26.1 mmol/L and free Ca 1.15 mmol/L.
By blood biochemistry on Nov. 23rd, 2009, K+ 4.67 mmol/L, Na+ 139.2 mmol/L, \( {\text{HCO}}_{3}^{-}\)27.2 mmol/L, Cl− 103.5 mmol/L, AG 8.5 mmol/L. ALT 12.9 U/L and AST 21.5 U/L.
By routine blood tests on Nov. 25th, 2009, leukocytes count 7.9 × 109/L, neutrophils 82.7 % and lymphocytes 12.2 %.
By blood gas analysis, pH 7.408, PaCO2 34.6 mmHg, PaO2 86 mmHg, SaO2 97 % and \( {\text{HCO}}_{3}^{-}\)21.9 mmol/L.
By routine blood tests on Nov. 27th, 2009, leukocytes count 3.72 × 109/L, lymphocytes 30.6 % and neutrophils 58.30 %.
Diagnostic Imaging
On Nov. 25th, 2009 (Fig. 11.33a–d): plain CT scanning demonstrated flaky blurry shadows with increased density in the right middle lung, with blurry boundaries.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.33
Case 11.34
History of Present Illness. A 31-years-old woman, 4 days after her cesarean delivery, with chief complaints of high fever, spasmodic breathing, and progressive dyspnea for 2 days. She suffered from sudden high fever 2 days after delivery and cough 1 day ago, with pink foamy phlegm. She also had progressive dyspnea, with no improvement after therapies but rapid deterioration.
Past History. None related to the present illness.
Contact History. Self reported history of contacting closely with Influenza A (H1N1) patients.
Signs. The highest body temperature 40 °C, with lips cyanosis. Respiration sound of both lungs coarse, with diffusive dry and moist rales. Heart rate 136 beats/min, being regular. Abdomen bloating.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus negative, the universal gene (NP gene) of H1N1 swine flu virus negative, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 8th, 2009, leukocytes count 12.97 × 109/L, erythrocytes count 3.24 × 1012/L, hemoglobin 83 g/L, neutrophils 91.1 %, platelets count 295 × 109/L.
By routine blood tests on Nov. 19th, 2009, leukocytes count 17.31 × 109/L, hemoglobin 116 g/L, neutrophils 84.7 % and platelets count 257 × 109/L.
By blood gas analysis, albumin 31.20 g/L, creatinine 147.4 μmol/L and C-reactive protein 163 mg/L.
Diagnostic Imaging
On Nov. 6th, 2009 (Fig. 11.34a, b): chest X-ray demonstrated large flaky blurry shadows with increased density in both lungs.
On Nov. 6th, 2009 (Fig. 11.34c–s): chest CT scanning demonstrated large flaky blurry shadows with increased density in the posterior basal segments of both lower lungs; parenchymal changes of some pulmonary tissues; enlarged and thickened pulmonary hila.
Diagnosis. Pneumonia complicating Influenza A (H1N1).




Fig. 11.34
Case 11.35
History of Present Illness. A 27-years-old woman, complained of menopause for 37+5 weeks and fever for 7 days. She also complained of frequent fetal movements for 5 days, decreased fetal movements for 1 day and bloody show for 2 days. Symptoms also included fever 7 days ago, with throat upset, general soreness and the highest body temperature 39.5 °C. Six days ago she suffered from frequent cough, a sore throat, difficulty supine and body temperatures fluctuating between 38 and 39.5 °C.
She was admitted on Nov. 14th, 2009. Medical consultation made a decision of terminating pregnancy.
Diagnosis. Pregnancy for 37+5 weeks, Influenza A (H1N1), pneumonia, suspected respiratory failure, fatal distress and anemia.
Past History. None related to the present illness.
Contact History. Self reported history of contacting closely with Influenza A (H1N1) patients.
Signs. Body height 164 cm, weight 80 kg, uterus height 31 cm, abdominal girth 93 cm and estimated fetus weight 3,300 g. Position of fetal heart LOA, fatal heart rate regular about 146 beats/min. Presentation floating, no palpable uterine contraction. External pelvimeters IS 24 cm, IC 26 cm, EC 19 cm and TO 9 cm.
By obstetrical color ultrasonography on Nov. 14th, 2009, static fetal heartbeat.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus negative, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 14th, 2009, leukocytes count 5.25 × 109/L, hemoglobin 86 g/L, neutrophils 82.1 %, lymphocytes 16.4 %, platelets count 174 × 109/L, albumin 16 g/L and globulin 22.47 g/L.
By blood gas analysis on Nov. 14th, 2009, pH 7.42, PaCO2 19.13 mmHg, PaO2 63 mmHg and oxygen saturation 95 %.
By routine blood tests, leukocytes count 7.09 × 109/L, hemoglobin 105 g/L, neutrophils 73.3 %, lymphocytes 19.7 % and platelets count 418 × 109/L.
By blood biochemistry, albumin 32.88 g/L and creatinine 60.6 μmol/L.
Diagnostic Imaging
On Nov. 23rd, 2009 (Fig. 11.35a): chest X-ray demonstrated diffusive blurry shadows with increased density in the right lower lung; cloud mist liked shadows with increased density in the left lower lung; enlarged and thickened pulmonary hilum.
On Nov. 25th, 2009 (Fig. 11.35b): chest X-ray demonstrated diffusive cloudy shadows with increased density in the right lower lung; enlarged and thickened pulmonary hilum; no improvements compared to the previous imaging results.
On Nov. 25th, 2009 (Fig. 11.35c–p): CT scanning demonstrated large flaky dense shadows in the right lower lung.
Diagnosis. Pneumonia complicating Influenza A (H1N1).



Fig. 11.35
Case 11.36
History of Present Illness. A 24-years-old woman, complained of cough, expectoration and fever for 3 days, with the highest body temperature 39.8 °C, yellowish mucoid phlegm and spontaneous sweating.
Past History. None related to the present illness.
Contact History. Self reported history of contacting closely with Influenza A (H1N1) patients.
Signs. Respiration sounds of both lungs coarse, with moist rale in both lower lungs. Heart beats 108 beats/min.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus negative, the universal gene (NP gene) of H1N1 swine flu virus negative, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood Tests, leukocytes count 11.08 × 109/L, hemoglobin 77 g/L, neutrophils 91.9 %, C-reactive protein 45.5 mg/L, total protein 57.48 g/L and albumin 26.42 g/L.
By routine blood tests on Nov. 25th, 2009, leukocytes 12.99 × 109/L, erythrocytes count 3.85 × 1012/L, hemoglobin 100 g/L, neutrophils 88.3 %, platelets count 158 × 109/L and albumin 28.34 g/L.
Diagnostic Imaging
On Nov. 3rd, 2009 (Fig. 11.36a, b): chest X-ray demonstrated flaky cloudy shadow with increased density in both lower lungs; enlarged and thickened pulmonary hilum.
On Nov. 5th, 2009 (Fig. 11.36c): chest X-ray demonstrated diffusive flaky cloudy shadow with increased density in middle-lower lobes of both lungs, thickened hilum covered; obvious progression compared to previous chest X-ray.
On Nov. 6th, 2009 (Fig. 11.36d): chest X-ray demonstrated diffusive flaky cloudy shadow with increased density in middle-lower lobes of both lungs; thickened hilum covered; no obvious changes compared to the previous chest X-ray.
On Nov. 7th, 2009 (Fig. 11.36e): chest X-ray demonstrated diffusive flaky cloudy shadows with increased density in middle-lower lobes of both lungs; thickened hilum covered; no obvious changed compared to the previous chest X-ray.
On Nov. 7th, 2009 (Fig. 11.36f–l): chest CT scanning demonstrated diffusive patchy parenchymal shadows with increased density in both lungs, with air bronchogram.
On Nov. 23rd, 2009 (Fig. 11.36m): chest X-ray demonstrated diffusive flaky cloudy shadows with increased density in both lungs; thickened hilum covered; obvious progression compared to previous X-ray.
On Nov. 23rd, 2009 (Fig. 11.36n–x): chest CT scanning demonstrated diffusive parenchymal shadows with increased density and ground glass-like shadows in both lungs, with gas bronchogram which was more obvious in the posterior basal segments of both lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).





Fig. 11.36
Case 11.37
History of Present Illness. A 18-years-old woman, with chief complaints of fever and cough for 2 days, with dyspnea and vomiting for 1 day. Hospitalized.
Past History. None related to the present illness.
Contact History. Self reported history of contacting closely with Influenza A (H1N1) patients.
Signs. Pharyngeal congestion, with antiadoncus. Moist rales in both lungs and respiration sound coarse.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus negative, the universal gene (NP gene) of H1N1 swine flu virus negative, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests, leukocytes count 11.1 × 109/L and neutrophils 82 %.
By blood gas analysis, pH 7.43, PaCO2 35.2 mmHg, PaO2 66 mmHg, \( {\text{HCO}}_{3}^{-}\) 23.4 mmol/L and SaO2 93 %.
Diagnostic Imaging
On Nov. 11th, 2009 (Fig. 11.37a–d): plain CT scanning demonstrated multiple patchy cloudy shadows in middle lobes of both lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.37
Case 11.38
History of Present Illness. A 19-years-old woman, complained of fever, cough and a sore throat for 26 h.
Past History. None related to the present illness.
Contact History. Self reported history of contacting closely with Influenza A (H1N1) patients.
Signs. Body temperature 39.7 °C, with pharyngeal congestion.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus negative, the universal gene (NP gene) of H1N1 swine flu virus negative, specific gene (HA gene) of Influenza A (H1N1) virus positive.
On Nov. 23rd, 2009, By routine blood tests, leukocytes count 8.77 × 109/L, neutrophils 81.6 % and lymphocytes 9.6 %.
By blood gas analysis, ALT 13.5 U/L and AST 21.4 U/L.
By routine blood tests on Nov. 24th, 2009, leukocytes count 5.41 × 109/L, neutrophils 62.74 % and lymphocytes 27.50 %.
Diagnostic Imaging
On Nov. 25th, 2009 (Fig. 11.38a–d): chest plain CT scanning demonstrated large flaky shadows with increased density in the right middle lung.
Diagnosis. Pneumonia complicating Influenza A (H1N1). Acute facial features.

Fig. 11.38
Case 11.39
History of Present Illness. A 23-years-old man, complained of fever, cough and expectoration for a week, with a body temperature of 39 °C and no chills and chest distress.
Past History. None related to the present illness.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Pharyngeal congestion, with tonsils not enlarged.
Laboratory Tests
Throat swabs by CDC found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus negative, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests, leukocytes count 1.48 × 109/L, hemoglobin 130 g/L, platelets count 130 × 1012/L.
By routine blood tests on Nov. 14th, 2009, leukocytes count 2.39 × 109/L, lymphocytes 36.4 % and neutrophils 51.1 %.
By blood gas analysis, pH 7.462, PaCO2 40.1 mmHg and PaO2 79.2 mmHg.
Diagnostic Imaging
On Nov. 14th, 2009 (Fig. 11.39a): chest X-ray demonstrated patchy flocculent shadows in lower lobes of both lungs; enhanced Lung markings.
On Nov. 15th, 2009 (Fig. 11.39b): chest X-ray demonstrated flaky cloudy shadows with increased density in lower lobes of both lungs; thickened lung markings and enlarged left lung hilum; obvious improved conditions compared to previous chest X-ray.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.39
Case 11.40
History of Present Illness. A 25-years-old man, complained of fever, a sore throat and cough up phlegm for 2 days, with accompanying shortness of breath and muscle soreness.
Contact History. Unknown.
Signs. Body temperature 39 °C, with pharyngeal congestion and tonsils swollen to I degree.
Laboratory Tests
Throat swabs by CDC on Nov. 10th, 2009 found universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus negative, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By blood gas analysis on Nov. 12th, 2009, pH 7.342, PaCO2 45.7 mmHg and PaO2 89.7 mmHg.
By blood gas analysis on Nov. 14th, 2009, normal.
By routine blood tests on Nov. 13th, 2009, leukocytes count 4.96 × 109/L, lymphocytes 17.1 % and neutrophils 74 %.
By blood gas analysis, on Nov. 15th, 2009, pH 7.456, PaCO2 40.8 mmHg and PaO2 127.6 mmHg.
By routine blood tests leukocytes count 8.28 × 109/L, lymphocytes 10.1 % and neutrophils 78.5 %.
Diagnostic Imaging
On Nov. 11th, 2009 (Fig. 11.40a): chest X-ray demonstrated symmetrical thorax; rightward migration of the trachea; decreased transparency of both lungs fields; enhanced and blurry lung markings; multiple intrapulmonary patchy blurry shadows, and heart shadow enlarged.
On Nov. 13th, 2009 (Fig. 11.40b): chest X-ray demonstrated symmetrical thorax, rightward migration of the trachea, decreased transparency of both lungs, thickened lung markings, multiple intrapulmonary flocculent patchy shadows in both lungs.
On Nov. 15th, 2009 (Fig. 11.40c): chest X-ray demonstrated enhanced and blurry lung markings, multiple intrapulmonary patchy cloudy shadows, and cardiac shadow enlarged.
On Nov. 17th, 2009 (Fig. 11.40d): chest X-ray demonstrated enhanced and blurry lung markings, decreased transparency of both lungs, multiple intrapulmonary patchy cloudy shadows, and the cardiac shadow enlarged.
On Nov. 20th, 2009 (Fig. 11.40e): chest X-ray demonstrated blurry lung markings, multiple intrapulmonary patchy blurry shadows; decreased shadows in the right lung compared to the previous X-ray.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.40
Case 11.41
History of Present Illness. A 21-years-old man, complained of fever for 5 days and cough for 1 day. He also suffered from headache, throat itch, nasal obstruction and runny nose.
Past History. None related to the present illness.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 37.8 °C, with pharyngeal congestion and tonsils swollen to I degree.
Laboratory Tests
By throat swabs, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 10th, 2009, leukocytes count 4.71 × 109/L, neutrophils 77.51 % and lymphocytes 13.82 %.
By blood biochemistry on Nov. 11th, 2009, liver function normal, renal function normal, electrolytes normal, myocardial enzymes normal, blood sugar level normal and LDH normal.
By HBV-M on Nov. 10th, 2009, HBsAb (+), HCVAb (−), HAVIgM (−), HIVAb (−) and syphilis (−).
On Nov. 12th, 2009, ECG normal.
On Nov. 13th, 2009, sputum culture negative.
By routine blood tests on Nov. 17th, 2009, leukocytes count 11.31 × 109/L, neutrophils 68.3 %, lymphocytes 21.6 % and erythrocytes count 4.72 × 1012/L.
On Nov. 18th, 2009, the patients was cured to be discharged.
Diagnostic Imaging
On Nov. 10th, 2009 (Fig. 11.41a): chest X-ray demonstrated flaky blurry shadows of the right middle-upper lung, enlarged and thickened pulmonary hilum, increased and thickened lung markings.
On Nov. 10th, 2009 (Fig. 11.41b–i): chest CT scanning demonstrated patchy light blurry shadows and ground glass liked shadows in bilateral lower lungs and the right middle lung, with uneven densities; no other abnormalities.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.41
Case 11.42
History of Present Illness. A 42-years-old man, with chief complaints of fever and cough for 5 days.
Past History. Self reported history of Hepatitis B for 10 years with regular liver function examination every half a year. None recent abnormalities.
Contact History. He denied recent contacts with Influenza A (H1N1) patients.
Signs. Body temperature 39.5 °C, with pharyngeal congestion and tonsils swollen to I degree. Coarse respiration sounds of bilateral lungs.
Laboratory Tests
By throat swabs, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 5th, 2009, leukocytes count 3.24 × 109/L, neutrophils 57.74 % and lymphocytes 32.74 %.
By blood biochemistry on Nov. 15th, 2009, TP 55 g/L, A 27 g/L, AST 100 U/L, ALT 69 U/L, BUN 2.8 mmol/L, uric acid 187 μmol/L, electrolyte Na+ 132 mmol/L, Cl− 94 mmol/L, Ca2+ 2.16 mmol/L, cholinesterase 3,588 U/L, CK 621 U/L and LDH 511 U/L.
By routine urine tests, URO (+).
By HBV-M, HBeAg (+), HBcAB (+), HCVAb (−), HAVIgM (−), HIVAb (−) and syphilis (−).
By HBV-DNA, 2.54 × 103.
By physical examinations on Nov. 8th, 2009, persistent fever during hospitalization, with body temperatures between 37.4 and 39.2 °C. The patient also had cough, expectoration and chest distress. Moist rales in both lungs and the right lung extensive moist rales.
By routine blood tests on Nov. 9th, 2009, leukocytes count 11.47 × 109/L, neutrophils 81.03 % and lymphocytes 8.82 %.
By blood biochemistry on Nov. 9th, 2009, TP 55 g/L, A 24 g/L, AST 64 U/L, ALT 54 U/L and BUN 3.4 mmol/L.
By blood gas analysis on Nov. 10th, 2009, pH 7.517, PaCO2 33.3 mmHg, PaO2 49 mmHg and SaPaO2 91 %. The patient had progressive conditions, with palpitation, more serious chest distress, cough and obvious expectoration. His family members requested transferring into another hospital due to his deteriorating conditions.
By sputum culture on Nov. 13th, 2009, Candida albicans positive.
On Nov. 4th, 2009, ECG normal.
Diagnostic Imaging
By B-mode ultrasonography on Nov. 7th, 2009, diffusive echo of liver parenchymal changes; multiple intrahepatic cysts in liver; hemangioma in right lobe of liver; spleen thickness 45 mm.
By chest CT scanning on Nov. 5th, 2009 (Fig. 11.42a–g), decreased transparency of the right lung with large flaky shadows; small flaky shadows in the left lower lung next to the heart margin with air bronchogram.
By chest X-ray on Nov. 5th, 2009 (Fig. 11.42h), large flaky cloud mist liked blurry shadows of both lungs; parenchymal changes shadows of the right upper lung.
By chest CT scanning on Nov. 9th, 2009 (Fig. 11.42i–q), scattered flocculent light blurry shadows and ground glass liked shadows in both lungs; parenchymal changes of partial lung tissues; gas bronchogram and quite good transparency of the left lung.
Diagnosis. Pneumonia complicating Influenza A (H1N1).



Fig. 11.42
Case 11.43
History of Present Illness. A 41-years-old woman, complained of fever and cough for 6 days, with accompanying headache, runny nose, no phlegm, no chills and no fatigue.
Past History. None related to the present illness.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39.3 °C, with pharyngeal congestion and tonsils swollen to II degree.
Laboratory Tests
By throat swabs, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests, leukocytes count 2.5 × 109/L, lymphocytes 26.8 % and neutrophils 65.6 %.
Diagnostic Imaging
By chest X-ray on Nov. 17th, 2009 (Fig. 11.43a): thickened lung markings of both lower lungs, with spotty blurry shadows.
By chest CT scanning on Nov. 18th, 2009 (Fig. 11.43b–p): multiple patchy shadows in dorsal segment of the left lower lung and posterior basal segment of the right lower lung, with blurry boundaries.
Diagnosis. Pneumonia complicating Influenza A (H1N1).




