
Abstract
Misperceptions regarding the causes, presentation, and diagnosis of acute compartment syndrome (ACS) can lead to a delay in its diagnosis and treatment that negatively impact patient outcomes. Open fractures do not have a lower risk of ACS compared to closed fractures. Acute compartment syndrome frequently presents without a fracture, and when it does, a delay in its diagnosis is more likely. Pain, not pallor, pulselessness, paresthesias, or paralysis, is the only reliable early clinical finding in an awake and alert patient. A single examination or intracompartmental pressure measurement cannot reliably diagnose or exclude ACS in at-risk patients. The misperceptions, low incidence, and numerous causes of ACS result in a low level of awareness among health-care professionals. Continued education, institutional protocols, and additional research may be necessary to raise awareness and improve the early detection of ACS.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Acute limb compartment syndrome
- Missed compartment syndrome
- Delayed compartment syndrome
- Misperceptions
Background to the Problem
-
Misperceptions regarding the causes, presentation, and diagnosis of acute compartment syndrome (ACS) can lead to a delay in its diagnosis and treatment that negatively impact patient outcomes.
-
The misperceptions, low incidence, and numerous causes of acute compartment syndrome result in a low level of awareness among health-care professionals.
-
There is controversy surrounding the best method to diagnose acute compartment syndrome.
-
A high degree of suspicion among health-care professionals is necessary to prevent a delay in the diagnosis of acute compartment syndrome.
What Is Recommended
Misperceptions regarding the causes, presentation, and diagnosis of acute compartment syndrome (ACS) can lead to a delay in its diagnosis and treatment that negatively impact patient outcomes. Health-care professionals should be properly educated on ACS to dispel these misperceptions in order to prevent the devastating consequences of a missed compartment syndrome.
Misperception #1: Open fractures do not develop acute compartment syndrome
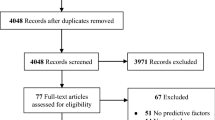
Up to 70% of ACS occurs in the presence of fractures, most commonly the tibial shaft (36%) and the distal radius (10%) [1]. Open fractures present with a defect in the fascial compartments and might intuitively thought to be at a lower risk of ACS (Fig. 16.1). However, the incidence of ACS in open tibial shaft fractures has not been shown to differ from that of closed fractures, ranging from 5% to 9%, with all four compartments of the leg being susceptible to ACS [2,3,4]. Providers must continue to monitor these patients for the signs and symptoms of ACS in the setting of open fracture.

Photograph of a patient presenting with a grossly open femur fracture who subsequently developed acute compartment syndrome. Large open wounds do not preclude the development of acute compartment syndrome
Misperception #2: A diagnosis of acute compartment syndrome is unlikely if there is no fracture
Around 30% of all ACS presents without an associated fracture [5]. When ACS presents without a fracture, a delayed diagnosis is more likely [1, 5]. Hope et al. [5] found a significantly longer delay to fasciotomy for ACS without fracture (34 versus 21 hours) along with a higher incidence of muscle necrosis at the time of fasciotomy (21% vs 8%) suggesting that this delay was detrimental to the patient.
There are numerous causes of ACS that do not involve fracture, including both traumatic and nontraumatic causes [6, 7]. Traumatic causes include injuries that crush, burn, penetrate, or compress. Even minor trauma can result in ACS in patients with bleeding disorders or anticoagulation medication. Nontraumatic causes include, but are not limited to, ischemia–reperfusion injuries, bleeding diatheses, intravenous (IV) extravasation, IV drug abuse, envenomation, nephrotic syndrome, and infection. The extensive list of potential causes means that ACS can present to health-care professionals over a wide range of specialties making it necessary for all providers to understand the presentation and diagnosis of ACS in order to prevent a delay in its treatment.
