
Abstract
Africa bears the major brunt of the global Buruli ulcer (BU) burden. In the past decade, more than 95% of all cases have been reported from Africa, with Côte d’Ivoire, Ghana, Benin, and Cameroon being the four most endemic countries. As the disease affects mainly populations in remote, rural areas, where access to formal healthcare structures is limited, the true prevalence of BU is difficult to gauge. The continued preference of BU patients in many of these endemic areas to first consult traditional healers before seeking biomedical treatment, results in a high proportion of patients with advanced stages of the disease, which often cause permanent disabilities. Reasons for a marked reduction of new infections reported from Africa in the past few years are poorly understood and include—apart from an actual reduction in BU incidence—the decline in international support for BU control programs and consequently decreased BU case-finding activities. Major efforts are required in the coming years to mobilize resources to maintain established healthcare infrastructure, surveillance systems, and expertise among health staff. Continued research is needed to solve serious challenges in the diagnosis and treatment of patients at primary healthcare facilities and district hospitals and to fill knowledge gaps on environmental reservoirs, potential vectors, and transmission mechanisms of Mycobacterium ulcerans, a crucial prerequisite for more targeted BU control strategies.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


1 Introduction
The first description of skin lesions resembling those caused by Mycobacterium ulcerans, dates back to the late nineteenth century, when the missionary physician Albert Cook [1] recorded a range of chronic, necrotizing skin ulcers in patients in Uganda. In the 1950s and 1960s a larger case series of patients with similar ulcers was detected in today’s Nakasongola district in Uganda [2, 3], formerly known as Buruli County. Since then, cases of the disease, henceforth designated “Buruli ulcer” (BU), were reported from 20 additional African countries, where the major burden commonly falls on children aged five to 15 years. BU in Africa is characterized by a patchy geographical distribution, affecting mainly rural communities with often very high local prevalence rates. Access to the formal health sector in these regions is limited and as a result knowledge on the actual distribution and frequency of infections is scanty [4]. The occurrence of M. ulcerans infections in Africa is closely linked to areas of land drained by rivers and their tributaries. While the probability of person-to-person transmission is thought to be very low, the nature of relevant environmental reservoirs is highly controversial and the mode by which the pathogen is transmitted from environmental sources to humans is not clarified [5, 6]. Several routes for the introduction of M. ulcerans into the susceptible layers of the skin are discussed.
Causes of BU disease are commonly perceived by the local population as somewhat mysterious and are often associated with witchcraft or sorcery [7,8,9]. Also insect bites, contamination of skin lesions, and contact with swamps and water bodies often connected with changes in ecology are considered risk factors for contracting BU and a concept of dual causality is frequently encountered, particularly among affected populations in West African countries [9]. As a consequence, patients may first consult traditional healers or prayer camps to deal with witchcraft before seeking biomedical treatment at hospitals or health centers. Other patients may consider care seeking at the formal health sector only as a last resort [8, 10, 11]. Findings from a biosocial analysis of BU among fishermen in northwestern Uganda revealed that late presentation for biomedical treatment resulted from a perceived lack of its efficacy and a perceived efficacy of herbalists’ treatment, which was sought promptly after first signs of lesions appeared [12]. These insights explain why in many BU endemic regions a high proportion of patients present to formal health facilities with large lesions, which require extended periods for healing and often result in permanent disabilities. According to the WHO classification system, BU lesions fall into one of three categories. Category I includes single, small lesions (nodules or ulcers) below five cm in diameter, Category II comprises single lesions between five and 15 cm in diameter as well as plaque and edematous forms, and Category III includes single lesions above 15 cm in diameter, multiple lesions, lesions at critical sites such as eyes, genitalia, and joints, as well as osteomyelitis [13]. Category II and III lesions are particularly prevalent in remote areas, where access to healthcare is limited and awareness of the disease is low. Surveillance and reporting of cases supported by community health workers, teachers, and other community volunteers are important elements for the control of BU. As long as preventable risks are not clearly identified and no vaccine is available, the main goal is to diagnose and treat patients in an early disease stage, when most lesions heal fast and without adjunct surgical treatment so that long-term sequelae and other complications can be avoided.