Fig. 11.43
Case 11.44
History of Present Illness. A 22-years-old woman, complained of fever for 1 week, cough and expectoration for 3 days, with the highest body temperature 40 °C.
Past History. None related to the present illness.
Contact History. Self reported of no recent contacts with Influenza A (H1N1) patients.
Signs
On Nov. 19th, 2009, heartbeat rate 180–190 beats/min and arterial oxygen saturation 65–77 %.
On Nov. 21st, 2009, suddenly slowed heart rate, decreased blood pressure and reduced arterial oxygen saturation to 35 %. Death occurred during emergency rescuing.
Laboratory Tests
By throat swabs, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By blood gas analysis on Nov. 19th, 2009, pH 7.45, PaCO2 39 mmHg, PaO2 478 mmHg, arterial oxygen saturation 69 %. Tracheal intubation at 4 p.m., with pH 7.36–7.26, PaCO2 41–56 mmHg and PaO2 37–59 mmHg.
By routine blood tests on Nov. 21st, 2009, leukocytes count 3.5 × 109/L, neutrophils 83.6 %, band neutrophils 8–14 %, with visible toxic granules.
By liver functions test, ALT 33.9 U/L with the highest of 109 U/L, AST 85.8 U/L with the highest of 507 U/L.
By renal functions test, BUN and Cr normal.
Diagnostic Imaging
By chest X-ray on Nov. 20th, 2009 (Fig. 11.44): large blurry shadows with increased density in middle and lower lobes of both lungs, more obvious in the both lower lungs; unclearly defined costophrenic angle at the uppermost of diaphragm.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.44
Case 11.45
History of Present Illness. A 37-years-old man, with chief complaints of fever and cough for 1 week, with expectoration of a little whitish phlegm, chest distress and progressively deteriorated conditions. By blood gas analysis, type I respiratory failure. After hospitalized, he was masked for inhalation of oxygen.
Past History. None related to the present illness.
Contact History. Self reported recent contacts with Influenza A (H1N1) patients.
Signs. Body temperature 39 °C, with pharyngeal congestion and tonsils not enlarged. Moist rales of both lungs.
Laboratory Tests
By throat swabs, CDC on Nov 15th, 2009 universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus negative, specific gene (HA gene) of Influenza A (H1N1) virus negative.
Diagnostic Imaging
By chest X-ray on Nov. 14th, 2009 (Fig. 11.45): flocculent patchy cloudy shadows with high density in both lungs, more obvious in the lower lobes; blurry lung markings; enlarged and blurry hila.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.45
Case 11.46
History of Present Illness. A 19-years-old man, complained of fever, headache and cough for 1 day, with irregular fever, headache, dizziness, cough and fatigue. He also suffered from a sore throat and a foreign-body sensation when swallowing. The next day, his body temperature reached 38.5 °C, with cough of a little yellowish and whitish phlegm. By physical examinations, hemogram increased, high body temperature of 42 °C, with nausea, vomiting, chest distress and shortness of breath.
Past History. None related to the present illness.
Contact History. Self reported contacts with suspected fever patients. The school he was studying in had many students suffering from fever and four were definitively diagnosed as Influenza A (H1N1) patients.
Signs. Body temperature 39.8 °C. Heart rate 102 beats/min, breathing rate 28 times/min and blood pressure 107/52 mmHg, with no lips cyanosis. Pharyngeal slight congestion. Follicles hyperplasia on the posterior wall of pharynx.
Laboratory Tests
By throat swabs, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 8th, 2009, hemoglobin 135 g/L, WBC 5.50 × 109/L, platelets count 175 × 109/L and neutrophils 70.7 %.
Diagnostic Imaging
By chest X-ray on Nov. 8th, 2009 (Fig. 11.46a): coarse lung markings of both lower lungs, enlarged pulmonary hila.
By chest CT scanning on Nov. 8th, 2009 (Fig. 11.46b–e) cloud mist liked blurry shadows of both lower lungs, decreased transparency of both lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.46
Case 11.47
History of Present Illness. A 44-years-old man, was hospitalized due to cough and expectoration for 6 days and fever for 4 days. One week prior to hospitalization, he accompanied a guest to the airport and no other reported contact histories.
Past History. Self reported history of diabetes for 2 years.
Contact History. Denied.
Signs. Body temperature 36 °C. Coarse respiration sound of bilateral lungs.
Laboratory Tests
By throat swabs, PT-PCR test positive for the nucleic acid of Influenza A (H1N1) virus.
By routine blood Tests, hemoglobin 135 g/L, leukocytes count 5.1 × 109/L, neutrophils 52.1 % and lymphocytes 32.3 %.
Diagnostic Imaging
By chest X-ray on Nov. 14th, 2009 (Fig. 11.47a): enhanced lung markings of both lungs; small flaky shadows with increased density in the middle band of the right upper lung, with a cord liked shadow connecting to the pulmonary hilum; irregular grid liked and spotty flaky shadows with densed density in the middle and lower right lung, unclear boundaries.
By X-ray on Nov. 16th, 2009 (Fig. 11.47b): enhanced lung markings of both lungs; scattered spotty and flaky shadows with densed density and irregular grid liked shadows in the both middle and lower lungs, boundaries unclear. Basically absorbed foci in the right upper lung, smaller focal areas in both middle and lower lungs, and less densed shadows, comparing to the previous X-ray findings.
By X-ray on Nov. 18th, 2009 (Fig. 11.47c): enhanced and blurry lung markings; intrapulmonary foci absorbed comparing to the previous X-ray findings.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.47
Case 11.48
History of Present Illness. A 23-years-old man, complained of fever and cough for 2 days, with a body temperature of 37.7 °C, slight cough, no phlegm and fatigue.
Past History. None related to the present illness.
Contact History. Self reported his coming from the epidemic area, from the US to Beijing by airplane on June 24th, 2009.
Signs. Pharyngeal congestion and tonsils not enlarged.
Laboratory Tests
By throat swabs (CDC), universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests on June 28th, 2009, leukocytes count 5.9 × 109/L, lymphocytes 16.7 % and neutrophils 70.4 %.
By routine blood tests on June 30th, 2009, leukocytes count 4.1 × 109/L, lymphocytes 42.7 % and neutrophils 44.9 %.
Diagnostic Imaging
By chest X-ray on June 28th, 2009 (Fig. 11.48): blurry lung markings, with accompanying patchy shadows.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.48
Case 11.49
History of Present Illness. A 27-years-old man, complained of fever and cough for a week. His body temperature 42 °C, with chills, watery rhinorrhea, nasal obstruction and a sore throat.
Past History. Not reported.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Pharyngeal congestion and tonsils swollen to I degree.
Laboratory Tests
By throat swabs, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By routine blood tests, leukocytes count 5.12 × 109/L, lymphocytes 21.7 % and neutrophils 60 %.
By liver functions test, ALT 138.5 U/L and AST 53.4 U/L.
By routine blood tests on Nov. 12th, 2009, leukocytes count 10.7 × 109/L, lymphocytes 6.8 % and neutrophils 87.3 %.
Diagnostic Imaging
By chest X-ray on Nov. 6th, 2009 (Fig. 11.49a, b): enhanced lung markings; flaky cloudy shadows in the left lower lung; decreased transparency of the left lung.
Diagnosis . Pneumonia complicating Influenza A (H1N1).

Fig. 11.49
Case 11.50
History of Present Illness. A 46-years-old man, complained of fever and cough for a week. His body temperatures were interictal, with the highest body temperature of 40.33 °C. He also suffered from chills, a sore throat, cough up a little whitish phlegm and headache.
Past History. Not reported.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Pharyngeal congestion, with tonsils not swollen. Moist rales of both lungs.
Laboratory Tests
By throat swabs on Nov. 5th, 2009, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
ECG. On Nov. 6th, 2009, sinus bradycardia.
Diagnostic Imaging
By chest X-ray on Nov. 6th, 2009 (Fig. 11.50a): increased lung markings of both lungs; multiple flaky blurry shadows in the right lung; blurry lung markings of the left lower lung.
By chest X-ray on Nov. 8th, 2009 (Fig. 11.50b): increased lung markings of both lungs; multiple flaky blurry shadows in the right lung; blurry lung markings of the left lower lung; no obvious changes compared to the previous X-ray findings.
By chest X-ray on Nov. 11th, 2009 (Fig. 11.50c): increased lung markings of both lungs; multiple flaky blurry shadows of the right lung; improved conditions compared to the previous X-ray findings.
By chest X-ray on Nov. 14th, 2009 (Fig. 11.50d): increased lung markings of both lungs, with spotty shadows; improved conditions compared to the previous X-ray findings.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.50
Case 11.51
History of Present Illness. A 15-years-old girl, with chief complaints of recurrent fever and cough for 1 week.
On Oct. 31st, 2009, she began to have fever with no obvious known causes, body temperature 38.6 °C. Her fever was irregular, with paroxysmal cough and a little whitish phlegm. She also suffered from dizziness, fatigue, rhinorrhea, nasal obstruction, a sore throat and a foreign-body sensation when swallowing. She took medicine for the cold such as Radix Isatidis, but the condition not improved. On the second day after medication, she still had dizziness and fever, with self reported body temperature of 39.2 °C. The symptoms also included chills, nausea, vomiting of saliva and deteriorated cough with a little yellowish phlegm.
Past History. Not reported.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 38.5 °C, heart rate 115 beats/min, breathing rate 22 times/min, and blood pressure 122/65 mmHg. Pharyngeal congestion slight, no retropharyngeal folliculosis. Respiration sound coarse in both lungs, with occasional moist rales in the left lower lung. The right lung no abnormal findings.
Laboratory Tests
By throat swabs, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
Routine blood tests on Nov. 6th, 2009, hemoglobin 120 g/L, leukocytes count 6.18 × 109/L, platelets count 119 × 109/L and neutrophils 63.6 %.
By blood gas analysis on Nov. 6th, 2009, pH 7.327, PaO2 76 mmHg, PaCO2 38.6 mmHg and oxygen content 137 mL/L.
By blood biochemistry on Nov. 6th, 2009, AST 38 U/L, CK 130 U/L, CK-MB 7.5 U/L, LDH 270 U/L and HBD 198 U/L.
Diagnostic Imaging
By chest X-ray on Nov. 6th, 2009 (Fig. 11.51a): cloud mist liked blurry shadows in the left lower lung.
By chest X-ray on Nov. 7th, 2009 (Fig. 11.51b): cloud mist liked blurry shadows in the left lower lung; increased pulmonary hilum; no obvious changes compared to the previous X-ray findings.
By chest X-ray on Nov. 8th, 2009 (Fig. 11.51c): cloud mist liked blurry shadows in the left lower lung; increased pulmonary hilum; no obvious changes compared to the previous X-ray findings.
By chest CT scanning on Nov. 8th, 2009 (Fig. 11.51d–f): irregular flaky shadows with increased density in basilar segment of the left lower lung, in a size of 5 cm × 7 cm and no space occupying effect.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.51
Case 11.52
History of Present Illness. A 18-years-old man, complained of fever for 3 days and cough for 2 days. His highest body temperature 38.5 °C, with accompanying headache, muscle soreness, slight cough and expectoration of a little yellowish thick phlegm.
Past History. Not reported.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Pharyngeal congestion, tonsils not swollen. Moist rales in both lungs.
Laboratory Tests
By throat swabs, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
Diagnostic Imaging
By chest X-ray on Nov. 2nd, 2009 (Fig. 11.52): flaky and flocculent shadows in cardiophrenic angle of the left lower lung; pulmonary markings of the rest lung areas increased.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.52
Case 11.53
History of Present Illness. A 51-years-old woman, complained of fever and cough for 3 days and chest distress for 1 day. Her highest body temperature 39.7 °C, with accompanying chills, runny nose, shortness of breath and expectoration of a little odorless whitish phlegm occasionally with blood in it.
Past History. Not reported.
Contact History. The patients had a foreign nationality, with a self reported history of contacting with fever patients.
Signs. Pharyngeal congestion and tonsils swollen to I degree. Moist rale in both lungs.
Laboratory Tests
By throat swabs (CDC), universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By blood gas analysis, pH 7.4, PaCO2 39 mmHg and PaO2 42.2 mmHg.
By routine blood tests, leukocytes count 6.0 × 109/L and neutrophils 64 %.
By blood gas analysis on Nov. 23rd, 2009, pH 7.43, PaCO2 41 mmHg and PaO2 65 mmHg.
By routine blood tests, leukocytes count 3.83 × 109/L and neutrophils 64 %.
By liver functions test, ALT 28.9 U/L and AST 66.7 U/L.
By blood gas analysis on Nov. 24th, 2009, pH 7.4, PaCO2 40 mmHg and PaO2 75 mmHg.
By routine blood tests, leukocytes count 9.86 × 109/L and neutrophils 72.8 %.
By liver functions test, ALT 33 U/L and AST 52 U/L.
Diagnostic Imaging
By chest X-ray on Nov. 22nd, 2009 (Fig. 11.53a): increased lung markings of both lungs; patchy shadows with high density in the right lung and the left middle and lower lung, with boundaries unclear; pulmonary hila of both lungs unclear; two costophrenic angles blur.
By chest X-ray on Nov. 24th, 2009 (Fig. 11.53b): multiple patchy shadows in both lower lungs; progressive conditions compared to the previous chest X-ray findings.
By chest X-ray on Nov. 26th, 2009 (Fig. 11.53c): diffusive shadows with increased density in both lungs; decreased transparency of both lungs; progressive conditions compared to the previous chest X-ray findings.
By chest X-ray on Nov. 28th, 2009 (Fig. 11.53d): scattered patchy cloudy shadows with increased density in both lungs; enlarged and thickened pulmonary hilum; blunt right costophrenic angle; improved conditions compared to the previous chest X-ray findings.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.53
Case 11.54
History of Present Illness. A 15-years-old boy, complained of fever and cough for 3 days. His temperatures were irregular, the highest 39.7 °C, with accompanying paroxysmal coughs, a little whitish phlegm, a sore throat and a foreign-body sensation when swallowing.
Past History. Self reported frequent occurrence of the cold since childhood and persistent chronic cough and expectoration, which had been diagnosed as bronchiectasis in another hospital (no more details).
Contact History. Recent occurrence of fever in several classmates, who received no tests for Influenza A (H1N1). Self reported history of closely contacting with the classmates who had fever.
Signs. Body temperature 39.5 °C, heart rate 110 beats/min, breathing rate 22 times/min and blood pressure 110/60 mmHg. Pharyngeal congestion with tonsils swollen to II degree. Vocal fremitus in both lungs weakened and respiration sound of both lungs coarse, with scattered middle and fine moist rales in both middle-lower lungs. Apical impulse at the midclavicular line 0.5 cm inner to the fifth rib. Puffing murmurs of 3/6 grades during systoles in apical area.
Laboratory Tests
Throat swabs by CDC on Nov. 8th, 2009, nucleic acid of Influenza A (H1N1) virus positive.
By routine blood tests, leukocytes count 6.5 × 109/L, neutrophils 80.4 %, erythrocytes count 5.86 × 1012/L, hemoglobin 119.4 g/L, platelets count 160 × 109/L. Myocardial enzyme spectrum of CK 247 U/L, CK-MB 11.7 U/L, LDH normal, troponin I normal and aspartic acid aminotransferase normal.
By routine blood tests on Nov. 9th, 2009, leukocytes count 3.15 × 109/L, neutrophils 49.6 %, erythrocytes count 6.49 × 1012/L, hemoglobin 125.5 g/L and platelets count 217 × 109/L. Myocardial enzyme spectrum of CK 231 U/L, CK-MB 12.16 U/L, LDH normal, troponin I normal and aspartic acid aminotransferase normal.
By blood gas analysis, pH 7.452, PaCO2 27.4 mmHg, PaO2 75.9 mmHg, AB 18.7 mmHg and BE 5.30 mmol/L.
By electrocardiography, sinus rhythm and sinus arrhythmia.
By routine blood tests on Nov. 13th, 2009, leukocytes count 4.41 × 109/L and neutrophils 40.70 %.
Throat swabs by CDC on Nov. 17th, 2009, nucleic acid of Influenza A (H1N1) virus negative; the patient cured.
Diagnostic Imaging
By chest X-ray on Nov. 8th, 2009 (Fig. 11.54a), lung markings increased and rough; scattered flaky shadows with blurry boundaries and increased density in both lower lungs; thickened and enlarged hilar shadow in the right lung; decreased transparency of both lungs.
By chest CT scanning on Nov. 8th, 2009 (Fig. 11.54b–f), patchy lesion with high density in the left lower lung, with unclear boundaries; increased and deranged lung markings.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.54
Case 11.55
History of Present Illness. A 34-years-old man, complained of high fever for 7 days, with the highest body temperature of 39.4 °C. He also had dizziness, muscle soreness and fatigue. No headache. No sore or dry throat. No nasal obstruction and rhinorrhea. The next day, he had a slight cough, no expectoration, slight chest distress.
Past History. Not reported.
Contact History. Self reported history of contacting with fever patients.
Signs. Body temperature 38.4 °C, heart rate 72 beats/min, breathing rate 40 times/min and blood pressure 118/76 mmHg. SaO2 60 %. No lips cyanosis. Respiration sounds coarse in both lungs, with bronchial respiration sound in both upper lungs and fine bubbling sound in both lower lungs.
Laboratory Tests
By throat swabs (CDC), universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
Diagnostic Imaging
By chest X-ray on Nov. 15th, 2009 (Fig. 11.55a), cloud mist liked blurry shadows with increased density in both lungs; parenchymal changes of partial pulmonary tissues; enlarged and thickened pulmonary hila.
By chest CT scanning on Nov. 15th, 2009 (Fig. 11.55b–f), large flaky dense blurry shadows with increased density in both lungs; parenchymal changes of partial pulmonary tissues; enlarged and thickened pulmonary hila.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.55
Case 11.56
History of Present Illness. A 35-years-old man, complained of fever and cough for 2 days, with a body temperature of 39.3 °C. He also had chills, a sore throat, dry cough and headache.
Past History. Not reported.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Pharyngeal congestion, with tonsils not swollen. Moist rales of both lungs.
Laboratory Tests
By throat swabs on Nov. 8th, 2009, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By blood gas analysis on Nov. 14th, 2009, pH 7.463, PaCO2 34.6 mmHg and PaO2 73.8 mmHg.
By blood gas analysis on Nov. 15th, 2009, pH 7.513, PaCO2 29.1 mmHg, PaO2 101.2 mmHg.
By routine blood tests, leukocytes count 3.76 × 109/L, lymphocytes 20.7 % and neutrophils 77.4 %.
Diagnostic Imaging
By chest X-ray on Nov. 7th, 2009 (Fig. 11.56a), thickened and deranged pulmonary markings of both lungs; multiple flaky shadows in both lungs, with blurry boundaries; enlarged and blurry hilar shadows of both lungs.
By chest X-ray on Nov. 10th, 2009 (Fig. 11.56b), multiple flaky shadows of both lungs; progressive conditions of enlarged focal area compared to the previous X-ray findings on Nov. 7th, 2009.
By chest X-ray on Nov. 11th, 2009 (Fig. 11.56c), multiple flaky shadows in both lungs; improved conditions of decreased focal area compared to previous chest X-ray findings on Nov. 10th, 2009.
By chest X-ray on Nov. 13th, 2009 (Fig. 11.56d), no obvious changes compared to previous chest X-ray findings on Nov. 10th, 2009.
By chest X-ray on Nov. 15th, 2009 (Fig. 11.56e), improved conditions compared to the chest X-ray on Nov. 13th, 2009.
By chest X-ray on Nov. 16th, 2009 (Fig. 11.56f), no obvious changes compared to chest film on Nov. 15th, 2009.
By chest X-ray on Nov. 18th, 2009 (Fig. 11.56g), inflammation of both lungs; no obvious changes compared to chest X-ray findings on Nov. 16th, 2009.
By chest X-ray on Nov. 20th, 2009 (Fig. 11.55h), improved conditions compared to chest X-ray findings on Nov. 18th, 2009.
By chest CT scanning on Nov. 20th, 2009 (Fig. 11.56i–n), intrapulmonary patchy flocculent shadows in both lungs, with increased density and limited foci; improved transparency of the left lower lung.
Diagnosis. Pneumonia complicating Influenza A (H1N1).