Misperception #3: The five “Ps” of acute compartment syndrome: Pain, pallor, pulselessness, parasthesias, and paralysis
It is important to consider ACS in the setting of any painful and tense muscle compartment. It has been classically taught that the clinical exam findings of ACS present as the “5 Ps” (pain, pallor, pulselessness, paresthesias, and paralysis) [3, 6, 7]. However, these findings represent arterial insufficiency and typically present in the late stages of compartment syndrome [6, 8, 9]. Instead, the “5 Ps” of ACS have been recommended by one author to be changed to pain, pain, pain, pain, and more pain; specifically, pain with passive stretch of the muscle compartment, pain out of proportion to that of the injury, and pain that is unresponsive to adequate analgesia [6]. Despite this recommendation, the sensitivity of pain is still low [9]. An analysis of four prospective trials involving the lower extremity determined that pain, pain with passive stretch, and paresthesias on exam had a sensitivity of 13–19% and a specificity of 97–98%, suggesting that the absence of these symptoms was better at excluding the diagnosis than ruling it in [9]. The presence of multiple clinical findings does increase the probability, with the likelihood of ACS increasing from 25%, to 68%, and to 98% with one, two, and three findings, respectively. Additionally, the ability of physicians to discern critically high intracompartmental pressure from baseline levels via palpation of muscle compartments has been shown to be poor and should not be relied on [10].
Misperception #4: A one-time elevated intracompartmental pressure measurement is diagnostic of acute compartment syndrome
There is no clear validated criteria for when ACS is actually present [7]. There is controversy surrounding the appropriate method to diagnose ACS. Classically, ACS has been diagnosed by the clinical exam of an awake and alert patient, while ICP monitoring is reserved for those with unreliable clinical exams. This is reflected in a recent survey of orthopedic traumatologists that demonstrated a strong consensus that the diagnosis of ACS should be made clinically based on the presence of a tense muscle compartment, pain with passive stretch, and pain out of proportion to the injury [11]. There was also a strong consensus that ICP monitoring should be used when the clinical exam was unreliable such as in children, multiply injured, or obtunded patients. In contrast, the routine use ICP monitoring in awake and alert patients was only supported by 18% of the respondents. While the clinical exam may be the standard for diagnosing ACS for many, the poor sensitivity of these findings has led some authors to recommend for routine ICP monitoring in at-risk patients [1, 7, 12]. Mcqueen et al. [13] were able to correctly identify all cases of ACS in a prospective cohort using a perfusion differential threshold of less than 30 mmHg between the diastolic blood pressure and the ICP. While this method is highly sensitive resulting in very few missed cases of ACS, other authors argue that ICP monitoring is not only costly and burdensome for the hospital staff but also nonspecific, leading to gross overtreatment [14, 15]. This appears to be especially true if one-time ICP measurements are used to make the diagnosis [14,15,16]. Whitney et al. [14] performed one-time ICP measurements in tibial shaft fractures with no exam findings of ACS and found that 35% of patients had perfusion differential <30 mmHg demonstrating that the use of this threshold would have led to a high rate of unnecessary fasciotomies in this population. In contrast to one-time ICP measurements, Mcqueen et al. [12] reviewed 850 tibial shaft fractures that underwent routine continuous ICP monitoring and found that a mean perfusion differential threshold of less than 30 mmHg for two consecutive hours had excellent sensitivity and specificity, 94% and 98%, respectively, for diagnosing ACS, making a strong argument for the use of routine continuous ICP monitoring in at-risk patients.
Limitations and Pitfalls
The misperceptions of ACS can ultimately result in a delayed or missed diagnosis, both of which can be devastating for patients. The timely and accurate diagnosis of ACS remains challenging due to the multitude of insults that can cause it, the inconsistent exam findings, and its presence in patients who cannot reliably communicate. These difficulties make a delayed diagnosis of ACS nearly inevitable. Physicians, advanced practitioners, and nurses must be appropriately educated to dispel the abovementioned misperceptions in order to have the appropriate level of suspicion necessary to detect and treat ACS in a timely manner. Whether using clinical exam findings, ICP monitoring, or both to diagnose ACS, it is important to understand that ACS is a disease process that develops over time making serial examinations or continuous ICP monitoring a necessity.