A momentum for the establishment of organized National BU Control Programs (NBUCPs) in the most affected countries was created by the Yamoussoukro Declaration and the global BU Initiative, launched by WHO in 1998 [14]. The three main pillars of global and national BU control strategies included (1) the strengthening of health systems by the development of infrastructure and provision of training for health workers, (2) sensitization and involvement of communities by information and education campaigns to facilitate early case detection and reporting, and (3) standardized case management in terms of diagnosis, treatment, and prevention of disability.
BU has been reported from five of the six WHO regions except the European region [4]. However, Africa bears the brunt of the disease burden with around 57,500 cases reported to WHO from 16 African countries between 2002 and 2016, representing 98% of all BU cases recorded worldwide during that time. The decreasing numbers of cases reported to WHO in the past couple of years play their part in further neglect of BU. Major efforts are required in the coming years to mobilize resources for the establishment, maintenance, and expansion of BU control activities.
2 Management of BU in Africa
2.1 Structure of Health Systems in Africa and Implications for the Management of BU
Health systems are organized in many African countries in three levels, each composed of administrative structures and care facilities [15, 16]. The central (tertiary) level constituted by the technical departments of the Ministry of Public Health is in charge of the development of national health strategies, national hospitals as well as reference laboratories. In the case of BU, control activities at this level are organized by NBUCPs, which define control strategies, plan the implementation of interventions, supervise and evaluate these interventions. National hospitals are usually not directly involved in the management of BU patients, whereas laboratory confirmation of suspected BU patients by PCR analysis is performed by national reference laboratories. The intermediate (secondary) level is composed of regional delegations of public health and regional hospitals, supervising control activities for BU. The peripheral (primary) level, where the implementation of BU control activities is based, is the health district, comprising the district health service, district hospitals, primary health centers, and communities. While the district health service organizes community sensitization and BU case-finding in collaboration with the primary health centers and community stake-holders, the district hospitals act as BU diagnostic and treatment centers (BU-DTCs), supervise BU care in primary health centers, and assist the district health service in community-based activities.
BU-DTC facilities have in the past often been built or rehabilitated and equipped by support partners to provide adequate infrastructure for BU diagnosis and treatment, including surgical theatres, wound dressing rooms, laboratories, physiotherapy units, and admission wards. Within the framework of national BU surveillance, all BU-DTCs are provided with BU case-definition, diagnostic and treatment guidelines and other documentation on the disease for use by health workers. Standard WHO BU case record files and registers referred to as BU01 and BU02 forms, respectively, are used at the BU-DTCs to document information on each patient. The BU-DTC health staff receives specific training through workshops organized by the NBUCPs and facilitated by BU experts, using the WHO training modules and guidelines on BU care. The data recording and reporting process at BU-DTCs is regularly monitored and supervised by the NBUCPs to ensure correctness and completeness [17, 18].
Main activities of the BU-DTCs include early case detection at the community level, training of village health workers and strengthening of the community-based surveillance system, information, education, and communication campaigns in communities and schools, strengthening of the health system and infrastructure, management of equipment, transport and logistics, standardized recording and reporting using WHO BU01 and BU02 forms, standardized case management (diagnosis and treatment), prevention of disability/rehabilitation, supportive activities, advocacy, social mobilization, partnerships, and operational research.
Box 1: Benin
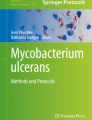
The first case of BU in Benin was registered in 1977 at the Saint Camille Hospital in Dogbo (Couffo Department). A first focus of the disease was detected in the Ouinhi district (Zou Department) in 1988 [19], cases of which were reported by Muelder and Nourou in 1990 [20]. The NBUCP in Benin was created in 1997 and surveillance using the WHO BU01 and BU02 forms started in 2003. In Benin, there are four peripheral BU-DTCs, which are locally referred to as ‘Centre de Dépistage et de Traitement de l’Ulcère de Buruli (CDTUB)’. These centers, which are responsible for the implementation of BU control activities, are distributed across the main endemic regions and located in Allada, Lalo, Pobe, and Zangnanado (Fig. 1). Health workers at these facilities have considerable experience in diagnosing and treating BU patients. Early case detection and referral of patients to the CDTUBs is supervised by health workers of the nearest health post, but relies strongly on community-based surveillance teams, comprising village volunteers (‘relais communautaires’) and teachers (‘focal points’). These teams are also responsible for the follow-up of patients after treatment. In order to facilitate reporting at each CDTUB, BU cases are registered on a BU02 form, which is sent out each quarter to regional authorities and the NBUCP, where data are analyzed and mapped. Feedback is provided annually by the NBUCP at a review meeting attended by the heads of all CDTUBs and other partners involved in BU activities in Benin. The CDTUBs perform quarterly data analyses, which they feed back to the teams in each center. Refresher workshops for the teams are conducted and new team members are trained [17]. This system allows to (1) conduct permanent active surveys for BU, (2) determine the burden of the disease, (3) provide the most adapted care for each patient. With this system in place, the number of reported BU cases increased steadily from 2003, reached a peak of 1203 cases in 2007 and decreased continuously thereafter, to 312 in 2016. The geographical distribution of BU cases in 2016 is shown in Fig. 1.