Fig. 11.56
Case 11.57
History of Present Illness. A 20-years-old man, complained of fever and cough for 3 days. No chills, but a sore throat, slight cough with a little yellowish thick phlegm and headache.
Past History. Not reported.
Contact History. None related to the present illness.
Signs. Body temperature 39.34 °C, with pharyngeal congestion and tonsils not swollen. Moist rales in the right lower lung.
Laboratory Tests
By throat swabs, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By blood gas analysis, pH 7.437, PaCO2 33.4 mmHg and PaO2 81.4 mmHg.
By routine blood tests, leukocytes count 3.3 × 109/L, lymphocytes 4.8 % and neutrophils 90.6 %.
Diagnostic Imaging
By chest X-ray on Nov. 18th, 2009 (Fig. 11.57a), thick and deranged lung markings of both lungs; scattered patchy blurry shadows.
By chest X-ray on Nov. 20th, 2009 (Fig. 11.57b), patchy cloudy shadows of both lungs; improved conditions compared to chest X-ray findings on Nov. 18th, 2009.
By chest X-ray on Nov. 30th, 2009 (Fig. 11.57c), patchy cloudy shadows in both lungs; improved conditions compared to chest X-ray findings on Nov. 20th, 2009.
By chest CT scanning on Nov. 18th, 2009 (Fig. 11.57d–y), multiple patchy shadows in both lungs, especially in basal segments; boundaries unclear; air bronchogram.
Diagnosis. Pneumonia complicating Influenza A (H1N1).






Fig. 11.57
Case 11.58
History of Present Illness. A 59-years-old man complained of continuous choking for 3 days and fever for 2 days, with the highest body temperature of 39.3 °C. He also had chills, headache, muscle soreness, rhinorrhea, cough, expectoration (with a little yellowish thick phlegm) and fatigue.
Past History. Not reported.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Past History. Self reported history of hypertension and chronic bronchitis.
Signs. Pharyngeal congestion, without antiadoncus.
Laboratory Tests
By throat swabs on Nov. 19th, 2009, universal gene (M gene) of influenza A virus positive, the universal gene (NP gene) of H1N1 swine flu virus positive, specific gene (HA gene) of Influenza A (H1N1) virus positive.
By blood gas analysis, pH 7.397, PaCO2 23.7 mmHg, PaO2 107 mmHg and SaO2 297.7 %.
By routine blood tests, leukocytes count 11.2 × 109/L and neutrophils 96.3 %.
Diagnostic Imaging
By chest X-ray on Nov. 19th, 2009 (Fig. 11.58), flocculent flaky shadows in middle and lower lobes of both lungs, thickened lung markings.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.58
Case 11.59
History of Present Illness. A 27-years-old man complained of fever, cough and expectoration for a week, with accompanying chills, shivers, rhinorrhea and nasal obstruction.
Past History. None.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39.5 °C; Pharyngeal congestion and no antiadoncus; moist rales of both lungs.
Laboratory Tests
Throat swabs by CDC on Nov. 20th, 2009 found universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) negative.
By liver function tests on Nov. 20th, 2009, ALT 24 U/L and AST 72.8 U/L.
By blood gas analysis on Nov. 22nd, 2009, pH 7.62, PaCO2 18 mmHg and PaO2 186 mmHg.
By routine blood tests, leukocytes count 1.93 × 109/L, lymphocytes 33.7 % and neutrophils 96.3 %.
By liver function tests, ALT 25.7 U/L and AST 84.1 U/L.
By liver function tests on Nov. 24th, 2009, ALT 22 U/L and AST 50 U/L.
By routine blood tests, leukocytes count 1.93 × 109/L, neutrophils 44.4 % and lymphocytes 43.3 %.
Diagnostic Imaging
By chest X-ray on Nov. 20th, 2009 (Fig. 11.59a), increased lung markings accompanied with patchy flocculent cloudy shadows in both lower lungs; enlarged and thickened pulmonary hilum.
By chest X-ray on Nov. 22nd, 2009 (Fig. 11.59b), thickened lung markings of both lungs; multiple patchy flocculent shadows in both lungs, with blurry boundaries; hilum structure unclear; the right costophrenic angle blunt; progressive conditions compared to chest X-ray findings on Nov. 20th, 2009.
By chest X-ray on Nov. 24th, 2009 (Fig. 11.59c), increased lung markings of both lungs; spotty patchy cloudy shadows in both lungs; obviously improved conditions compared to chest X-ray findings on Nov. 22nd, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.59
Case 11.60
History of Present Illness. A 25-years-old man, complained of cough for 7 days and fever for 6 days. He had no chills, but a sore throat, shortness of breath and headache, followed by spasmodic breathing, with pink foam-like phlegm.
Past History. None.
Contact History. Denied a history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 40 °C, with pharyngeal congestion and tonsils swollen. Moist rales in both lungs.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
By liver function tests on Nov. 19th, 2009, ALT 81.3 U/L and AST 166.6 U/L.
By routine blood tests, leukocytes count 2.54 × 109/L, lymphocytes 15.4 %, and neutrophils 75.1 %.
By liver function tests on Nov. 23rd, 2009, ALT 63.1 U/L, AST 55.1 U/L, Cr 137.5 μmol/L and UREA 9.67 mmol/L.
By liver function tests on Nov. 24th, 2009, ALT 40 U/L, AST 32 U/L, Cr 115.9 μmol/L and UREA 16.73 mmol/L.
By blood gas analysis, pH 7.33, PaCO2 54 mmHg and PaO2 85 mmHg.
By routine blood tests, leukocytes count 17.89 × 109/L, lymphocytes 5.5 % and neutrophils 90.7 %.
By routine blood tests on Nov. 30th, 2009, leukocytes count 7.8 × 109/L, neutrophils 88.4 % and lymphocytes 8.2 %.
By blood gas analysis, pH 7.512, PaO2 48.8 mmHg and PaCO2 32.16 mmHg.
By liver function tests, ALT 166.8 U/L and AST 270.5 U/L.
Diagnostic Imaging
By chest X-ray on Nov. 19th, 2009(Fig. 11.60a), multiple flaky cloudy shadows in both middle-lower lungs; enlarged and blurry lung hilum; costophrenic angle unclear.
By chest X-ray on Nov. 20th, 2009(Fig. 11.60b), multiple flaky cloudy shadows in both middle-lower lungs; enlarged and blurry lung hilum; improved conditions compared to chest X-ray on Nov. 19th, 2009.
By chest X-ray on Nov. 23rd, 2009 (Fig. 11.60c), multiple flaky cloudy shadows in both middle-lower lungs; enlarged and parenchymal changes of lung hilum; progressive conditions compared to chest X-ray on Nov. 19th, 2009.
By chest X-ray on Nov. 24th, 2009 (Fig. 11.60d), large flaky cloudy shadows in both lungs; obviously deteriorated conditions compared to chest X-ray findings on Nov. 23rd, 2009.
By chest X-ray on Nov. 25th, 2009 (Fig. 11.60e), flaky flocculent cloudy shadows in both lungs; increased transparency of both lungs compared to chest X-ray findings on Nov. 23rd, 2009, obviously improved condones.
Pathologic Tissues Analysis
Figure 11.60f–g: By H&E staining, widened space between alveolar walls; Alveolar wall congestion; neutrophils and plasmacyte infiltrated, dominantly monocytes; alveolar edema fluid and fibrin exudated.
Figure 11.60h–i: By H&E staining, many inflammatory cells in the space between cardiac muscle tissues.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.60
Case 11.61
History of Present Illness. A 38-years-old man, complained of fever for 3 days and spasmodic breathing for 1 day. He initially had chills, fatigue, dizziness and cough; no sore throat and runny nose; followed by spasmodic breathing and dyspnea. Blood gas analysis indicated type I respiratory failure and metabolic acidosis.
Past History. Histories of myocarditis, hypertension, cardiac failure.
Contact History. Self reported history of contacting with a patient with fever who was receiving vaccines for Influenza A (H1N1).
Signs. Body temperature 39.6 °C; blood pressure 75/58 mmHg.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive and specific gene of Influenza A (H1N1) virus (gene HA) positive.
By routine blood tests on Oct. 29th, 2009, leukocytes count 6.64 × 109/L, neutrophils 89.8 % and lymphocytes 6.0 %.
By blood gas analysis: pH 7.423, PaO2 78.4 mmHg and PaCO2 37.2 mmHg.
By liver function tests on Oct. 30th, 2009, ALT 187.2 U/L and AST 148.2 U/L.
Diagnostic Imaging
By chest X-ray on Oct. 28th, 2009 (Fig. 11.61a): multiple flaky flocculent cloudy shadows in both lungs, more obvious in both middle-lower lungs; hilum structure of both lungs blurry.
By chest X-ray on Oct. 30th, 2009 (Fig. 11.61b): multiple flaky flocculent cloudy shadows in both middle-lower lungs; some foci absorbed and improved conditions compared to chest X-ray findings on Oct. 28th, 2009.
By chest X-ray on Nov. 2nd, 2009 (Fig. 11.61c): increased lung markings; no other abnormalities.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.61
Case 11.62
History of Present Illness. A 17-years-old man, complained of fever for 6 days and cough for 4 days, with dyspnea and chest pain for 1 day. After hospitalization for 14 days, he was cured. At 9 p.m. on Oct. 24th, 2009, he started to have fever, with the highest body temperature of 38 °C. The fever was irregular, with chills and headache. On the next day, runny nose occurred, with recurrent fever of higher body temperature afternoons and his temperatures above 38 °C. On Oct. 26th, 2009, throat upset occurred, with paroxysmal dry cough, no sore throat and hoarse voice. Dyspnea occurred last night, with accompanying continuous dull chest pain that was worse when lying down and relieved when sitting up. He also coughed, with a little rusty phlegm but no blood. He was clinically diagnosed as acute type I respiratory failure secondary to pneumonia complicating to critical Influenza A (H1N1).
Past History. None.
Contact History. In the school he was studying in, many students had fever and some was diagnosed as Influenza A (H1N1). Self reported history of contacting with patients definitively diagnosed as Influenza A (H1N1).
Signs. Body temperature 39.1 °C; heart rate 133 beats/min, breathing rate 24 times/min and blood pressure 95/54 mmHg. He was conscious, but with slight shortness of breath. Pharyngeal congestion obvious. No retropharyngeal folliculosis. Bilateral tonsils swollen to II degree.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive and specific gene of Influenza A (H1N1) virus (gene HA) positive.
By routine blood tests, hemoglobin 153 g/L, leukocytes count 10.41 × 109/L, and neutrophils 80.1 %.
By blood gas analysis, pH 7.46, PaCO2 32 mmHg, PaO2 58.8 mmHg, AB 22.2 mmol/L and BE −1.6 mmol/L.
By blood biochemistry, K+ 4.38 mmol/L, Na+ 134.7 mmol/L, CK 1631.1 mmol/L, LDH 228.9 mmol/L and GOT 50.3 U/L.
By the four coagulation indices test, PT 14.5 s and PTA 59.3 %.
Diagnostic Imaging
By chest X-ray on Oct. 30th, 2009 (Fig. 11.62a), large flaky cloudy shadows with increased density in both lower lungs; enlarged and thickened hilum of the right lung.
By chest CT scanning on Oct. 30th, 2009 (Fig. 11.62b1–c2), symmetrical large flaky shadows with increased density in posterior basal segments of both lower lungs, with gas bronchogram.
Figure 11.62d1–e2: pulmonary tissues parenchymal changes in mediastinal window.
By chest CT scanning on Nov. 2nd, 2009 (Fig. 11.62f1–l), symmetrical large flaky shadows with increased density in posterior basal segments of both lower lungs, with gas bronchogram; improved conditions compared to chest X-ray findings on Oct. 30th, 2009.
By chest CT scanning on Nov. 5th, 2009 (Fig. 11.62m–t), symmetrical large flaky shadows with increased density in posterior basal segments of both lower lungs, with gas bronchogram; improved conditions compared to chest X-ray findings on Nov. 2nd, 2009.
By chest CT scanning on Nov. 9th, 2009 (Fig. 11.62u–x), increased and deranged lung markings; no other abnormalities; improved conditions compared to chest X-ray findings on Nov. 5th, 2009.
By chest X-ray on Nov. 9th, 2009 (Fig. 11.62y, z): no abnormalities in both lungs and cardiac diaphragm.
Diagnosis. Pneumonia complicating Influenza A (H1N1).





Fig. 11.62
Case 11.63
History of Present Illness. A 45-years-old man, complained of intermittent fever and cough for 5 days, with accompanying slight cough with a little whitish phlegm, no chills and runny nose.
Past History. None.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39 °C. Pharyngeal congestion with tonsils swollen to I degree. Moist rale in the right lung.
Laboratory Tests
Throat swabs by CDC on Nov. 17th, 2009 found universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive and specific gene of Influenza A (H1N1) virus (gene HA) negative.
By routine blood tests on Nov. 15th, 2009, leukocytes count 5.49 × 109/L, lymphocytes 23.7 % and neutrophils 66.5 %.
Diagnostic Imaging
By chest X-ray on Nov. 15th, 2009 (Fig. 11.63a), thickened lung markings of both lungs; decreased transparency of the right lower lung; patchy shadows in the right lower lung.
By chest X-ray on Nov. 18th, 2009 (Fig. 11.63b), thickened lung markings of both lungs; decreased transparency of both lungs; patchy shadows in the right lower lung; improved conditions compared to chest X-ray findings on Nov. 15th, 2009.
By chest X-ray on Nov. 20th, 2009 (Fig. 11.63c), patchy shadows in both lower lungs; no obvious changes compared to chest X-ray findings on Nov. 18th, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.63
Case 11.64
History of Present Illness. A patient complained of sore throat, dry cough and fever for 3 days, with runny nose but no chills and fatigue.
Past History. None.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 37.8 °C. Pharyngeal congestion. Tonsils not swollen.
Laboratory Tests
Throat swabs by CDC on July 29th, 2009, found universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) negative and specific gene of Influenza A (H1N1) virus (gene HA) positive.
By routine blood tests on Aug. 2nd, 2009, leukocytes count 4.8 × 109/L, lymphocytes 34.7 % and neutrophils 41.9 %.
Diagnostic Imaging
On July 31st, 2009 (Fig. 11.64), round liked shadows with increased density in the right lower lung, with blurry boundaries.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.64
Case 11.65
History of Present Illness. A 21-years-old woman, complained of fever and cough for 9 days, with accompanying cough with yellowish phlegm. No chills, convulsion, sore throat, nasal obstruction, rhinorrhea, chest pain and diarrhea. She received therapies of cefuroxime and Phlegm Heat Clearer prescribed by a physician from a nearby clinic with no favorable outcomes. Body temperatures between 38 and 38.7 °C. Cough and expectoration not relieved, with chest distress and shortness of breath.
Past History. None.
Contact History. Self reported no history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39.7 °C. Pharyngeal congestion. Tonsils swollen to I degree. Moist rale in both lungs but none after cough.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) negative and specific gene of Influenza A (H1N1) virus (gene HA) positive.
By routine blood tests on Nov. 10th, 2009, leukocytes count 8.64 × 109/L, neutrophils 76.14 % and lymphocytes 19.34 %.
By routine blood tests on Nov. 17th, 2009, leukocytes count 6.79 × 109/L, neutrophils 73.14 % and lymphocytes 14.74 %.
By blood biochemistry on Nov. 17th, 2009, T 62 g/L, A 25 g/L; By liver functions tests, ALT and AST normal; by renal functions test, BUN 2.6 mmol/L, Cr 62 μmol/L, uric acid 138 μmol/L, Ca2+ 2.07 mmol/L, cholinesterase 5,674 U/L, CK 140 U/L and LDH 547 U/L.
By blood biochemistry on Nov. 19th, 2009, liver functioning total protein T 63 g/L, albumin (A) 26 g/L, ALT and AST normal; K+ 3.41 mmol/L, BUN 1.8 mmol/L, uric acid 137 μmol/L, cholinesterase 6,204 U/L, CK 91 U/L, LDH 470 U/L and Glu 8.42 mmol/L.
On Nov. 19th, 2009 sub-types of T-lymphocyte, CD4+ 259 × 106/L, CD8+ 142 × 106/L, CD4+/CD8+ 1.82.
By HBV-M, HCVAb (−), HAVIgM (−), HIVAb (−) and syphilis (−).
ESR 98 mm/h.
On Nov. 18th, 2009, sputum smearing found no acid-fast bacilli.
By arterial blood gas analysis on Nov. 19th, 2009, pH 7.542, PaO2 130 mmHg and PaCO2 28.3 mmHg.
Diagnostic Imaging. By chest X-ray on Nov. 14th, 2009 (Fig. 11.65a), large flaky shadows in the inner zone of the right middle-lower lung and the left lower lung, with blurry boundaries; several cavity shadows in both lower lungs, with blurry boundaries.
By chest CT scanning on Nov. 14th, 2009 (Fig. 11.65b–m): flaky flocculent cloudy shadows in both lungs fields; parenchymal shadows in the left lower lung; thin walled cavities and dilated bronchi shadows in both upper lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).