Future Directions
Continued education and institutional protocols are potential tools for correcting the misperceptions of ACS. In an effort to improve the early identification of ACS at one academic hospital, Schaffzin et al. [17] implemented a series of changes with the goal of increasing the number of at-risk patients that received appropriate orders for, performance of, and documentation of serial neurovascular examinations. These institutional changes included provider and nursing reminders, modifications to electronic medical record order sets, mandatory education, and formal lectures. The use of chart inserts and checklists have also been used to help increase the identification and monitoring of at-risk patients for ACS [18].
The implementation of educational programs, order sets, and checklists may be able to better identify and monitor patients at risk of ACS; however, additional research is still necessary to develop clear and validated criteria for when ACS is actually present. Advanced diagnostic tests for the identification of ACS have been investigated extensively, including biomarkers for muscle damage and ischemia, magnetic resonance imaging, ultrasound, scintigraphy, laser Doppler flowmetry, near-infrared spectroscopy, and direct hardness measurements, but none of these tests have demonstrated superiority to the clinical exam and ICP monitoring [3, 7]. Schimdt et al. [19] performed a multicenter prospective trial that combined continuous ICP monitoring, near-infrared spectroscopy muscle oxygenation, clinical exam findings, and 6-month outcome scores in order to develop a predictive model for ACS. The application of this predictive model to future prospective studies has the potential to develop a more reliable diagnostic criteria for ACS.
Take-Home Message
-
Acute compartment syndrome should be considered in at-risk patients presenting with a tense painful muscle compartment.
-
Open fractures are still at risk of developing acute compartment syndrome.
-
Acute compartment syndrome presenting without a fracture is more likely to have a delayed diagnosis.
-
Pain is the only reliable early clinical finding, while pallor, pulselessness, paresthesias, and paralysis present later.
-
Reliance on one-time intracompartmental pressure monitoring will result in a high rate of unnecessary fasciotomies.
-
Continuous intracompartmental pressure monitoring is the most sensitive and specific test for acute compartment syndrome.
-
Educational programs, order sets, checklists, and improved diagnostic techniques are potential tools to dispel the misperceptions of acute compartment syndrome and to prevent a delayed diagnosis.
References
McQueen MM, Gaston P, Court-Brown CM. Acute compartment syndrome. Who is at risk? J Bone Joint Surg Br [Internet]. 2000 Mar [cited 2018 Apr 8];82(2):200–3. Available from: http://www.ncbi.nlm.nih.gov/pubmed/10755426.
Blick SS, Brumback RJ, Poka A, et al. Compartment syndrome in open tibial fractures. J Bone Joint Surg Am [Internet]. 1986 Dec [cited 2018 Apr 14];68(9):1348–53. Available from: http://www.ncbi.nlm.nih.gov/pubmed/3782206.
Shadgan B, Pereira G, Menon M, et al. Risk factors for acute compartment syndrome of the leg associated with tibial diaphyseal fractures in adults. J Orthop Traumatol [Internet]. 2015 Sep 28 [cited 2018 Apr 14];16(3):185–92. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25543232.
DeLee JC, Stiehl JB. Open tibia fracture with compartment syndrome. Clin Orthop Relat Res [Internet]. 1981 Oct [cited 2018 Apr 8];(160):175–84. Available from: http://www.ncbi.nlm.nih.gov/pubmed/7026116.
Hope MJ, McQueen MM. Acute compartment syndrome in the absence of fracture. J Orthop Trauma [Internet]. 2004 Apr [cited 2018 Apr 8];18(4):220–4. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15087965.
von Keudell AG, Weaver MJ, Appleton PT, et al. Diagnosis and treatment of acute extremity compartment syndrome. Lancet [Internet]. 2015 Sep 26 [cited 2018 Apr 8];386(10000):1299–310. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26460664.
Schmidt AH. Acute compartment syndrome. Injury [Internet]. 2017 Jun [cited 2018 Apr 15];48:S22–5. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28449851.
Mubarak SJ, Owen CA, Hargens AR, et al. Acute compartment syndromes: diagnosis and treatment with the aid of the wick catheter. J Bone Joint Surg Am [Internet]. 1978 Dec [cited 2018 Apr 8];60(8):1091–5. Available from: http://www.ncbi.nlm.nih.gov/pubmed/721856.