Geographical distribution of BU in Southern Benin. The map illustrates the number of reported BU cases in 2016 as well as the location of the CDTUBs in the main BU endemic region of Benin
In contrast to the decrease in the number of new BU cases reported in recent years in Benin, the percentage of patients diagnosed with WHO Category III lesions has increased (Fig. 2). Between 2007 and 2011 the number of new BU cases with Category I and II lesions detected was much higher than those with Category III lesions, whereas almost half of the newly detected BU cases between 2012 and 2016 were diagnosed with Category III lesions.

Evolution of new BU cases detected in Benin according to the WHO classification system. The percentage of patients diagnosed with Category III (red) and Category I and II (blue) lesions is shown
Therefore, the current challenge for the Ministry of Health through the NBUCP is to effectively address the issue of severe, chronic BU lesions. According to national health statistics, 267 new BU cases were detected in 2017. Of these, 46% presented with ulcers, 30% with mixed forms, 13% with plaques, and only a minority with nodules and edema. For a significant proportion of cases (23%) in 2017 BU-related disability was registered at entry.
Box 2 Cameroon
BU was first reported in Cameroon in 1969 [21]. Organized BU control in the country began 33 years later with the creation of two BU-DTCs in Ayos and Akonolinga in 2002 with the support of FAIRMED (formerly known as ALES (Aide Aux Lépreux Emmaüs-Suisse)) and MSF (Médecins Sans Frontières) Suisse, respectively. Effectiveness of BU management in these initial centers prompted the Ministry of Health in Cameroon to establish an NBUCP in 2004. Following a national BU survey in 2004, three additional BU-DTCs were created in 2006 in the three newly identified highly endemic health districts, namely Bankim, Mbonge, and Ngoantet-Mbalmayo. The initial strategy of medical teams from these BU-DTCs was to perform mass screening for BU, sensitization and awareness campaigns in communities and schools, and management of the BU cases detected. Gradually, health committees were activated in the intervention areas, and became responsible for community sensitization and awareness campaigns for BU, case-finding, and referral. Community participation in referral of suspected cases to the BU-DTCs for confirmation and treatment increased after many volunteers were trained to recognize BU in their communities. As communities became more aware of BU, active case-finding gradually gave way to passive case-finding with cases coming on their own or being referred to BU-DTCs.
In Cameroon, the WHO BU02 forms together with activity reports are sent by BU-DTCs to the NBUCP on a monthly basis. Between 2002 and 2016, 3850 BU cases were reported in the country, with a peak of 914 cases seen in 2004, explained by the national survey for BU in that year. Considerably lower numbers of cases were reported in recent years with a trough of 85 cases in 2016. Between 2002 and 2014 the number of health districts identified to be endemic for BU rose from 2 to 64 (Fig. 3). While endemic regions were mainly detected in the South and Central part of Cameroon, a national survey is required to confirm the suspected presence of BU in the northern part of the country. However, it has been shown that a reduction in program resources and activities by the major support partners over the past years has led to decreased surveillance activities, which has negatively impacted performance indicators in Cameroon [18].

Increase in the number of health districts identified to be BU endemic between 2001 and 2014 [18]
In many African BU endemic areas, government expenditure on health care is extremely low. Low per capita income and limited potential for domestic revenue mobilization hamper the ability of governments to respond effectively to national health problems, such as BU. Many NBUCPs depend strongly on external partner funding, which has decreased considerably in the past few years in some of the BU endemic countries, leading to a decrease in BU surveillance and laboratory confirmation of cases. This may in turn lead to a rise in the proportion of patients reporting with WHO Category III lesions [18]. Therefore, financing remains a key challenge for the establishment and sustainability of effective BU control programs.