Fig. 11.65
Case 11.66
History of Present Illness. A 23-years-old man, complained of fever and cough for 4 days, with accompanying rhinorrhea.
Past History. Chronic gastroenteritis for more than 10 years. Icterohepatitis in childhood.
Contact History. Some students from the school he was studying in were diagnosed as Influenza A (H1N1).
Signs. Body temperature 39.7 °C. Pharyngeal congestion. Tonsils swollen to I degree. Coarse respiration sound in both lungs, with no moist rale.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) negative and specific gene of Influenza A (H1N1) virus (gene HA) positive.
By routine blood tests on Nov. 6th, 2009, leukocytes count 11.72 × 109/L, neutrophils 84.01 % and lymphocytes 6.32 %.
By blood biochemistry on Nov. 6th, 2009, liver function: T 62 g/L, A 35 g/L; AST 123 U/L and ALT 142 U/L; renal function: BUN 13.7 mmol/L, uric acid 494 μmol/L; electrolytes: Na+ 127 mmol/L, Cl− 87 mmol/L, Ca2+ 1.94 mmol/L and CK 207 U/L.
By routine urine tests, protein (+).
By routine blood tests on Nov. 9th, 2009, leukocytes count 6.38 × 109/L, neutrophils 33.64 % and lymphocytes 38.74 %.
By blood biochemistry on Nov. 9th, 2009, T 65 g/L, A 34 g/L, AST 44 U/L and ALT 69 U/L.
The Five indices of blood infection, WNL.
ECG: normal.
Diagnostic Imaging
By B-mode ultrasound on Nov. 7th, 2009 (Fig. 11.66a): diffusive echo of hepatic parenchyma with slight changes; spleen thickness 4.8 mm.
By chest CT scanning on Nov. 5th, 2009 (Fig. 11.66b–f): decreased transparency of the right lung, with flaky shadows; small flaky shadows in the left lower lung beside the heart margin.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.66
Case 11.67
History of Present Illness. A 50-years-old man, complained of cough and fever for a week. He was hospitalized due to deteriorating conditions for 1 day. He also had chest distress, spasmodic breathing and cough up yellowish phlegm.
Past History. Type II diabetes.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39.8 °C. Pharyngeal congestion. Edema.
Diagnosis. Critical Influenza A (H1N1); pneumonia of both lungs; Type I respiratory failure; metabolic acidosis; renal dysfunctioning; hypertension (extremely critical).
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive and specific gene of Influenza A (H1N1) virus (gene HA) positive.
By blood gas analysis on Nov. 12th, 2009, pH 7.318, PaCO2 36.8 mmHg and PaO2 48.8 mmHg.
Liver function: ALT 349 U/L, AST 52 U/L and TBil 9.1 U/L.
ECG: sinus bradycardia; borderline ECG.
By blood gas analysis on Nov. 3rd, 2009, pH 7.143, PaCO2 82.5 mmHg and PaO2 27.4 mmHg.
Diagnostic Imaging
By chest X-ray on Nov. 2nd, 2009 (Fig. 11.67), blurry lung markings of both lungs; decreased transparency of both lungs; patchy shadows in both middle-lower lungs, with blurry boundaries.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.67
Case 11.68
History of Present Illness. A 54-years-old woman, complained of fever for 6 days and cough for 4 days and was hospitalized. She had persistent fever, cough with phlegm (a little odorless whitish phlegm).
Past History. None.
Contact History. Denied history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39 °C. Pharyngeal congestion. Tonsils not swollen. Moist rale in both lungs.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
By blood gas analysis on Nov. 14th, 2009, pH 7.469, PaCO2 37.6 mmHg and PaO2 71 mmHg.
By routine blood tests, leukocytes count 4.93 × 109/L, lymphocytes 10.3 % and neutrophils 87.5 %.
By blood gas analysis on Nov. 15th, 2009, pH 7.382, PaCO2 39.4 mmHg and PaO2 54.1 mmHg.
By routine blood tests, leukocytes count 4.95 × 109/L, lymphocytes 17.0 % and neutrophils 77.5 %.
By liver function test on Nov. 16th, 2009, ALT 101.8 U/L and AST 120.4 U/L.
By blood gas analysis, pH 7.418, PaCO2 48 mmHg and PaO2 135.5 mmHg.
Diagnostic Imaging
By chest X-ray on Nov. 14th, 2009 (Fig. 11.68a): large flaky shadows with increased density in both middle-lower lungs; decreased transparency of both lungs; thickened hilum of both lungs.
By chest X-ray on Nov. 17th, 2009 (Fig. 11.68b): flaky shadows with increased density in both middle-lower lungs; progressive conditions compared to chest X-ray findings on Nov. 14th, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.68
Case 11.69
History of Present Illness. A 21-years-old man, complained of fever, sore throat and dry cough for 2 days, with chills, shivering, sore throat and cough.
Past History. None.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 38.9 °C. Pharyngeal congestion. Tonsils swollen to II degree.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
By routine blood tests on July 5th, 2009, leukocytes count 3.0 × 109/L, lymphocytes 38.9 % and neutrophils 44.56 %.
By routine blood tests on July 7th, 2009, leukocytes count 3.2 × 109/L, lymphocytes 53.6 % and neutrophils 32.3 %.
Diagnostic Imaging
By chest X-ray on July 7th, 2009 (Fig. 11.69), flaky and strip liked shadows in inner zone of the left upper lung; enhanced lung markings; increased and thickened pulmonary hilum.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.69
Case 11.70
History of Present Illness. A 19-years-old man, complained of fever and cough for 1 day, with chills, slight cough and headache.
Past History. None.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 38.9 °C. Pharyngeal congestion. Tonsils not swollen. Moist rale in both lungs.
Laboratory Tests
Throat swabs by CDC found universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive and specific gene of Influenza A (H1N1) virus (gene HA) negative.
By liver function test on Oct. 28th, 2009, ALT 25.1 U/L, AST 32.2 U/L and CK 452.9 U/L.
By throat swabs on Oct. 30th, 2009, negative findings.
Diagnostic Imaging
By chest X-ray on Oct. 30th, 2009 (Fig. 11.70): increased lung markings of both lungs; cloud mist liked shadows with increased density; enlarged and thickened pulmonary hilum.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.70
Case 11.71
History of Present Illness. A 2-years-old boy, had chief complaints of fever and cough for 2 days, with runny nose but no chills and fatigue.
Past History. None.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39.6 °C. Pharyngeal congestion. Tonsils swollen to I degree.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive and specific gene of Influenza A (H1N1) virus (gene HA) positive.
By routine blood tests, leukocytes count 5.9 × 109/L, lymphocytes 51.6 %, neutrophils 42.6 % and platelets count 190 × 109/L.
Diagnostic Imaging
By chest X-ray on Nov. 1st, 2009 (Fig. 11.71a), diffusive patchy shadows in both lungs; blurry lung markings, predominantly in the right lung.
By chest X-ray on Nov. 2nd, 2009 (Fig. 11.71b), blurry pulmonary markings of both lungs; enlarged and thickened hilum, predominantly in the both lower lungs; improved conditions compared to chest X-ray findings on Nov. 2nd, 2009.
Diagnosis. Pneumonia complicating critical Influenza A (H1N1).

Fig. 11.71
Case 11.72
History of Present Illness. A patient complained of fever and cough for 3 days. Phlegm difficult expectorating; diarrhea but no chills and fatigue.
Past History. None.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39 °C. Pharyngeal congestion. Tonsils swollen to I degree. Moist rale in both lungs.
Laboratory Tests
By throat swabs on Nov. 12th, 2009, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) negative, specific gene of Influenza A (H1N1) virus (gene HA) negative.
By routine blood tests on Nov. 13th, 2009, leukocytes count 4.119 × 109/L, lymphocytes 51.6 % and neutrophils 36.5 %.
Diagnostic Imaging
By chest X-ray on Nov. 12th, 2009 (Fig. 11.72a), small flaky cloudy shadows in the left lower lung.
By chest X-ray on Nov. 14th, 2009 (Fig. 11.72b), multiple small patchy cloudy shadows in both lower lungs; blurry lung markings; no obvious changes compared to chest X-ray findings on Nov. 12th, 2009.
By chest X-ray on Nov. 16th, 2009 (Fig. 11.72c), cloud mist liked blurry shadows in both lower lungs; blurry lung markings; enlarged and thickened pulmonary hilum; progressive conditions compared to chest X-ray findings on Nov. 14th, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.72
Case 11.73
History of Present Illness. A 37-years-old man, complained of fever and cough for 7 days, with expectoration of whitish or yellowish phlegm.
Past History. None.
Contact History. Denied history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39 °C. Pharyngeal congestion. Tonsils not swollen. Coarse respiration sound in both lungs. No moist rale. Heart rate 100 beats/min.
Laboratory Tests
Throat swabs by CDC found universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) negative, specific gene of Influenza A (H1N1) virus (gene HA) negative.
By routine blood tests on Nov. 13th, 2009, leukocytes count 9.4 × 109/L, neutrophils 83.6 % and lymphocytes 12.2 %.
By blood biochemistry on Nov. 17th, 2009, liver function tests: T 65 g/L, A 31 g/L, AST 46 U/L, ALT 56 U/L; renal function BUN normal, uric acid 180 μmol/L; electrolytes Cl− 92 mmol/L, cholinesterase normal, CK 365 U/L, LDH 257 U/L; alkaline phosphatase 134 U/L, γ-GT 42 U/L.
By routine urine tests, URO (+). CRP on 2009-11-19, 20.50 mg/L.
ESR 5 mm/h.
By HBV-M, HbeAb (+), HCVAb (−), HAVIgM (−), HIVAb (−), syphilis (−).
Sub-types of T-lymphocytes counts, CD4+ 328 × 106/L, CD8+ 199 × 106/L, and CD4+/CD8+ 1.6.
Sputum culture on Nov. 19th, 2009 negative.
Diagnostic Imaging
By chest X-ray on Nov. 15th, 2009 (Fig. 11.73a), increased and blurry lung markings of both lower lungs; cloud mist liked shadows with increased density; enlarged and thickened pulmonary hilum.
By chest CT scanning on Nov. 16th, 2009 (Fig. 11.73b–k), large flaky blurry shadows in posterior basal segments of both lungs; parenchymal changes of some pulmonary tissues; gas bronchogram more obvious in the right lung.
Diagnosis. Pneumonia complicating Influenza A (H1N1).



Fig. 11.73
Case 11.74
History of Present Illness. A 39-years-old woman, complained of cough deterioration and fever for 5 days, with headache, chills, muscle soreness, fatigue and expectoration of whitish thick phlegm.
Past History. None.
Contact History. Self reported of coming from the epidemic area of Influenza A (H1N1).
Signs. Body temperature 39 °C. Pharyngeal congestion. Tonsils swollen to I degree. Moist rale in both lungs.
Laboratory Tests
By throat swabs on Nov. 19th, 2009, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) negative, specific gene of Influenza A (H1N1) virus (gene HA) negative.
By routine blood tests, leukocytes count 3.39 × 109/L and neutrophils 70.25 %.
By routine blood tests on Nov. 22nd, 2009, leukocytes count 2.72 × 109/L, lymphocytes 36.4 % and neutrophils 53.2 %.
Diagnostic Imaging
By chest X-ray on Nov. 22nd, 2009 (Fig. 11.74), thickened lung markings of both lungs; patchy blurry shadows in both middle-lower lungs; both diaphragmatic surfaces blurry.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.74
Case 11.75
History of Present Illness. A 40-years-old man, complained of fever and cough for 5 days and dyspnea for 1 day, with chills and chest distress.
Past History. None.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39 °C. Pharyngeal congestion. Tonsils not swollen.
Laboratory Tests
By throat swabs on Nov. 16th, 2009, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) negative.
By routine blood tests, leukocytes count 2.83 × 109/L, lymphocytes 37.1 % and neutrophils 59.4 %.
By blood gas analysis, pH 7.512, PaCO2 30 mmHg and PaO2 34 mmHg.
Diagnostic Imaging
By chest X-ray on Nov. 16th, 2009 (Fig. 11.75a): increased pulmonary markings of both lungs; flaky blurry shadows in both lower lungs; enlarged and thickened pulmonary hilum.
By chest X-ray on Nov. 17th, 2009 (Fig. 11.75b): increased pulmonary markings of both lungs; flaky blurry shadows in both lower lungs; improved conditions compared to chest X-ray findings on Nov. 16th, 2009.
By chest X-ray on Nov. 18th, 2009 (Fig. 11.75c): increased pulmonary markings of both lungs; flaky blurry shadows in both lower lungs; no obvious changes compared to chest X-ray findings on Nov. 17th, 2009.
By chest X-ray on Nov. 20th, 2009 (Fig. 11.75d): cloud mist liked shadows in both lungs fields; decreased transparency of both lungs; slightly progressive conditions compared to chest X-ray findings on Nov. 17th, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.75
Case 11.76
History of Present Illness. A 16-years-old boy, complained of recurrent chest distress and suffocation for 4 years, with fever and cough for 4 days.
Past History. Self reported diagnosis of asthma 4 years ago.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 37 °C. Mental conditions good. Pharyngeal congestion.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
Diagnostic Imaging
By chest CT scanning on Nov. 4th, 2009 (Fig. 11.76a–g), scattered ground glass liked of flaky flocculent shadows in both lungs; bronchial walls thickened.
By chest CT scanning on Nov. 9th, 2009 (Fig. 11.76h–o): thickened pulmonary markings of both lungs; improved conditions compared to chest CT scanning on Nov. 4th, 2009.
By chest CT scanning on Nov. 11th, 2009 (Fig. 11.76p–t): increased pulmonary markings of both lungs; obviously improved conditions compared to chest CT scanning on Nov. 4th, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).



Fig. 11.76
Case 11.77
History of Present Illness. A 37-years-old man, complained of intermittent cough with yellowish thick phlegm.
Past History. None.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 37 °C. Breathing rate 18–24 times/min. Heart rate 69–84 beats/min. Blood pressure (100–110)/(66–70) mmHg. Pharyngeal congestion. Respiration sound of both lungs low, with rare or moderate fine moist rale in both lower lungs but no dry rale. Cardiac border slightly enlarged toward left, with heart rate 98 beats/min.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
Diagnostic Imaging
By chest CT scanning on Nov. 5th, 2009 (Fig. 11.77a–f), large flaky shadows with increased density in posterior basal segments of both lower lungs.
By chest CT scanning on Nov. 6th, 2009 (Fig. 11.77g–l), large flaky shadows with increased density in posterior basal segment of both lower lungs; improved conditions compared to chest CT scanning on Nov. 5th, 2009.
By chest CT scanning on Nov. 7th, 2009 (Fig. 11.77m–r), large flaky shadows with increased density in posterior basal segment of both lower lungs; improved conditions compared to chest CT scanning on Nov. 6th, 2009.
By chest CT scanning on Nov. 10th, 2009 (Fig. 11.77s–x), flaky shadows with increased density in posterior basal segment of both lower lungs; improved conditions compared to chest CT scanning on Nov. 5th, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).