Ulmer T. The clinical diagnosis of compartment syndrome of the lower leg: are clinical findings predictive of the disorder? J Orthop Trauma [Internet]. 2002 Sep [cited 2018 Apr 8];16(8):572–7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12352566.
Shuler FD, Dietz MJ. Physicians’ ability to manually detect isolated elevations in leg intracompartmental pressure. J Bone Joint Surg Am [Internet]. 2010 Feb [cited 2018 Apr 8];92(2):361–7. Available from: http://insights.ovid.com/crossref?an=00004623-201002000-00013.
Collinge C, Attum B, Tornetta P, et al. Acute compartment syndrome: an expert survey of Orthopedic Trauma Association (OTA) members. J Orthop Trauma [Internet]. 2018 Jan 24 [cited 2018 Apr 8];1. Available from: http://insights.ovid.com/crossref?an=00005131-900000000-98659.
McQueen MM, Duckworth AD, Aitken SA, et al. The estimated sensitivity and specificity of compartment pressure monitoring for acute compartment syndrome. J Bone Joint Surg [Internet]. 2013 Apr 17 [cited 2018 Apr 14];95(8):673–7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23595064.
McQueen MM, Court-Brown CM. Compartment monitoring in tibial fractures. The pressure threshold for decompression. J Bone Joint Surg Br [Internet]. 1996 Jan [cited 2018 Apr 15];78(1):99–104. Available from: http://www.ncbi.nlm.nih.gov/pubmed/8898137.
Whitney A, O’Toole RV, Hui E, et al. Do one-time intracompartmental pressure measurements have a high false-positive rate in diagnosing compartment syndrome? J Trauma Acute Care Surg [Internet]. 2014 Feb [cited 2018 Apr 14];76(2):479–83. Available from: https://insights.ovid.com/crossref?an=01586154-201402000-00033.
Harris IA, Kadir A, Donald G. Continuous compartment pressure monitoring for tibia fractures: does it influence outcome? J Trauma Inj Infect Crit Care [Internet]. 2006 Jun [cited 2018 Apr 14];60(6):1330–5. Available from: https://insights.ovid.com/crossref?an=00005373-200606000-00025.
Bistolfi A, Massazza G, Verné E, et al. Antibiotic-loaded cement in orthopedic surgery: a review. ISRN Orthop. [Internet]. 2011 Aug 7 [cited 2018 Mar 9];2011:1–8. Available from: https://www.hindawi.com/archive/2011/290851/.
Schaffzin JK, Prichard H, Bisig J, et al. A collaborative system to improve compartment syndrome recognition. Pediatrics [Internet]. 2013 Dec 1 [cited 2018 Apr 20];132(6):e1672–9. Available from: http://pediatrics.aappublications.org/cgi/doi/10.1542/peds.2013-1330.
Cascio BM, Pateder DB, Farber AJ, et al. Improvement in documentation of compartment syndrome with a chart insert. Orthopedics [Internet]. 2008 Apr [cited 2018 Apr 20];31(4):364. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19292285.
Schmidt AH, Bosse MJ, Frey KP, et al. Predicting Acute Compartment Syndrome (PACS): the role of continuous monitoring. J Orthop Trauma [Internet]. 2017 Apr [cited 2018 Apr 15];31 Suppl 1:S40–7. Available from: http://insights.ovid.com/crossref?an=00005131-201704001-00009.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2019 The Author(s)
About this chapter

Cite this chapter
Parry, J.A. (2019). Common Misperceptions Among Health-Care Professionals. In: Mauffrey, C., Hak, D., Martin III, M. (eds) Compartment Syndrome. Springer, Cham. https://doi.org/10.1007/978-3-030-22331-1_16
Download citation
DOI: https://doi.org/10.1007/978-3-030-22331-1_16
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-22330-4
Online ISBN: 978-3-030-22331-1
eBook Packages: MedicineMedicine (R0)