2.2 Diagnosis and Treatment of BU
In addition to relatively typical ulcerative disease stages, BU may present in the form of rather unspecific, non-ulcerative nodules, edema, or plaque lesions. The clinical diagnosis of BU in Africa is complicated by many skin conditions with similar presentation ranging from cysts, lipoma, psoriasis, skin lymphomas, tropical ulcers, ulcerated skin malignancies, and venous or vascular ulcers, over bacterial skin infections such as actinomycosis, boils, cellulitis, ecthyma, folliculitis, furuncle, impetigo, noma, treponematosis, parasitic infections including cutaneous leishmaniasis and myiasis, to cutaneous tuberculosis, leprosy, and atypical mycobacteriosis [17, 22, 23]. At the level of district health facilities, microscopic detection of acid-fast bacilli (AFBs) is usually the only available laboratory diagnostic test for BU. As this method has limited sensitivity and specificity, specimens from suspected lesions are commonly collected and shipped in bulk to diagnostic reference laboratories for the detection of M. ulcerans DNA by PCR analysis, the current gold standard for the diagnosis of BU. To avoid further delay and dropout of patients, treatment of clinically suspected BU cases is often started before PCR results are reported back to the health centers.
Since 2004, WHO recommends treatment of BU with an 8-week course of daily combination antibiotic therapy consisting of oral rifampicin and injectable streptomycin [13]. However, prolonged duration of streptomycin therapy can cause persistent hearing loss and nephrotoxicity in BU patients [24]. In 2017 the WHO Technical Advisory Group on BU decided that the recommendation for treatment should be changed to oral clarithromycin and rifampicin, pending the full results of a clinical trial for the new regimen. At national level, this combination has already been introduced in several African BU endemic countries. Free provision of antibiotics to BU treatment centers is managed by the NBUCPs. However, logistics involved in the supply of the drugs to remote, rural health facilities is complicated and access to the required antibiotics is not always secured. Other direct and indirect treatment costs, such as for transport and stay at health facilities, wound management, and loss of labor of patients and caretakers have to be covered by patients and their families. The main source of funding for these costs is direct household spending, mostly through out-of-pocket payments, which may prevent patients from seeking care or may have catastrophic consequences for the household economies [25, 26]. The situation is further aggravated by the fact that many patients report with advanced stages of the disease, for which treatment is both much more demanding and more expensive. Although antibiotic treatment is effective, extensive destruction of tissue complicates healing and often leads to contractures and deformities. For such lesions, surgical debridement, skin grafting, and physical re-education may be required after antibiotic therapy. Lifelong functional limitations are a common outcome of large ulcers and are associated with loss of workforce, school abandonment [27], stigma, and social exclusion [28].
Early detection of BU, the development of an inexpensive, sensitive and specific point-of-care diagnostic test suitable for pre-treatment diagnosis, as well as the development of shorter treatment regimens suitable for decentralized care in rural endemic areas are key priorities for future efforts to improve the control of BU in Africa. For the diagnosis at field sites, the application of M. ulcerans antigen capture-based approaches are currently being evaluated [29]. Local thermotherapy of BU lesions using heat packs filled with phase change material [30] may be developed into an alternative treatment option if antibiotic treatment is not indicated, not tolerated or not readily available. Considering the continued preference of many patients to first seek care from traditional healers, sustained collaborations between community health workers, BU-DTC health staff, and traditional healers is essential for the implementation of BU control activities [10].
3 Geographical Distribution of BU: Reporting of Cases Versus Actual Situation in Africa
The geographical distribution of BU cases in Africa by country reported to WHO between 2002 and 2016 is illustrated in Fig. 4, with Côte d’Ivoire, Ghana, and Benin being the most affected.

Geographical distribution of BU in Africa by country. The map shows an accumulated number of cases reported to WHO between 2002 and 2016. Data source: WHO
These three countries were among the first with well-established BU surveillance systems [31,32,33,34], after their governments have signed the Yamoussoukro declaration on BU in 1998, an agreement to mobilize resources for the establishment of NBUCPs with technical support from WHO. In Cameroon, which is ranked fourth among the most affected countries, a wide-spread distribution of endemic regions was detected upon increased case-finding activities (Fig. 3) [18], strongly suggesting that the number of BU cases is vastly underestimated in some other BU endemic countries, where organized BU control programs have only more recently been set in place. This is for example illustrated by large series of BU patients from Nigeria, who presented to established health facilities in Benin over the past few years [35, 36], demonstrating an urgent need for the improvement of BU control activities in Nigeria [37].