Fig. 11.77
Case 11.78
History of Present Illness. A 19-years-old man, complained of fever for 6 days and dyspnea with cough and expectoration for 5 days.
The patient suffered from fever due to catching a cold 6 days before his hospitalization, with the highest temperature 38 °C. He also had cough, difficulty breathing, expectoration of yellowish and sometimes blood phlegm. The sputum small in amount. Diagnosis on admission:
-
(1)
critical Influenza A (H1N1).
-
(2)
critical pneumonia; type 2 respiratory failure; ARDS.
-
(3)
multiple organs dysfunction.
Past History. Denied history of major basic diseases.
Contact History. Denied history of contacting with Influenza A (H1N1) patients and suspected patients with flu liked symptoms.
Signs. Pharyngeal congestion. Body temperature 39 °C.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
By blood biochemistry, electrolytes Na+ 94.2 %, Myo 131 ng/L, CK-MB 7.68 ng/L, troponin not abnormal.
By blood gas analysis, pH 7.53, PaCO2 27.1 mmHg and PaO2 52 mmHg.
Diagnostic Imaging
By CT scanning on Nov. 20th, 2009 (Fig. 11.78a–d), diffusive patchy shadows and parenchymal shadows in the right middle and lower lung, the left upper lung, lingular segments of the left upper and lower lung and the left lower lung; enlarged cardiac shadow; a little effusion of both chest cavities.
Laboratory Tests
By blood biochemistry, ALT 46 U/L, AST 92 U/L, albumin 40 g/L, globulin 29.6 g/L mmol/L, PA 140 mg/L, CRP 325.2 mg/L, K+ 4.56 mmol/L, Na+ 132.6 mmol/L, Cl− 93.4 mmol/L; CK 12,261 U/L, CK-MB 30 U/L, LDH 764 U/L, HBDH 524 U/L, myocardial enzymospectrum high, anti-“O” 73 IU/L, ESR 72 mm/h; by coagulation tests, PTA 63.1 %, PT-INR 1.22, d-dimer negative.
By routine blood tests, leukocytes count 4.91 × 109/L.
By blood gas analysis, pH 7.49, PaCO2 36 mmHg, PaO2 92 mmHg, BE 5.2 mmol/L, \( {\text{HCO}}_{3}^{-}\) 27.7 mmol/L, SpO2 97 %, K+ 4.6 mmol/L, Na+ 137 mmol/L, IPAP 15 cm H2O, EPAP 12 cm H2O and FiO2 50 %.
Signs. Body temperature 37.8 °C. Heart rate 70 beats/min. Breathing rate 29 times/min. Blood pressure 117/82 mmHg, SpO2 98 %. Conscious. Pharyngeal congestion. Respiration sounds low. A great amount of moist rale of both lungs.
By blood biochemistry on Nov. 23rd, 2009, ALT 41 U/L, AST 67 U/L, albumin 35.1 g/L, globulin 31.5 g/L mmol/L, PA 94 mg/L, CRP 298.1 mg/L, K+ 4.38 mmol/L, Na+ 133.5 mmol/L, Cl− 96.8 mmol/L. CK 818 U/L, CK-MB 28 U/L, LDH 786 U/L, HBDH 554 U/L, myocardial enzymospectrum high, anti-“O” 73 U/L, ESR 72 mm/h; by coagulation tests, PT 10.8 s, PTa 63.1 %, PT-INR 1.22 s, d-dimer negative.
By routine blood tests, leukocytes count 7.9 × 109/L.
By blood gas analysis, pH 7.38, PaCO2 56 mmHg, PaO2 150 mmHg, BE 5.6 mmol/L, \( {\text{HCO}}_{3}^{-}\) 32.4 mmol/L, Na+ 135 mmol/L, K+ 4.5 mmol/L and SaO2 99 %.
ECG Monitoring. Body temperature 37.0 °C. Heart rate 76 beats/min. Breathing rate 24 times/min. Blood pressure 110/70 mmHg. SpO2 96 %.
Signs. Pharyngeal congestion. Respiration sounds in both lungs low. Decreased moist rales.
ECG. Sinus rhythm; atrioventricular block of I degree.
Diagnostic Imaging
By chest CT scanning on Nov. 23rd, 2009 (Fig. 11.78e–j), pulmonary tissues of both lungs gathering toward hilum; pulmonary markings gathering; no pulmonary markings in the middle-lateral zone of the lung but gas shadows; dense parenchymal shadows in the posterior basal segment of both lungs; bilateral pneumothorax and about 70 % compressed pulmonary tissues of both lungs compared to chest CT scanning on Oct. 20th, 2009.
Laboratory Tests
On Nov. 25th, 2009, ESR 66 mm/h. d-dimer positive. By routine blood tests, leukocytes count 9.8 × 109/L.
By blood biochemistry, ALT 55 U/L, AST 50 U/L, TB 27.3 mmol/L, CRP 115.3 mg/L, BUN 7.43 mmol/L, Glu 10.14 mmol/L, NA 131.4 mmol/L, CK 241 U/L, CK-MB 18 U/L. LDH 542 U/L, HBDH 415 U/L, myocardial enzymospectrum lower than before, IgG 23.41 g/L, LACT 3.7 mmol/L.
Signs. Acute appearance. Shortness of breath. Facial blushing. SpO2 80–90 %. Breathing rate 45 times/min. Heart rate 105 beats/min. Respiration sounds of both lungs lower. Tracheal migration not obvious.
Diagnostic Imaging
By chest CT scanning on Nov. 25th, 2009 (Fig. 11.78k–n), strip liked gas shadows in the external zone of both lungs; 30 % compressed pulmonary tissues of both lungs; lung volume of both lungs decreased; gathered pulmonary markings; parenchyma changes of both lower lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.78
Case 11.79
History of Present Illness. A 20-years-old man, athlete, Georgians, complained of fever for 30 h.
Past History. None.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 37.2 °C. Pharyngeal congestion. Rare moist rales in the left lower lung.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
Diagnostic Imaging
By chest CT scanning on Nov. 6th, 2009 (Fig. 11.79a–f), flaky shadows with increased density in posterior basal segment of the right lung, with blurry boundaries; increased and thickened pulmonary markings of the rest lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.79
Case 11.80
History of Present Illness. A 35-years-old man, complained of fever, cough and expectoration for 6 days, and worsened conditions for 3 days. He also had chills, headache, general soreness, paroxysmal cough with small amount of whitish foamy phlegm. The cough deteriorated 3 days ago, with large amount of whitish foamy phlegm about 60 mL per day and occasional bloody phlegm.
Past History. Denied histories of major basic diseases.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 38.7 °C. Pharyngeal congestion by physical examination on Nov. 24th, 2009. Moist rales in both lower lungs. Heart rate 71 beats/min. Heart rate regular. Breathing rate 23 times/min. Blood pressure 105/75 mmHg.
Laboratory Tests
By throat swabs on Nov. 20th, 2009, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
By routine blood tests, leukocytes count 11.1 × 109/L, hemoglobin 154 g/L. By coagulation tests, PT 9.3 s, PTA 154.5 % and APTT 26.9 s.
By blood biochemistry, ALT 81 U/L, AST 39 U/L, PA 351 mg/L, CK 37 U/L, CK-MB 12 U/L, HBDH 139 U/L, LDH 174 U/L, blood lactate 1.7 mmol/L, renal function and electrolytes normal, improved liver function.
Humoral Immunity: IgG 22.05 g/L and the other indices normal.
By sputum smear, a great amount of G+ coccus; a small amount of G− coccus and G− bacillus.
Diagnostic Imaging
By chest CT scanning on Nov. 24th, 2009 (Fig. 11.80a–f): flaky shadows with increased density in internal segment and basal segment of the both lower lungs; thickened bilateral pleura.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.80
Case 11.81
History of Present Illness. A 32-years-old man, complained of fever, cough and sore throat for 6 days, and shortness of breath for 2 days. The highest body temperature 41 °C, with sore throat, cough and occasional expectoration of a little whitish foamy phlegm.
On Nov. 14th, 2009, the patient started to have orthopnoea and bloody sputum. His spirituality and appetite remained poor. On Nov. 16th, 2009, he had bad coughs with a little pink foamy phlegm. Moist wheezing diffused in both lungs, especially in the right lung.
On Nov. 18th, 2009, he had no fever, but occasional coughs with a little yellowish phlegm. By physical examinations, pharyngeal congestion; tonsils swollen to I degree; moist wheezing in both lungs obviously decreased.
On Nov. 19th, 2009, he coughed a little mucoid phlegm with blood after getting up in the morning. By physical examination, pharyngeal congestion; moist wheezing in both lungs obviously decreased, with no dry wheezing.
On Nov. 20th, 2009, he had bad coughs with a little mucous bloody phlegm. By physical examination, pharyngeal congestion; moist wheezing in both lungs obviously decreased, with occasional dry wheezing.
Past History. None.
Contact History. Self reported history of contacting with patients suffering from flu liked symptoms within 1 week. Denied history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 36.7 °C. Heart rate 107 beats/min. Breathing rate 25 times/min. Blood pressure 119/79 mmHg, SpO2 88 %. Appearance of acute diseases. Orthopnoea. Conscious. Spirituality good. Pharyngeal congestion. The tonsils swollen to I degree. Shortness of breath. Much moist wheezing in both lungs. Dry wheezing in the right middle-lower lung.
Laboratory Tests
Throat swabs by CDC found universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
By blood gas analysis on Nov. 14th, 2009, pH 7.4, PaCO2 24.6 mmHg, PaO2 51 mmHg, BE 10 mmol/L, K+ 4.3 mmol/L and SaO2 87 %.
By routine blood tests, leukocytes count 8.2 × 109/L, neutrophils 84.8 %, platelets count 95 × 109/L, hemoglobin 167 g/L, PT 12.5 s, d-dimer negative.
By blood biochemistry, ALT 58 U/L, AST 97 U/L, albumin 40.3 g/L, globulin 46 g/L mmol/L, BUN 14.12 mmol/L, uric acid 630/L, ALP 224 U/L, CRP 128.9 mg/L, K+ 4.86 mmol/L, Na+ 127.6 mmol/L, Cl− 95.8 mmol/L. CK 2,232 U/L, CK-MB 58 U/L. LDH 582 U/L, HBDH 758 U/L, myocardial enzyme obviously abnormal.
EGC. ST-T changes; Intraventricular block; suspected viral myocarditis.
Laboratory Tests. Leukocytes count 8.1 × 109/L; by urine test, SG 1.030, BLD (++) and PRO (++).
By immune cells tests on Nov. 17th, 2009, CD3+ 205 × 106/L, CD4+ 93 × 106/L, CD8+ 108 × 106/L.
By blood biochemistry, ALT 55 U/L, AST 85 U/L, albumin 39.3 g/L, globulin 23.6 g/L mmol/L, CRP 124.6 mg/L, K+ 5.22 mmol/L, Na+ 128.9 mmol/L, Cl− 95.8 mmol/L. CK 190 U/L, CK-MB 48 U/L. LDH 697 U/L, HBDH 516 U/L, myocardial enzyme slightly decreased.
By blood gas analysis, pH 7.49, PaCO2 33.5 mmHg, PaO2 71 mmHg, BE 2 mmol/L, \( {\text{HCO}}_{3}^{-}\) 25.2 mmol/L, SpO2 95 %, K+ 4.0 mmol/L, Na+ 136 mmol/L.
By blood biochemistry on Nov. 18th, 2009, ALT 51 U/L, AST 66 U/L, albumin 35.6 g/L, globulin 26.6 g/L mmol/L, CRP 47.9 mg/L, K+ 4.45 mmol/L, Na+ 132.6 mmol/L, Cl− 98 mmol/L. CK 629 U/L, CK-MB 40 U/L. LDH 630 U/L, HBDH 492 U/L, myocardial enzyme slightly decreased; blood lactate 3 mmol/L.
By routine blood tests, leukocytes count 5.3 × 109/L, GR 82.8 %, hemoglobin 111 g/L, platelets count 23 × 109/L. Fecal bacterial proportion, positive coccus 50 %, negative coccus 50 %. HBV-M indicated HBsAb positive.
By blood gas analysis, pH 7.51, PaCO2 32.5 mmHg, PaO2 63 mmHg, BE 3 mmol/L, \( {\text{HCO}}_{3}^{-}\) 26.0 mmol/L, SpO2 94 %, K+ 4.0 mmol/L, Na+ 139 mmol/L.
By blood biochemistry on Nov. 20th, 2009, ALT 123 U/L, AST 74 U/L, albumin 37.1 g/L, CRP 4.2 mg/L, K+ 3.78 mmol/L, Na+ 137.4 mmol/L, Cl− 100.3 mmol/L. CK 394 U/L, CK-MB 20 U/L. LDH 388 U/L, HBDH 298 U/L, LACT 3.2 mmol/L.
By routine blood tests, leukocytes count 8.2 × 109/L, hemoglobin 139 g/L, platelets count 193 × 109/L.
ESR: 16 mm/h, PT normal.
By sputum smear, positive coccus and a little negative coccus; negative bacillus and fungal spores.
By blood gas analysis, pH 7.49, PaCO2 35 mmHg, PaO2 62 mmHg, BE 3.1 mmol/L, \( {\text{HCO}}_{3}^{-}\) 25.7 mmol/L, SaO2 94 %, K+ 4.4 mmol/L, Na+ 136 mmol/L.
By blood biochemistry on Nov. 22nd, 2009, ALT 222 U/L, AST 109 U/L, TBIL 25.2 μmol/L, CK 683 U/L, Glu 11.73 mmol/L, Cysc 1.21 mg/L, CO2 16.9 mmol/L, HBDH 293 U/L, LDH 427 U/L, IgG 6.09 g/L, LACT 2.6 mmol/L.
By routine blood tests, leukocytes count 10.6 × 109/L, lymphocytes 6.8 %.
Diagnostic Imaging
CT scanning on Nov. 14th, 2009 (Fig. 11.81a–h), patchy shadows and ground glass liked shadows in both lungs, especially in posterior basal segment of both lower lungs.
By chest X-ray on Nov. 17th, 2009 (Fig. 11.81i), cloud mist ground glass liked shadows with increased density in both lungs; blurry pulmonary hilum.
By chest X-ray on Nov. 18th, 2009 (Fig. 11.81j), cloud mist ground glass liked shadows with increased density slightly faded; increased transparency of both lungs compared to chest X-ray findings on Nov. 17th, 2009.
By chest CT scanning on Nov. 20th, 2009 (Fig. 11.81k–q), absorbed shadows and improved conditions of both lungs compared to chest CT scanning on Nov. 15th, 2009, increased transparency of both lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).



Fig. 11.81
Case 11.82
History of Present Illness. A 45-years-old man, complained of recurrent cough and fever for 10 days.
Past History. He was diagnosed as having acute myeloid leukemia M2a 10 months ago and received blood transfusion of ten units type O red blood cell suspensions and eight units platelet.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Pharyngeal congestion. Respiration sound in both lungs low, with a little moist wheezing in both lower lungs.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
Diagnostic Imaging
By chest CT scanning on Nov. 16th, 2009 (Fig. 11.82a–f), increased and thickened lung markings; cloud mist liked blurry shadows in posterior basal segments of both lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.82
Case 11.83
History of Present Illness. A 23-years-old man, with a foreign nationality, complained of fever for 20 h.
Past History. None.
Contact History. Self reported traveling in several countries by airplane before coming to China.
Signs. Body temperature 39 °C. Heart rate 107 beats/min. Breathing rate 22 times/min. Blood pressure 110/80 mmHg. SpO2 98 %. Appearance of acute diseases. Lips cyanosis. Pharyngeal congestion. Dry wheezing in expiration phase of both lungs.
Laboratory Tests
By throat swabs on Nov. 6th, 2009, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
By physical examination on Nov. 8th, 2009, temperature 38.4 °C. Occasional coughs with a small amount of whitish foamy phlegm. Pharyngeal congestion. Respiration sound clear in both lungs, with no dry and moist wheezing.
ECG. Sinus tachycardia.
No obvious abnormalities in both lungs by chest CT scanning.
On Nov. 9th, 2009, throat soreness relieved. Occasional coughs with a little whitish foamy phlegm. Pharyngeal congestion. Respiration sound clear in both lungs. Heart rate 75 beats/min.
On Nov. 11th, 2009, he was cured and discharged.
Diagnostic Imaging
By chest CT scanning on Nov. 8th, 2009 (Fig. 11.83a–d), increased lung markings of both lungs; thickened bronchial walls.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.83
Case 11.84
History of Present Illness. A 19-years-old man, complained of fever, headache, sore throat, cough and vomiting stomach contents.
Past History. None.
Contact History. Self reported no history of having been to the epidemic area.
Signs. Pharyngeal congestion.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
Diagnostic Imaging
By chest X-ray on Nov. 12th, 2009 (Fig. 11.84), increased and deranged lung markings of both lungs; spotty flaky blurry shadows; enlarged and thickened pulmonary hilum.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.84
Case 11.85
History of Present Illness. A 52-years-old man, complained of fever for a week, cough for 4 days and dyspnea for 1 day. He also had hyperhidrosis, shortness of breath, fatigue and diarrhea for 5 times with yellowish loose stool. Symptomatic treatment was not effective but with occurrence of respiratory distress and orthopnoea.
Past History. None.
Contact History. Self reported no history of having been to the epidemic area.
Signs. The highest body temperature 38.5 °C. Appearance of acute diseases. Misery facial expressions. Face cyanosis. Respiratory distress. Conscious. Spirituality poor. Reluctant to talking. Lips cyanosis. Respiration sound low in both lungs. Moderate to much moist rale in both lungs, with a little dry wheezing.
Laboratory Tests
Throat swabs by CDC on Nov. 7th, 2009, nucleic acid of Influenza A (H1N1) virus positive.
By routine blood tests on Nov. 7th, 2009, leukocytes count 5.6 × 109/L, neutrophils 62.7 %, hemoglobin 12.7 g/L, platelets count 106 × 109/L. By blood gas analysis, pH 7.36, PaCO2 42 mmHg, PaO2 46 mmHg, BE 3.0 mmol/L and \( {\text{HCO}}_{3}^{-}\) 22.5 mmol/L.
By blood gas analysis on Nov. 9th, 2009, pH 7.479, PaCO2 40.1 mmHg, PaO2 76 mmHg, BE 6 mmol/L, \( {\text{HCO}}_{3}^{-}\) 29.8 mmol/L.
By blood gas analysis on Nov. 10th, 2009, pH 7.479, PaCO2 40.1 mmHg, PaO2 57 mmHg, BE 6 mmol/L, \( {\text{HCO}}_{3}^{-}\) 29.8 mmol/L and SpO2 96 %.
By blood gas analysis on Nov. 13th, 2009, pH 7.470, PaCO2 33.9 mmHg, PaO2 71 mmHg, BE 1 mmol/L, SpO2 95 %, \( {\text{HCO}}_{3}^{-}\) 24.7 mmol/L, Na+ 137 mmol/L, K+ 4.3 mmol/L.
By routine blood tests on Nov. 16th, 2009, leukocytes count 13.8 × 109/L, hemoglobin 119 g/L, platelets count 296 × 109/L.
By blood gas analysis, pH 7.449, PaCO2 35.6 mmHg, PaO2 69 mmHg, BE 1 mmol/L, \( {\text{HCO}}_{3}^{-}\) 24.7 mmol/L, SpO2 95 %.
By blood biochemistry, CK 217/L, HBDH 341 U/L, CK-MB 14 U/L, LDH 429 U/L.
By liver function tests, ALT 61 U/L, AST 42 U/L, γ-GT 318 U/L, ALB 38.7 g/L, TB 16.5 μmol/L, improved liver function.
By renal function tests, BUN 11 mmol/L, Glu 10.4 mmol/L, Cys-c 1.45 mmol/L; C-reactive protein 76.8 mg/L, LACT 4.6 mmol/L, APTT 28.8 s, PTA 67 %, d-dimer positive; and humoral immunity IgG 18.02 g/L; ESR 61 mm/h.
By sputum smear, a small amount of gram-negative bacilli.
Diagnostic Imaging
By chest X-ray on Nov. 7th, 2009 (Fig. 11.85a), diffusive cloudy shadows with increased density in both middle-lower lungs; decreased transparency of both lungs; enlarged and blurry hilum.
By chest X-ray on Nov. 8th, 2009 (Fig. 11.85b), diffusive cloudy shadows with increased density in the right middle-lower lung and in the left lung; decreased transparency of both lungs; enlarged and blurry hilum; slightly improved conditions compared to chest X-ray findings on Nov. 7th, 2009.
By chest X-ray on Nov. 9–10th, 2009 (Fig. 11.85c, d), flaky cloudy shadows with increased density in both lungs; decreased transparency of both lungs;0 obviously improved conditions compared to chest X-ray findings on 2009-11-8.
By chest X-ray on Nov.13–16th, 2009 (Fig. 11.85e, f), diffusive cloudy shadows with increased density in both lower lungs; decreased transparency of both lungs; enlarged and blurry hilum; expanded field with blurry dense shadows compared to chest X-ray findings on Nov. 9–10th, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.85
Case 11.86
History of Present Illness. A 15-years-old man, complained of fever for 4 days and cough, tightness in breathing and dyspnea for 3 days. He also had dizziness, sore throat, nasal obstruction, rhinorrhea, dry cough, fatigue, poor appetite, tidal fever, spontaneous sweating, gradual emaciation and difficulty coughing up yellowish thick phlegm.
Clinical Diagnosis: (1) Influenza A (H1N1) and severe pneumonia; Type I respiratory failure; septic shock; (2) Moderate anemia; (3) Hypoalbuminemia; (4) Coughing up blood to be diagnosed; (5) Mediastinal emphysema.
Past History. None.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39.3 °C. Generally poor conditions and poor nutrition. Appearance of acute diseases with pale face. Moderately anemic appearance. Spiritualities quite bad. Conscious. Reluctant to talking. Supine with high pillow. Warm extremities. Shortness of breath. Conjunctiva pale. Lips dry with no cyanosis. Pharyngeal congestion obvious. Bilateral tonsils not swollen. Respiration sound of the right lower lung slightly low. Large amount of fine moist wheezing in both middle-lower lungs, especially in the right lung.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
By routine blood tests on Sep. 18th, 2009, leukocytes count 27.33 × 109/L, neutrophils 80.7 % and hemoglobin 92 g/L.
By blood gas analysis, PaCO2 34 mmHg, PaO2 48 mmHg, SpO2 85 %; blood Na+ 132.2 mmol/L. By coagulation tests, PT 21.9 s and APTT 33.7 s.
By liver and renal functions tests on Sep. 25th, 2009, AST 81 U/L, ALT 270 U/L, TP 67.2 g/L, ALB 40.0 g/L, TBIL 3.9 μmol/L, BUN 4.0 mmol/L, Cr 54.0 μmol/L, UA 222 μmol/L, K+ 4.54 mmol/L, Na+ 131.4 mmol/L, Cl− 97.5 mmol/L, ESR 62 mm/h.
Electrolytes: Na+ in a low level but slightly increased than previous test results; myocardial enzymospectrum: CK 259.0 U/L, HBDH 283 U/L, LDH 283 U/L, CK-MB 26 U/L and decreased level of myocardial enzyme.
Diagnostic Imaging
By chest CT scanning on Sep. 18th, 2009 (Fig. 11.86a–d), small flaky parenchymal shadows in the right lower lung, with surrounding cloud mist liked shadows with increased density.
By chest CT scanning on Sep. 25th, 2009 (Fig. 11.86e–h), small flaky cloudy shadow in the right lower lung; improved conditions compared to chest CT scanning on Sep. 18th, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.86
Case 11.87
History of Present Illness. A 57-years-old woman, complained of abdominal pain in the right upper quadrant for 3 days, deteriorated with chest distress and suffocation for 2 days. Conscious disturbance. Paroxysmal migrating abdominal pain. Chest distress and dyspnea.
Past History. Chronic bronchitis for more than 20 years, long-term use of hormone. Edema of lower extremities. Denied histories of hypertension and diabetes but having symptoms of polyuria, polydipsia and polyphagia.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. In coma. Over-weight. Multiple ecchymosis in whole body. Severe edema in bulbar conjunctival. Left palpebral conjunctiva bleeding. Bilateral pupils are isocoria, sensitive to light. Diffusive moist wheezing in both lungs, with occasional dry wheezing. Heart rate 102 beats/min. No pathological murmurs in cardiac valvar areas. Abdominal girth 100 cm. Abdominal tension increased. Pitting edema in areas below elbow joints and below knee joints.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
By blood gas analysis on Nov. 13th, 2009, pH 7.141, PaCO2 19.1 mmHg, PaO2 60 mmHg, BE −22 mmol/L, K+ 5.2 mmol/L, SpO2 92 %.
By routine blood tests, leukocytes count 21.52 × 109/L, neutrophils 93 %, platelets count 88 × 109/L, hemoglobin 139 g/L.
By blood biochemistry, albumin 26.7 g/L, globulin 46 g/L, Glu 42.8 mmol/L, BUN 14.12 mmol/L, osmotic pressure 327 mmol/L.
By routine urine tests, urine keton (++++) and urine glucose (++++).
By blood gas analysis on Nov. 14th, 2009, pH 7.417, PaCO2 48 mmHg, PaO2 100 mmHg, BE 6 mmol/L.
By blood gas analysis on Nov. 16th, 2009, pH 7.509, PaCO2 43.3 mmHg, PaO2 52 mmHg, BE 11 mmol/L, \( {\text{HCO}}_{3}^{-}\)34.5 mmol/L, K+ 3.6 mmol/L.
By routine blood tests on Nov. 17th, 2009, leukocytes count 15.9 × 109/L, hemoglobin 117 g/L, neutrophils 87.5 %, platelets count 113 × 109/L, WBC and neutrophils percentage increased. CK 24 U/L, HBDH 297 U/L, CK-MB 19 U/L, LDH 383 U/L, Na+ 142.5 mmol/L, K+ 4.46 mmol/L.
By blood biochemistry, ALT 50 U/L, AST 48 U/L, ALB 33.2 g/L, GGT 883 U/L, PA 136 mg/L, Glu 12.57 mmol/L, LACT 2.3 mmol/L, ESR 78 mm/h, PT normal and d-dimer positive.
By sputum smear, a small amount of negative bacillus; no fungal spore and no acid-fast bacillus.
Sputum culture found Acinetobacter baunannii/calcoaceticus complex.
By blood gas analysis, pH 7.567, PaCO2 45.5 mmHg, PaO2 74 mmHg, BE 19 mmol/L, \( {\text{HCO}}_{3}^{-}\)41.4 mmol/L and SpO2 96 %.
Sputum culture on Nov. 19th, 2009 found a small amount of Gram negative bacillus.
Sputum smear found a small amount of positive coccus, negative coccus; a great amount of negative bacillus, fungal spore. d-dimer weak positive. LACT 2.6 mmol/L, leukocytes count 15.5 × 109/L, neutrophils 88.8 %, platelets count 164 × 109/L, hemoglobin 109 g/L. ALB 34.4 g/L, PA 158 mg/L, CRP 87.6 mg/L, Glu 10.46 mmol/L, HBDH 225 U/L, LDH 357 U/L.
By blood gas analysis, pH 7.43, PaCO2 64 mmHg, PaO2 67 mmHg, BE 14.9 mmol/L, \( {\text{HCO}}_{3}^{-}\)41.4 mmol/L, FiO2 60 %. Na+ 144 mmol/L, K+ 3.5 mmol/L. Discharge of 200 mL dark red bloody pleural fluid.
Sputum smear found negative coccus and bacillus; a great amount of fungal spore.
Diagnostic Imaging
By chest X-ray on Nov. 13th, 2009 (Fig. 11.87a), diffusive shadows with increased density in the right lung field and the left lower lung field; upper border of the right diaphragm blurry.
By chest X-ray on Nov. 14th, 2009 (Fig. 11.87b), diffusive shadows with increased density in the right lung field and in the left lower lung field; increased transparency of the right lung and obviously improved conditions compared to chest X-ray findings on Nov. 13th, 2009.
By chest X-ray on Nov. 15th, 2009 (Fig. 11.87c), diffusive shadows with increased density in the left middle-lower lung field; increased transparency of the right lung with obviously improved conditions and progressive conditions of the left lung compared to chest X-ray findings on Nov. 13th, 2009.
By chest X-ray on Nov. 16th, 2009 (Fig. 11.87d), diffusive shadows with increased density in both lower lungs fields; increased transparency of the right lung and obviously improved conditions of the right lung compared to chest X-ray findings on Nov. 15th, 2009.
By chest X-ray on Nov. 17th, 2009 (Fig. 11.87e), diffusive shadows with increased density in the right lung; improved conditions of the left lung and progressive conditions of the right lung compared to chest X-ray findings on Nov. 16th, 2009.
By chest X-ray on Nov. 18th, 2009 (Fig. 11.87f), diffusive shadows with increased density in the right lung; obviously improved conditions of the left lung and progressive conditions of both lower lungs compared to chest X-ray findings on Nov. 17th, 2009.
By chest X-ray on Nov. 19th, 2009 (Fig. 11.87g), diffusive shadows with increased density in the right lung field; the right lung compressed by 80 %; obviously improved conditions of the left lung and progressive conditions of both lower lungs compared to chest X-ray findings on Nov. 17th, 2009.
By chest CT scanning on Nov. 19th, 2009 (Fig. 11.87h–k), no transparency area of lung markings in the right lung; visible gas–fluid level; hydropneumothorax in the right lung; compressed and gathering pulmonary tissues of the right lung; mediastinum rightward migration; a small amount of effusion in the left chest cavity. By pleural effusion test, purulent effusion of the chest cavity.
Diagnosis. Pneumonia complicating Influenza A (H1N1).



Fig. 11.87
Case 11.88
History of Present Illness. A 19-years-old woman, complained of fever, with the highest body temperature of 39.6 °C. She also had sore throat and coughs occasionally with whitish foamy phlegm.
Past History. None.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 37.4 °C. Heart rate 94 beats/min. Breathing rate 22 times/min. Blood pressure 120/70 mmHg. Pharyngeal congestion. The right tonsil swollen to II degree and the left tonsil swollen to I degree, with no purulent secretions.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
By routine blood tests on Nov. 16th, 2009, leukocytes count 5.0 × 109/L, neutrophils 58.3 %, lymphocytes 33.5 %, erythrocytes count 5.3 × 1012/L, hemoglobin 161 g/L, platelets count 187 × 109/L.
By blood biochemistry, CRP 19 mg/L, HBDH 185 U/L.
Diagnostic Imaging
By chest CT scanning on Nov. 13th, 2009 (Fig. 11.88a–d), ground glass liked shadows in the dorsal segment of the right lower lung and in the posterior basal segment of the right lower lung; lobular central nodular/patchy shadows with air cavities.
By chest CT scanning on Nov. 16th, 2009 (Fig. 11.88e–h), ground glass liked/patchy shadows in the dorsal segment and the posterior basal segment of the right lower lung; obviously absorbed foci and improved conditions compared to chest CT scanning on Nov. 13th, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.88
Case 11.89
History of Present Illness. A 59-years-old woman, complained of fever, chest pain, cough and expectoration of whitish foamy phlegm, general soreness, headache and fatigue. Her highest body temperature was 39.8 °C, with sore throat, tightness of breath, expectoration of yellowish thick phlegm, palpitation, shortness of breath and bloody yellowish phlegm.
Past History. History of hypertension for 26 years.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Respiration sounds low. Fine moist wheezing in both lower lungs and diffusive dry wheezing in both lower lungs. The heart oversized relative to the dullness area. Heart rate 78 beats/min. Heart rhythm regular. Diagnosis on admission: (1) Influenza A (H1N1) and critical pneumonia of both lungs; hypoxemia; Type I respiratory failure. (2) Acute episode of chronic bronchitis; emphysema; chronic obstructive pulmonary disease.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
By blood gas analysis on Nov. 8th, 2009, pH 7.467, PaCO2 32.2 mmHg, PaO2 57 mmHg, \( {\text{HCO}}_{3}^{-}\) 22.5 mmol/L, SaO2 96 %.
Diagnostic Imaging
By chest CT scanning on Nov. 8th, 2009 (Fig. 11.89a–d), patchy shadows with increased density in both lower lungs.
By chest CT scanning on Nov. 9th, 2009 (Fig. 11.89e–h), patchy shadows with increased density in both lower lungs; no obvious changes compared to chest CT scanning on Nov. 8th, 2009.
By chest CT scanning on Nov. 11th, 2009 (Fig. 11.89i–l), patchy shadows with increased density in both lower lungs; obviously improved conditions compared to chest CT scanning on Nov. 9th, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).



Fig. 11.89
Case 11.90
History of Present Illness. A 31-years-old man, complained of cough, expectoration and throat soreness for 10 days; fever and tightness of breath for 4 days. The patient suffered from a cold and cough 10 days ago, with a little whitish foamy phlegm and throat soreness. Four days before hospitalization, he suffered from fever and chills, with the highest body temperature of 39 °C and bloody phlegm. He reported tightness of breath, tidal fever, spontaneous sweating and chills when coughing and talking.
Past History. HBV carrier, with normal liver function.
Contact History. Denied history of contacting with Influenza A (H1N1) patients.
Signs. Pharyngeal congestion. The right tonsil swollen to I degree and the left tonsil not swollen. Respiration sounds in both lungs lowered. Moderate and fine moist wheezing in both lungs, especially in the right lung.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
On Nov. 18th, 2009, by blood gas analysis, pH 7.54, PaCO2 30.2 mmHg, PaO2 51 mmHg, BE −3.0 mmol/L, \( {\text{HCO}}_{3}^{-}\)26.0 mmol, indicating type I respiratory failure.
By routine blood tests, leukocytes count 8.4 × 109/L, neutrophils 89.8 %, hemoglobin 174 g/L.
By blood biochemistry, ALT 86 U/L, AST 55 U/L, PA 72 mg/L, CRP 121.4 mg/L, CK 133 U/L, CK-MB 22 U/L, HBDH 282 U/L, LDH 387 U/L, blood lactate 3.7 mmol/L. ESR 58 mm/h.
On Nov. 21st, 2009, by blood biochemistry, ALT 133 U/L, AST 88 U/L, TP 58.4 g/L, ALB 28.7 g/L, Glu 29.7 g/L, PA 135 mg/L, Na+ 130.8 mmol/L, K+ 4.47 mmol/L; LACT 3.0 mmol/L.
By routine blood tests, leukocytes count 4.8 × 109/L, lymphocytes count 7.9 %, neutrophils 89.5 %.
By blood gas analysis, pH 7.36, PaCO2 60 mmHg, PaO2 51 mmHg, BE 5.2 mmol/L, \( {\text{HCO}}_{3}^{-}\) 32.8 mmol, SaO2 86 %, Na+ 138 mmol/L, K+ 4.0 mmol/L.
On Nov. 23rd, 2009, sputum smear twice found a great amount of positive coccus, a small amount of negative coccus and negative bacillus, with fungal spores.
By routine blood tests, leukocytes count 12.6 × 109/L, neutrophils 94.4 %, increased compared to the previous tests findings.
By blood biochemistry, ALT 291 U/L, AST 136 U/L, CRP 5.6, LACT 5.0 mmol/L.
Electrolytes: Na+ 132.9 mmol/L, K+ 4.64 mmol/L; HBDH 243 U/L, LDH 315 U/L. Increased myocardial enzyme of the liver function compared to the previous tests findings.
Diagnostic Imaging
Chest CT scanning on Nov. 18th, 2009 (Fig. 11.90a–f), patchy cloudy shadows with increased density and ground glass liked shadows in both lungs, especially in posterior basal segments of both lower lungs, with gas bronchogram.
Chest CT scanning on Nov. 21st, 2009 (Fig. 11.90g–k), patchy cloudy shadows with increased density in both lungs, especially in posterior basal segments of both lower lungs; obviously progressive conditions compared to chest CT scanning on Nov. 18th, 2009.
Chest CT scanning on Nov. 23rd, 2009 (Fig. 11.90l–r), patchy cloudy shadows with increased density in both lungs, especially in posterior basal segments of both lower lungs, with gas bronchogram; slightly absorbed foci and improved conditions compared to chest CT scanning on Nov. 21st, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).



Fig. 11.90
Case 11.91
History of Present Illness. A 28-years-old man, complained of fever and cough for 1 day, with expectoration of yellowish thick phlegm, chills, shivers, rhinorrhea and nasal obstruction.
Past History. Histories of hepatitis A and tuberculosis 10 years ago.
Contact History. Self reported history of contacting with patients suffering from flu liked symptoms within a week.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
On Nov. 18th, 2009, blood gas analysis found pH 7.437, PaCO2 31.4 mmHg, PaO2 68 mmHg, EB-3 mmol/L, \( {\text{HCO}}_{3}^{-}\) 21.2 mmol/L. Routine blood tests found leukocytes count 6.46 × 109/L, neutrophils 90.3 %, platelets count 111 × 109/L, hemoglobin 143 g/L.
On Nov. 19th, 2009, blood biochemistry found PA 175 mg/L; CRP 119.4 mg/L; LACT 2.2 mmol/L; PT 15.6 s. Routine blood tests found leukocytes count 7.8 × 109/L, neutrophils 86.7 % and lymphocytes 9.8 %.
Diagnostic Imaging
By chest CT scanning on Nov. 18th, 2009 (Fig. 11.91a–d), flaky or ground glass liked shadows in the posterior basal segment of the left low lung.
By chest CT scanning on Nov. 21st, 2009 (Fig. 11.91e–h), flaky or ground glass liked shadows in the posterior basal segment of the left lower lung; no obvious changes compared to chest CT scanning on Nov. 18th, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.91
Case 11.92
History of Present Illness. A 40-years-old man, complained of fever and cough for 3 days; dyspnea for 1 day. He also suffered from expectoration. After anti-inflammatory medications by himself, conditions were not improved, with chest distress and dyspnea.
Past History. History of diabetes.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39 °C.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
On Nov. 13th, 2009, blood gas analysis found pH 7.324, PaCO2 52.5 mmHg, PaO2 34.1 mmHg. Routine blood tests found leukocytes count 5.53 × 109/L, neutrophils 84.6 % and lymphocytes 8.7 %. The liver functions: ALT 33 U/L, AST 43 U/L, Cr 51.3 U/L, Glu. 19.83 mmol/L.
On Nov. 18th, 2009, blood gas analysis found pH 7.26, PaCO2 49 mmHg, PaO2 216 mmHg. Routine blood tests found leukocytes count 8.32 × 109/L, neutrophils 87.3 %, lymphocytes 9.6 %. The liver functions: ALT 62.2 U/L, AST 79.5 U/L, UREA 22.96 U/L, Cr 172.5 U/L.
On Nov. 22nd, 2009, blood gas analysis found pH 7.24, PaCO2 40 mmHg, PaO2 108 mmHg. Routine blood tests found leukocytes count 11.38 × 109/L, neutrophils 89.7 %, and lymphocytes 7.2 %. The liver functions: ALT 62.2 U/L, AST 79.5 U/L, UREA 22.96 U/L, Cr 172.5 U/L.
On Nov. 26th, 2009, blood gas analysis found pH 7.21, PaCO2 37 mmHg, PaO2 152 mmHg. Routine blood tests found leukocytes count 7.73 × 109/L, neutrophils 89.4 %, lymphocytes 9.1 %, erythrocytes count 1.9 × 1012/L, hemoglobin 60 g/L. The liver functions: ALT 29 U/L, AST 35 U/L, UREA 17.63 U/L, Cr 134 U/L.
On Nov. 28th, 2009, blood gas analysis found pH 7.24, PaCO2 40 mmHg, PaO2 108 mmHg. Routine blood tests found leukocytes count 7.67 × 109/L, neutrophils 81.7 %, lymphocytes 13.4 %, erythrocytes count 2.13 × 1012/L, hemoglobin 67 g/L. The liver functions: ALT 62.3 U/L, AST 145 U/L, UREA 12.09 U/L, Cr 132.8 U/L.
Diagnostic Imaging
By chest X-ray on Nov. 25th, 2009 (Fig. 11.92a), decreased transparency of the right lung and the left middle-lower lung; intrapulmonary large flaky shadows with increased density; enlarged and blurry hilum.
By chest X-ray on Nov. 26th, 2009 (Fig. 11.92b), decreased transparency of the right lung and the left middle-lower lung; intrapulmonary large flaky shadows with increased density; enlarged and blurry hilum; progressive conditions compared to the chest X-ray findings on Nov. 25th, 2009.
By chest X-ray on Nov. 28th, 2009 (Fig. 11.92c), decreased transparency of the right lung and the left middle-lower lung; intrapulmonary large flaky shadows with increased density; enlarged and blurry hilum; progressive conditions compared to the chest X-ray findings on Nov. 26th, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.92
Case 11.93
History of Present Illness. A 45-years-old woman, suffered from chills and fever 5 days ago. She also had eyes upset, dry cough, a little phlegm, chest distress and suffocation. He had been diagnosed as having bronchitis in another hospital. After anti-inflammatory therapy, she had chest distress and shortness of breath. Finally, she was transferred to You’an Hospital in Beijing.
Past History. None related to the present illness.
Contact History. Self reported history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39.5 °C. Pharyngeal congestion.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) negative.
On Nov. 13th, 2009, blood gas analysis found pH 7.466, PaCO2 35.5 mmHg, PaO2 76.0 mmHg. Routine blood tests found leukocytes count 2.84 × 109/L, neutrophils 83.8 % and lymphocytes 12 %.
On Nov. 14th, 2009, blood gas analysis found pH 7.471, PaCO2 31.8 mmHg, PaO2 43.6 mmHg. Routine blood tests found leukocytes count 3.39 × 109/L, neutrophils 81.1 % and lymphocytes 14.5 %. The liver functions: ALT 21.1 U/L, AST 51.3 U/L, UREA 3.34 U/L, Cr 41.0 U/L.
On Nov. 15th, 2009, blood gas analysis found pH 7.438, PaCO2 36.5 mmHg, PaO2 69.3 mmHg. Routine blood tests found leukocytes count 2.18 × 109/L, neutrophils 84 %, lymphocytes 12.8 %.
On Nov. 18th, 2009, blood gas analysis found pH 7.488, PaCO2 33.2 mmHg, PaO2 46.9 mmHg. Routine blood tests found leukocytes count 3.69 × 109/L, neutrophils 67.7 %, lymphocytes 24.7 %. The liver functions: ALT 62.9 U/L, AST 144.4 U/L, Cr 46.3 U/L, Glu 7.45 mmol/L.
On Nov. 20th, 2009, blood gas analysis found pH 7.460, PaCO2 34 mmHg, PaO2 79 mmHg.
On Nov. 30th, 2009, blood gas analysis found pH 7.310, PaCO2 58 mmHg, PaO2 78 mmHg. Routine blood tests found leukocytes count 11.25 × 109/L, neutrophils 83.5 %, lymphocytes 11.8 %, erythrocytes count 3.25 × 1012/L, hemoglobin 102 g/L. The liver functions: ALT 44 U/L, AST 149 U/L, UREA 4.83 U/L, Cr 33.5 U/L.
Diagnostic Imaging
By chest X-ray on Nov. 25th, 2009 (Fig. 11.93a), diffusive shadows with increased density in the right lower lung and the left middle lower lung; hilum enlarged and blurry; the upper bound of diaphragm covered.
By chest X-ray on Nov. 26th, 2009 (Fig. 11.93b), diffusive shadows with increased density in both lungs; hilum enlarged and blurry; the upper bound of diaphragm covered; obviously progressive conditions compared to chest X-ray findings on Nov. 25th, 2009.
By chest X-ray on Nov. 27th, 2009 (Fig. 11.93c), diffusive shadows with increased density in both lungs; hilum enlarged and blurry; the upper bound of diaphragm covered; no obvious changes compared to chest X-ray findings on Nov. 26th, 2009.
By chest X-ray on Nov. 30th, 2009 (Fig. 11.93d), diffusive shadows with increased density in both lungs; hilum enlarged and blurry; the upper bound of diaphragm covered; obviously progressive conditions compared to chest X-ray findings on Nov. 27th, 2009.
By chest X-ray on Dec. 2nd, 2009 (Fig. 11.93e), diffusive shadows with increased density in both lungs; hilum enlarged and blurry; the upper bound of diaphragm covered; slightly improved conditions compared to chest X-ray findings on Nov. 30th, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.93
Case 11.94
History of Present Illness. A 24-years-old man, complained of fever and cough for 5 days. After therapies of azithromycin in another hospital and You’an Hospital in Beijing, his conditions were not improved, with recurrent fever and deteriorated cough. On the fifth day after disease onset, he was hospitalized due to positive throat swabs.
Past History. None related to the present illness.
Contact History. Not definitive history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 39.6 °C. Conscious but poor spirituality. Pharyngeal congestion. Tonsils not swollen. The respiration sound of the left lungs low, with no dry and moist rale.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
On Dec. 1st, 2009, blood biochemistry found TP 65 g/L, A 38 g/L, AST 28 U/L, ALT 28 U/L, LDH 345 U/L; CK 135 U/L, renal function and electrolytes normal. HBV-M found HBsAB (+) and the others negative; HCVAb (−), HAVIgM (−), HIVAb (−), HIVIgM (−), syphilis (−). The coagulation tests found APTT 37 s, TT 18 s, Fib 5.07 g/L.
ECG. Sinus rhythm.
Diagnostic Imaging
By chest CT scanning on Nov. 30th, 2009 (Fig. 11.94a–f), scattered patchy blurry shadows in posterior segments of both lower lungs.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.94
Case 11.95
History of Present Illness. A 22-years-old man, complained of fever and cough for 6 days, with expectoration of a little whitish sputum, nasal obstruction and runny nose. He received therapies for cold in another hospital, with poor outcomes. He was hospitalized on the third after disease onset due to positive throat swabs.
Past History. History of intelligence disturbance.
Contact History. Self reported none definitive history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 38.6 °C. Pharyngeal congestion. Tonsils swollen to I degree. Shortness of breath. The respiration sound of both lungs coarse. Large amount of dry and moist rales in both lungs.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
On Dec. 1st, 2009, routine blood tests found leukocytes count 3.64 × 109/L, neutrophils 60.1 %, lymphocytes 25.3 %.
On Dec. 1st, 2009, TP 68 g/L, A 31 g/L, AST 60 U/L, ALT 60 U/L, LDH 621 U/L, CK 141 U/L. HBV-M found all indices negative.
ECG. Normal.
Diagnostic Imaging
By chest CT scanning on Nov. 27th, 2009 (Fig. 11.95a–e), scattered cloud flockiest blurry dense shadows in both lungs; air bronchogram, especially in the dorsal and basal segments of both lungs with blurry boundaries.
By chest CT scanning on Dec. 3rd, 2009 (Fig. 11.95f–j), scattered cloud blurry dense shadows or ground glass liked dense shadows in both lungs; air bronchogram, especially in the dorsal and basal segments of both lungs; no obvious changes compared to chest CT scanning on Nov. 27th, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.95
Case 11.96
History of Present Illness. A 41-years-old man, complained of fever and cough for 4 days. He had fever 4 days ago, with a body temperature of 40 °C, with cough, no phlegm, sore extremities and fatigue. Therapies of ephalosporins and penicillin infusion showed no favorable outcomes in the local countryside clinic. Then he received oseltamivir therapy 1 day ago in the local hospital, with outcomes of chest tightness and the shortness of breath after activities. The patients was then transferred into the clinic of You’an Hospital in Beijing. On the fourth day after disease onset, he was hospitalized due to positive throat swabs.
Past History. The right collar bone fracture 10 years ago. No histories of other illnesses.
Contact History. Self reported none definitive history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 36.9 °C. Heart rate 92 beats/min. Respiration 23 times/min. Conscious but poor spirituality. No lips cyanosis. Tonsils not swollen. Respiration sound of the left middle lung low, with no dry and moist rales. Heart sound powerful with regular rhythm. No murmurs in the heart valvar areas.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
On Nov. 28th, 2009, routine blood tests found leukocytes count 4.1 × 109/L, lymphocytes 46.10 % and neutrophils 38.30 %.
On Nov. 28th, 2009, HBV-M found HBsAb (+), and the other indices negative; HCVAb (−); syphilis (−).
On Nov. 29th, 2009, blood gas analysis found pH 7.379, PaO2 103 mmHg, PaCO2 39.8 mmHg, SaO2 98 %, \( {\text{HCO}}_{3}^{-}\) 23.5 mmol/L, BE −2 mmol/L.
On Dec. 1st, 2009, subtypes of T-lymphocytes were CD4+ 816 × 106/L, CD8+ 516 × 106/L, CD4+/CD8+ 1.58.
Diagnostic Imaging
By chest CT scanning on Dec. 1st, 2009 (Fig. 11.96a–d), extensive cloudy flocculent shadows in both lungs; poor transparency of both lungs, especially the left lung; unsmooth bilateral pleura.
By chest CT scanning on Dec. 1st, 2009 (Fig. 11.96e–h), intrapulmonary patchy shadows with slightly increased density; blurry boundaries; uneven densities within shadows; obviously improved conditions compared to chest CT scanning on Nov. 28th, 2009.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.96
Case 11.97
History of Present Illness. A 42-years-old man, complained of fever and cough for 8 days; chest distress for 5 days. He had fever 8 days ago, with the highest body temperature of 39.5 °C. He also had cough, with whitish sputum but no chills and convulsion. Therapies (details unknown) were given in the local hospital, but with no favorable outcomes. And the patient suffered from chest distress 5 days ago, deteriorating after activities. He was admitted on the seventh day after the disease onset into You’an Hospital in Beijing due to positive throat swabs.
Past History. None related to the present illness.
Contact History. No definitive history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 37.8 °C. Heart rate 86 beats/min. Breathing rate 32 times/min. Conscious but poor spirituality. Lips cyanosis. Pharyngeal congestion. Tonsils swollen to I degree. The respiration sound of both lungs coarse, with moist rales.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
On Dec. 2nd, 2009, blood gas analysis found pH 7.45, PaO2 68 mmHg, PaCO2 46 mmHg, \( {\text{HCO}}_{3}^{-}\) 31.5 mmol/L and BE 7.3 nmol/L.
On Dec. 2nd, 2009, blood biochemistry found LFT 24 g/L, A 24 g/L, ALT 42 U/K, AST 110 U/K, CK 154 U/K, CK-MB 7.38 U/K, LDH 988 U/K, CHE 4,394 U/K.
On Dec. 2nd, 2009, routine blood tests found leukocytes count 3.73 × 109/L, lymphocytes 85.5 %, neutrophils 13.42 %. HBV-M found HBsAb (−), HBcAb (−), HCVAb (−), HIVAb (−), HIVIgM (−), syphilis (−).
On Dec. 3rd, 2009, blood gas analysis found pH 7.49, PaO2 56 mmHg, PaCO2 43 mmHg, SaO2 94.9 %, \( {\text{HCO}}_{3}^{-}\) 23.2 mmol/L, BE 3.8 nmol/L.
On Dec. 4th, 2009, blood gas analysis found pH 7.51, PaO2 66 mmHg, PaCO2 29 mmHg, SaO2 98.3 %, \( {\text{HCO}}_{3}^{-}\) 28.7 mmol/L, BE 0.2 nmol/L.
Sputum culture for 48 h found no pathogens.
Diagnostic Imaging
By chest X-ray on Dec. 1st, 2009 (Fig. 11.97a), cloud mist liked shadows with increased density in both lungs, especially in the right lung; enlarged and thickened hilum.
By chest X-ray on Dec. 1st, 2009 (Fig. 11.97b–f), large flaky shadows with increased density in both lungs; parenchymal shadows in some pulmonary tissues, especially in the dorsal and the posterior basal segments.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.97
Case 11.98
History of Present Illness. A 58-years-old man, complained of fever and cough for 3 days, with a little yellowish and whitish phlegm. He was admitted to You’an Hospital in Beijing due to positive throat swabs.
Past History. History of hypertension for 3 years
Contact History. No definitive history of contacting with Influenza A (H1N1) patients.
Signs. The highest body temperature 39 °C. Pharyngeal congestion obvious. Tonsils not swollen. Respiration sound of both lungs coarse, with obvious moist rales in both lungs.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
On Nov. 20th, 2009, routine blood tests, leukocytes count 3.4 × 109/L, neutrophils 43.9 %, lymphocytes 16.1 %.
On Nov. 20th, 2009, routine blood tests, leukocytes count 3.39 × 109/L, neutrophils 81.4 %, lymphocytes 41.52 %.
On Nov. 24th, 2009 blood biochemistry found AST 36 U/L, renal function normal, electrolytes normal, LDH 252 U/L, CK 213 U/L and AK 5.45 U/L. HBV-M negative.
ECG. Normal.
Diagnostic Imaging
By chest CT scanning on Nov. 21st, 2009 (Fig. 11.98a–c), scattered patchy blurry shadows of both lungs, with blurry boundaries.
Diagnosis. Pneumonia complicating Influenza A (H1N1).

Fig. 11.98
Case 11.99
History of Present Illness. A 36-years-old man, complained of fever and cough for 6 days. He started to have fever 6 days ago, with a body temperature of 39.7 °C, with cough, bloody phlegm, no chills, convulsion, sore throat, nasal obstruction, rhinorrhea, chest pain and diarrhea. Cefodizime, azithromycin and andrographolide were administered in the local hospital, but with no favorable outcomes. He still suffered from out of breath and limited activities. Therapies of gatifloxacin, vidarabine, aminophylline intravenous drip were given in the First Affiliated Hospital of Zhengzhou University, but with occurrence of dyspnea, decreased SaO2. Noninvasive mechanical ventilation was then ordered. On the sixth day after illness onset, he was transferred to You’an Hospital in Beijing by an ambulance due to positive throat swabs. Finally, death occurred, followed by autopsy.
Past History. None related to the present illness.
Contact History. No definitive history of contacting with Influenza A (H1N1) patients.
Signs. Body temperature 36.5 °C. Heart rate 120 beats/min. Breathing rate 35 times/min. The blood pressure 120/85 mmHg. Conscious but poor spirituality. Orthopnoea. Pharyngeal congestion. Tonsils not swollen. Shortness of breath. Vocal fremitus weakened in the right middle-lower lung and in the left lower lung. Respiration sound coarse in the left upper middle lung and in the right upper lung. Respiration sound weakened in the left lower lung. No respiration sound in the right middle lower lung.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) negative, specific gene of Influenza A (H1N1) virus (gene HA) positive.
On Nov. 21st, 2009, the sputum smear found no fungus.
On Nov. 21st, 2009, routine blood tests found leukocytes count 5.41 × 109/L, neutrophils 87.84 %, lymphocytes 8.14 %, erythrocytes count 3.94 × 1012/L, hemoglobin 112 g/L, platelets count 213 × 109/L.
On Dec. 2nd, 2009, blood biochemistry of the liver function found ALT 20 U/L, AST 48 U/L; of renal function found BUN 2.7 mmol/L, Cr 57 μmol/L, UA 135 μmol/L; of electrolytes found K+ 3.48 mmol/L, Ca2+ 2.02 mmol/L, Na+ 131 mmol/L; Glu 8.2 mmol/L, CK-MB 3.0 U/L, LDH 505 U/L.
On Nov. 21st, 2009, blood gas analysis found pH 7.38, PaO2 23 mmHg, PaCO2 49.8 mmHg, \( {\text{HCO}}_{3}^{-}\) 29.6 mmol/L. HBV-M found all indices negative, HCVAb (−), HAVIgM (−), HIVAb (−), syphilis (−).
On Nov. 23rd, 2009, sputum culture for three times found no pathogenic bacteria growth.
On Nov. 25th, 2009, ESR 60 mm/h.
On Nov. 24th, 2009, blood MycoDotTM (include TB-CHEK, TB-IgG and TB-Dot): negative.
On Nov. 25th, 2009, the sputum smear found no acid-fast bacillus.
On Nov. 25th, 2009, routine blood tests found leukocytes count 17.4 × 109/L, neutrophils 95.84 %, lymphocytes 3.61 %, erythrocytes count 3.35 × 1012/L, hemoglobin 94 g/L, platelets count 265 × 109/L.
On Nov. 25th, 2009, blood biochemistry of the liver function found ALT 16 U/L, AST 28 U/L; of the renal function found BUN 2.3 mmol/L, Cr 54 μmol/L, UA 79 μmol/L; of electrolytes found K+ 3.41 mmol/L, Ca2+ 1.95 mmol/L, Na+ 137 mmol/L; Glu 6.34 mmol/L, CK 42 U/L, CK-MB 4.0 U/L, LDH 476 U/L. Blood gas analysis found pH 7.526, PaO2 41 mmHg, PaCO2 29.1 mmHg, \( {\text{HCO}}_{3}^{-}\) 24.1 mmol/L.
Diagnostic Imaging
By chest CT scanning on Nov. 20th, 2009 (Fig. 11.99a–d), large flaky shadows with increased density in both middle lower lungs.
By diagnostic imaging on Nov. 20th, 2009 (Fig. 11.99e–h), parenchymal changes of some pulmonary tissues; gas bronchogram; parenchymal changes and gas bronchogram especially in the dorsal and the posterior basal segments of both lungs.
By chest X-ray on Nov. 20th, 2009 (Fig. 11.99i), diffusive shadows with increased density in the both middle lower lungs, more obvious in the left lung than in the right lung.
By pathological analysis (Fig. 11.99j–l), H&E staining showed widened pulmonary interstitial; alveolar cellulose exudates; pulmonary interstitial fibrosis; infiltration of lymphocytes, mononuclear cells and neutrophils.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.99
Case 11.100
History of Present Illness. A 70-years-old man, complained of recurrent fever and cough for more than 10 years. He self reported mental tiredness and swollen legs for 4 years, poor appetite for 9 days and fever for 3 days. At 17:00 on Sep. 12th, 2009, he was admitted with clinical diagnosis of severe Influenza A (H1N1) and pneumonia of both lungs; type II respiratory failure; acute episode of chronic bronchitis; obstructive pulmonary emphysema; heart originated heart diseases; heart failure; heart function of grade III to IV; bronchiectasis; type II diabetes and diabetic peripheral neuropathy; diabetic nephropathy; cataracts; respiratory acidosis and metabolic alkalosis.
Past History. Histories of chronic obstructive pulmonary disease and diabetes.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) negative, specific gene of Influenza A (H1N1) virus (gene HA) positive.
By routine blood tests, leukocytes count 10.9 × 109/L, neutrophils 85.0 %, platelets count 113 × 109/L. Blood gas analysis found pH 7.4, PaO2 92 mmHg, PaCO2 59 mmHg, BE 9 nmol/L, CRP 171.4 mg/L, BUN 11.0 mmol/L, Cr normal, liver functions normal, myocardial enzyme normal, blood coagulation time within normal limits.
Diagnostic Imaging
By chest X-ray on Sep. 12th, 2009 (Fig. 11.100a, b), flaky blurry shadows with increased density in the both lower lungs; enlarged and blurry hilum.
By chest CT scanning on Sep. 12th, 2009 (Fig. 11.100c–h), infectious foci in the left lung, anterior segment of the right upper lung, posterior basal segment of the right lower lung, lateral basal segment of the right lung; slight bronchiectasis in the lower lobes of both lungs; bronchitis emphysema of both lungs; aortic diameter about 4.0 cm; the trunk diameter of pulmonary artery about 3.3 cm.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.100
Case 11.101
History of Present Illness. A 75-years-old woman, complained of fever, expectoration and fever for 4 days. After a history of contacting with a Influenza A (H1N1) patient, she started to have fever 4 days before admission, with the highest body temperature of 39 °C. She also had serious cough with yellowish phlegm but with difficulty expectorating, headache, sore throat, tightness of breath, self reported mental tiredness, poor appetite. After self administration of medicines for the cold, her body temperature decreased, but recurrent without to the normal level.
Past History. History of hypertension.
Contact History. Self reported history of contacting with a Influenza A (H1N1) patient.
Signs. Body temperature 37.4 °C. Heart rate 100 beats/min. Breathing rate 26 times/min. Blood pressure 110/70 mmHg, SpO2 94 %. Jugular vein obvious distention. Hepatojugular reflux positive. Vocal fremitus of both lungs weakened. Hyper resonance on percussion. Downward migration of the lower bound of lung. Shortness of breath. Respiration sound of both lungs low. Moderate to fine moist rales in both middle lower lungs, especially in the left lung; rare to moderate low dry rales of double phase in both lungs. Relative dullness of the heart. Heart bound extended leftward. Heart rate 100 beats/min. Heart rhythm regular. Heart sounds of S1 and S2 normal, with A2 > P2. Mild pitting edema under the knees of legs.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) negative, specific gene of Influenza A (H1N1) virus (gene HA) negative.
By routine blood tests, leukocytes count 10.0 × 109/L, neutrophils 73.0 %, platelets count 113 × 109/L. Blood gas analysis found pH 7. 4, PaO2 92 mmHg, PaCO2 59 mmHg, BE 9 mmol/L. By blood biochemistry, CRP 171.4 mg/L, BUN 11.0 mmol/L.
By reexamination of blood gas analysis, pH 7.35, PaO2 108 mmHg, PaCO2 43 mmHg, \( {\text{HCO}}_{3}^{-}\) 27 mmol/L.
ECG. T wave low and flat.
Diagnostic Imaging
By chest CT scanning on Nov. 16th, 2009 (Fig. 11.101a–f), increased lung markings of both lower lungs; spotty and flaky blurry shadows, especially posterior segment of the lower lung.
Diagnosis. Pneumonia complicating Influenza A (H1N1).


Fig. 11.101
Case 11.102
History of Present Illness. A 74-years-old man, complained of fever an cough for 4 days.
Past History. History of hypertension for 8 years, with the highest blood pressure of 200/100 mmHg and a usual blood pressure of 180/90 mmHg. Oral intake of Bezoar antihypertensive pill maintained the blood pressure normal. In addition, a history of type II diabetes for 2 years, with oral intake of metformin but no monitoring of blood glucose. Also having history of chronic bronchitis for more than 10 years. Death occurred with autopsy.
Contact History. None.
Signs. Body temperature 39.4 °C. Confused in deep coma. No response to verbal commands. Heart rate 120 beats/min and the pulses regular. Breathing rate 24 times/min. Respiration assisted with tracheal cannulation and a respirator. The respiration sound of both lungs low. Rare moist rales in the bottoms of both lungs. Abdomen (−). Both lower extremities not swollen.
Laboratory Tests
By throat swabs, nucleic acid of Influenza A (H1N1) virus positive.
On Dec. 3rd, 2009, routine blood tests found leukocytes count 9.51 × 109/L, neutrophils 80.6 %, Hb 102 g/L, platelets count 154 × 109/L. Blood gas analysis found pH 7.3, PaO2 144 mmHg, PaCO2 70 mmHg, \( {\text{HCO}}_{3}^{-}\) 33.4 mmol/L, BE 5.4 mmol/L, SaO2 98.8 %. The Liver functions test found ALT 46.6 U/L, AST 56.3 U/L, TBLT 6.9 μmol/L, Cr 85.6 μmol/L, K+ 4.14 mmol/L, Na+ 150.5 mmol/L.
On Dec. 3rd, 2009, routine blood tests found leukocytes count 10.83 × 109/L, GR 79.8 %, Hb 105 g/L, PLT 140 × 109/L. Blood gas analysis found pH 7.31, PaO2 93 mmHg, PaCO2 71 mmHg, \( {\text{HCO}}_{3}^{-}\) 34.7 mmol/L, BE 7 mmol/L, SaO2 96 %. The liver function tests found ALT 46.2 U/L, AST 46.1 U/L, TBLT 6.9 μmol/L, Cr 112 μmol/L, K+ 3.45 mmol/L, Na+ 154 mmol/L.
Diagnostic Imaging
By chest X-ray (Fig. 11.102a, b), cloud mist liked blurry shadows with increased density in the both upper lungs and in the both lower lungs; enlarged and blurry hilum.
Pathological Analysis
Figure 11.102c–j demonstrated widened pulmonary interstitial, interalveolar fibrosis, inflammatory cells infiltration (mainly neutrophils), exudation of mononuclear cells, lymphocytes and macrophages by H&E staining.
Figure 11.102k, l demonstrated myocardial interstitial edema and minor blood vessels dilatation by H&E staining.



Fig. 11.102
Case 11.103
History of Present Illness. A 55-years-old woman, complained of cough for 7 days, fever for 6 days, with the highest temperature of 40 °C. She had no chills, but sore throat, shortness of breath, headache, spasmodic breathing, pink foamy phlegm. Death occurred with following autopsy
Past History. None.
Contact History. Denied history of contacting with any Influenza A (H1N1) patient.
Signs. Pharyngeal congestion. Tonsils not swollen. Moist rales in both lungs.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
On Nov. 19th, 2009, the liver functions tests found ALT 81.3 U/L, AST 166.6 U/L.
On Nov. 23rd, 2009, the liver functions tests found ALT 63.1 U/L, AST 55.1 U/L, Cr 137.5 μmol/L, UREA 9.67 mmol/L.
On Nov. 24th, 2009, the liver functions tests found ALT 40 U/L, AST 32 U/L, Cr 115.9 μmol/L, UREA 16.73 mmol/L. Blood gas analysis found pH 7.33, PaCO2 54 mmHg, PaO2 85 mmHg. Routine blood tests found leukocytes count 17.89 × 109/L, lymphocytes 5.5 %, neutrophils 90.7 %.
On Oct. 28th, 2009, routine blood tests found leukocytes count 7.8 × 109/L, neutrophils 88.4 %, lymphocytes 8.2 %. Blood gas analysis found pH 7.512, PaO2 48.8 mmHg, PaCO2 32.16 mmHg. The liver functions tests found ALT 166.8 IU/L, AST 270.5 IU/L.
Diagnostic Imaging
By chest X-ray (Fig. 11.103a), flaky shadows with increased density in both lungs, especially in the both lower lungs; enlarged and blurry hilum.
By chest X-ray (Fig. 11.103b), flaky shadows with increased density in both lungs, especially in the right lower lung and the left lung; enlarged and blurry hilum.
Pathology Analysis
By H&E staining (Fig. 11.103c), interalveolar walls space widened; alveolar wall congestion; infiltration of neutrophils and plasma cells (mainly mononuclear cells); intraalveolar edema and cellulose exudates by H&E staining.
By H&E staining (Fig. 11.103d), hyaline membrane formed in the alveoli.
By H&E staining (Fig. 11.103e), alveolar epithelium detached; cellulose in some alveolar cavities exudates.
By H&E staining (Fig. 11.103f), large amount of hyaline membrane formed in the alveoli.
By H&E staining (Fig. 11.103g), blood vessels in alveolar wall congestion.
By H&E staining (Fig. 11.103h), more intraalveolar cellulose exudates.
By H&E staining (Fig. 11.103i), thin alveolar walls; occlusion of blood vessels in the alveolar walls; large number of intraalveolar cellulose exudates.
By H&E staining (Fig. 11.103j), type I epithelial cells detached and necrotic, with following type II epithelial cells slightly proliferate.
By H&E staining (Fig. 11.103k), intraalveolar loose cellulose exudates.
By H&E staining (Fig. 11.103l), intraalveolar dense cellulose exudates.
By Masson’s staining (Fig. 11.103m), large number of intraalveolar cellulose exudates, with no growth of bacteria.
By PAS staining (Fig. 11.103n), large number of intraalveolar cellulose exudates.
By P immunohistochemical staining (Fig. 11.103o), large number of macrophages gather and clump.
By AFB staining (Fig. 11.103q), large numbers of inflammatory cells infiltration but with no acid-fast bacilli.



Fig. 11.103
Case 11.104
History of Present Illness. A 48-years-old man, complained of fever for 5 days, with the highest temperature of 39 °C. He also had expectoration of yellowish phlegm, spasmodic breathing and chest distress. Death occurred with following autopsy.
Past History. Histories of diabetes, chronic renal dysfunction, chronic bronchitis.
Contact History. Self reported no history of contacting with any Influenza A (H1N1) patient.
Signs. Pharyngeal congestion. Tonsils swollen to I degree.
Laboratory Tests
Throat swabs by CDC found universal gene of Influenza A virus (gene M) positive, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
On Nov. 28th, 2009, blood gas analysis found pH 7.13, PaCO2 41 mmHg, PaO2 60 mmHg. Routine blood tests found leukocytes count 8.1 × 109/L, erythrocytes count 2.49 × 1012/L. Blood biochemistry found AST 76.3 U/L, ALT 13.4 U/L.
On Nov. 30th, 2009, blood gas analysis found pH 7.19, PaCO2 38 mmHg, PaO2 85 mmHg. Routine blood tests found leukocytes count 14.59 × 109/L, erythrocytes count 3.0 × 1012/L. Blood biochemistry found AST 44.3 U/L, ALT 11.7 U/L.
On Dec. 6th, 2009, blood gas analysis found pH 7.34, PaCO2 40 mmHg, PaO2 80 mmHg. Blood biochemistry found K+ 4.0 mmol/L, Na+ 130 mmol/L, Cr 161.6 μmol/L.
On Dec. 7th, 2009, urine culture found Enterococci faecium. Sputum culture found bur kholderia cepacia.
On Dec. 12th, 2009, blood gas analysis found pH 7.19, PaCO2 47 mmHg, PaO2 168 mmHg. Routine blood tests found leukocytes count 11.51 × 109/L. Blood biochemistry found UREA 32.06 mmol/L, Cr 813.5 μmol/L, Cr 813.5 μmol/L, K+ 7.76 mmol/L, Na+ 130 mmol/L.
Diagnosis. Critical pneumonia complicating Influenza A (H1N1).
Pathological Analysis
By H&E staining (Fig. 11.104a, b), capillary edema and congestion; inflammatory cells infiltration.
By H&E staining (Fig. 11.104c, d), large number of inflammatory cells infiltration in the myocardial tissues.

Fig. 11.104
Case 11.105
History of Present Illness. A 45-years-old woman, complained of chills and fever for 5 days, with the highest temperature of 39.5 °C. She also suffered from eyes upsets, dry cough, a little phlegm, chest distress and suffocation. He was diagnosed as having bronchitis in another hospital and received therapies of anti-inflammation, but with outcomes of chest distress, shortness of breath. He was then transferred to You’an Hospital in Beijing for treatment, but occurrence of death due to respiratory failure.
Past History. Denied histories of major basic diseases.
Contact History. Denied history of contacting with any definitively diagnosed Influenza A (H1N1) patient or patients with flu liked symptoms.
Signs. Pharyngeal congestion. Body temperature 39 °C.
Laboratory Tests
By throat swabs, universal gene of Influenza A virus (gene M) negative, universal gene of H1N1 swine flu (gene NP) positive, specific gene of Influenza A (H1N1) virus (gene HA) positive.
On Nov. 15th, 2009, throat swabs found gene M positive, gene NP positive, gene HA negative.
On Nov. 13th, 2009, blood gas analysis found pH 7.466, PaCO2 35.5 mmHg, PaO2 76.0 mmHg; routine blood tests found leukocytes count 2.84 × 109/L, neutrophils 83.8 %, lymphocytes 12 %.
On Nov. 14th, 2009, blood gas analysis found pH 7.471, PaCO2 31.8 mmHg, PaO2 43.6 mmHg; routine blood tests found leukocytes count 3.39 × 109/L, neutrophils 81.1 %, lymphocytes 14.5 %; liver functions tests found ALT 21.1 U/L, AST 51.3 U/L, UREA 3.34 mmol/L, CREA 41.0 μmol/L.
On Nov. 15th, 2009, blood gas analysis found pH 7.438, PaCO2 36.5 mmHg, PaO2 69.3 mmHg; routine blood tests found leukocytes count 2.18 × 109/L, neutrophils 84 %, lymphocytes 12.8 %.
On Nov. 18th, 2009, blood gas analysis found pH 7.488, PaCO2 33.2 mmHg, PaO2 46.9 mmHg; routine blood tests found leukocytes count 3.69 × 109/L, neutrophils 67.7 %, lymphocytes 24.7 %; liver functions tests found ALT 62.9 U/L, AST 144.4 U/L, CREA 46.3 μmol/L, Glu 7.45.
On Nov. 20th, 2009, blood gas analysis found pH 7.460, PaCO2 34 mmHg, PaO2 79 mmHg; routine blood tests found leukocytes count 9.8 × 109/L, neutrophils 82.6 %, lymphocytes 9.4 %, erythrocytes count 3.23 × 1012/L, Hb 102 g/L; liver functions tests found ALT 257.4 U/L, AST 91.5 U/L, UREA 8.12 mmol/L, CREA 51.4 μmol/L.
On Nov. 30th, 2009, blood gas analysis found pH 7.310, PaCO2 58 mmHg, PaO2 78 mmHg; routine blood tests found leukocytes count 11.25 × 109/L, neutrophils 83.5 %, lymphocytes 11.8 %, Hb 102 g/L; liver functions tests found ALT 44 U/L, AST 149 U/L, UREA 4.83 mmol/L, CREA 33.5 μmol/L.
Diagnostic Imaging
By chest X-ray on Nov. 16th, 2009 (Fig. 11.105a), diffusive large flaky shadows with increased density in both middle lower lungs; boundaries blurry.
By chest X-ray on Nov. 27th, 2009 (Fig. 11.105b), diffusive large flaky shadows with increased density in both middle lower lungs, decreased transparency of both lungs and progressive conditions compared to chest X-ray findings on Nov. 16th, 2009.
By chest X-ray on Dec. 4th, 2009 (Fig. 11.105c), diffusive shadows with increased density in both lungs; decreased transparency of both lungs; hilum blurry; progressive conditions compared to chest X-ray findings on Nov. 27th, 2009.
By chest X-ray on Dec. 18th, 2009 (Fig. 11.105d), diffusive shadows with increased density in both lungs; thickened shadows, parenchymal changes and improved transparency of both pulmonary apex compared to X-ray findings on Dec. 4th, 2009.
By chest X-ray on Dec. 19th, 2009 (Fig. 11.105e), diffusive shadows with increased density in both lungs; improved transparency of the left lung compared to the chest X-ray findings on Dec. 4th, 2009.
By chest X-ray on Dec. 20th, 2009 (Fig. 11.105f), diffusive shadows with increased density in both lungs; parenchymal lung tissues fibrosis.
By chest CT scanning 72 h after death on Dec. 26th, 2009 (Fig. 11.105g–j), large amount of effusion in bilateral chest cavities; left gas fluid level.
Pathological Analysis and Autopsy
Gross autopsy findings:
Figure 11.105k: 72 h after death, lung tissues fibrosis and patchy bleeding.
Figure 11.105l: H&E staining found a few alveolar cells, most lung tissues fibrosis, large amount of inflammatory cells; intraalveolar bleeding.
Figure 11.105m: H&E staining found a few alveolar cells, most lung tissues fibrosis, no bronchiolar epithelium; large amount of inflammatory cells (mainly macrophages); all the findings in line with diffusive alveolar impairments after necrotic bronchitis; intraalveolar bleeding.
Figure 11.105n: H&E staining found many inflammatory cells in hepatocellular spaces.
Figure 11.105o: H&E staining found many inflammatory cells in hepatocellular spaces.
Figure 11.105p: H&E staining found renal sinus dilation; many inflammatory cells in renal parenchymal spaces.
Figure 11.105q: H&E staining found renal sinus dilation; many inflammatory cells in renal parenchymal spaces.
Figure 11.105r: H&E staining found a few inflammatory cells in myocardial cells spaces.
Figure 11.105s: H&E staining found a few inflammatory cells in myocardial cells spaces.
Diagnosis. Critical Influenza A (H1N1).




Fig. 11.105
Case 11.106
History of Present Illness. A 22-years-old woman, complained of fever in late pregnancy with no known causes. For the clinic visit, she had fever 6 days ago and had had continual fever with the highest temperature of 39 °C. She suffered from remittent fever with chills, shivers, sore throat but no pharynx soreness. In addition, she had intermittent moderate cough, with a few phlegm and shortness of breath. Two days before admission, she delivered a baby boy after natural labor and she was admitted due to obvious shortness of breath, increased frequency of breathing, cyanosis and spasmodic breathing. Her conditions progressively deteriorated and death occurred because of respiratory failure.
Past History. Denied history of major basic diseases.
Contact History. Denied the history of contacting with any definitively diagnosed Influenza A (H1N1) patient or any patient with flu liked symptoms.
Signs. Pharyngeal congestion. The highest body temperature of 39 °C.
Laboratory Tests
On Nov. 30th, 2009, the throat swabs by local CDC found universal gene of flu virus (gene HA) positive.
On Dec. 2nd, 2009, routine blood tests, blood gas analysis and blood biochemistry found leukocytes count 14.37 × 109/L, hemoglobin 73 g/L, neutrophils 82 %, pH 7.38, PaCO2 33 mmHg, PaO2 66 mmHg, ALT 330 U/L, AST 2,650 U/L, ALB 23.7 g/L, Cr 58.9 μmol/L, UREA 2.49 nmol/L, K+ 3.9 mol/L, Na+ 135 mmol/L. And blood smear found rod nuclear cells 17 %, metamyelocyte 3 %.
On Dec. 7th, 2009, routine blood tests found leukocytes count 19.48 × 109/L, hemoglobin 84 g/L, neutrophils 90.6 %, pH 7.40, PaCO2 35 mmHg, PaO2 60 mmHg, SaO2 90.9 %.
On Dec. 8th, 2009, routine blood tests found leukocytes count 11.71 × 109/L, hemoglobin 70 g/L, neutrophils 91.3 %, pH 7.43, PaCO2 40 mmHg, PaO2 61 mmHg, SaO2 91.7 %.
On Dec. 10–12th, 2009, sputum culture found Acinetobacter baumannii, only sensitive to polymyxin.
On Dec. 14th, 2009, routine blood tests found leukocytes count 12.81 × 109/L, hemoglobin 80 g/L, neutrophils 83 %, pH 7.32, PaCO2 58 mmHg, PaO2 93 mmHg, SaO2 96.3 %, ALT 23 U/L, AST 22 U/L, ALB 36.3 g/L, Cr 41.6 μmol/L, UREA 3.57 nmol/L, K+ 3.8 mol/L, Na+ 135 mmol/L. Sputum culture found Acinetobacter baumannii.
Diagnostic Imaging
By chest X-ray on Dec. 2nd, 2009 (Fig. 11.106a), large flaky shadows with increased density in both lungs; obviously decreased transparency of most lung.
By chest X-ray on Dec. 5th, 2009 (Fig. 11.106b), large flaky shadows with increased density; shadows thickened and fused with parenchymal changes and obviously progressive conditions compared to chest X-ray findings on Dec. 2nd, 2009.
By chest X-ray on Dec. 13th, 2009 (Fig. 11.106c), diffusive cloud mist liked shadows with increased density in both lungs; compared to the chest X-ray findings on Dec. 5th, 2009, the shadows light and improved transparency of both lungs but still having large lesion field and decreased transparency of lungs.
By chest X-ray on Dec. 27th, 2009 (Fig. 11.106d), diffusive cloud mist liked shadows with increased density in both lungs; compared to the chest X-ray findings on Dec. 13th, 2009, the shadows thickened and fused and improved transparency of both upper lungs but still having poor transparency of both lungs.
By chest CT scanning 2 h after death on Dec. 29th, 2009 (Fig. 11.106e–h), large amount of effusion of bilateral chest cavities; the right hydropneumothorax.
Pathological Analysis and Autopsy
Figure 11.106i, j: pulmonary tissues surface 2 h after death; decreased lung volume, extensive fibrosis and diffusive patchy bleeding.
Figure 11.106k: H&E staining found a few alveolar cells; fibrosis of most lung tissues; many inflammatory cells; intraalveolar bleeding.
Figure 11.106l: H&E staining found a few alveolar cells; fibrosis of most lung tissues; no bronchiolar epithelial cells; many inflammatory cells (mainly macrophages); the findings in line with extensive alveolar impairments after necrotic bronchitis; intraalveolar bleeding.
Figure 11.106m: H&E staining found fibrosis of lung tissues and alveolar bleeding.
Figure 11.106n: H&E staining found many inflammatory cells in the hepatocellular spaces; hepatic sinusoid dilation; large number of erythrocytes in phagocytes.
Figure 11.106o: H&E staining found many inflammatory cells in hepatocellular spaces; necrosis of liver cells in fragments.
Figure 11.106p: H&E staining found renal sinus dilation; several inflammatory cells in the renal parenchymal spaces.
Figure 11.106q: H&E staining found renal sinus dilation; several inflammatory cells in the renal parenchymal spaces.
Figure 11.106r: H&E staining found a few inflammatory cells in myocardial cells spaces.
Figure 11.106s: H&E staining found a few inflammatory cells in myocardial cells spaces.




Fig. 11.106
Reference
Perez-Padilla R, de la Rosa-Zamboni D, Ponce de Leon S, et al. Pneumonia and respiratory failure from swine-origin influenza A (H1N1) in Mexico. N Engl J Med. 2009;361:680–9.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media B.V., Dordrecht and Tsinghua University Press
About this chapter
Cite this chapter
Hongjun, L., Ning, L. (2013). Diagnostic Imaging of Chest. In: Li, H., Li, N. (eds) Radiology of Influenza A (H1N1). Springer, Dordrecht. https://doi.org/10.1007/978-94-007-6162-9_11
Download citation
DOI: https://doi.org/10.1007/978-94-007-6162-9_11
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-007-6161-2
Online ISBN: 978-94-007-6162-9
eBook Packages: MedicineMedicine (R0)