Reasons for a marked reduction of new infections reported from Africa in the past few years are not entirely understood, but may at least in part be related to a decline in international support for BU control programs [18]. In Ghana, the annual BU case confirmation rates gradually decreased over the past years, from a high proportion of 76% in 2009 to a trough of only 15% in 2016. High confirmation rates in earlier years may be attributed to prior training activities on case detection and proper specimen collection provided by the NBUCP to healthcare givers within the facilities of the Ghana Health Service as well as to quarterly early case search activities conducted within the framework of the Stop BU project by researchers of the Noguchi Memorial Institute for Medical Research. The downward trend in confirmation rates may be a reflection of both an actual reduction in BU incidence and ceasing outreach activities by the NBUCP in recent years [38]. On the other hand, initiation of surveillance activities in the endemic countries may have led to the detection of many patients with long-standing infections and the current number of reported cases may reflect more the true incidence of BU. As the shedding of the bacteria from chronic BU lesions is hypothesized to fuel potential reservoirs of the pathogen, early identification and treatment of BU patients may lead to a reduction of the bacterial burden in the environment, which may in turn reduce transmission. This view is supported by the fact that no major animal reservoir has been detected to date in Africa, as opposed to BU endemic areas of southern Australia, where large numbers of possums in BU endemic settings were shown to be infected with M. ulcerans [39]. Another aspect to be considered is the potential cyclical occurrence of the disease associated with environmental or climatic factors. Also, a number of African countries, where BU cases had been detected in the past, do no longer report cases to WHO. These include countries where political instability or overburdened health systems may prevent efforts to control BU. On the other hand, also the possibility of over-reporting in areas where access to reliable laboratory confirmation is limited has to be taken into consideration, when estimating the actual burden of BU in Africa.
4 Distribution of BU Among Affected Populations in Africa
The distribution of BU within endemic countries is highly focal and local prevalence rates may vary from one village to another. Affected populations commonly live in remote, rural areas, which are sometimes largely isolated from the world around. Families typically live on subsistence-level agriculture and small-scale husbandry and obtain their water from nearby rivers or tributaries. Stagnant water bodies, which are used for washing clothes or bathing, appear to be strongly associated with the occurrence of BU [40] (Fig. 5).

Typical BU endemic settings in Africa. Left photograph: Health post in Cameroon. Right photograph: Water site in Cameroon used for doing the laundry or bathing
In many areas the emergence of BU or an increase in the incidence of BU have been ascribed to environmental disturbances such as damming of rivers, establishment of permanent wet agricultural areas like rice fields, deforestation, sand digging or mining activities with remaining water holes and seasonal ponds. For example, on the campus of the University of Ibadan, Nigeria, damming of a small stream flowing through the campus was associated with the emergence of BU among Caucasians living on site [41]. In northern Liberia, BU cases emerged when the Manor River was dammed and wetlands extended for swamp rice farming [42]. Other examples include the damming of the Mapé River in Cameroon [43], the Densu River in Ghana [44], and the Bandama River in Côte d’Ivoire [45]. Apart from man-made environmental changes, heavy rainfall may also lead to an upsurge of BU; in Uganda, an outbreak in the Busoga District was for example related to unprecedented flooding of the lakes of Uganda between 1962 and 1964 [46].
All age groups may be affected with an often equal gender distribution. However, children between five and 15 years of age are vastly overrepresented among cases in Africa, even if the age distribution of the typically very young general population is taken into account [47, 48]. In contrast, very young children seem to be underrepresented [47], and sero-epidemiological studies of populations living in BU endemic areas of Ghana and Cameroon have shown that children below the age of four years are also less exposed to M. ulcerans than older individuals [49, 50]. This suggests that exposure to M. ulcerans intensifies at an age, when children start to have more intense contact with the environment, outside their hitherto confined movement range. While the risk of developing BU seems to drop in young adults, the population age adjusted cumulative incidence of BU in the elderly was reported to be similar to that in older children [47, 48]. This may be related to immunosenescence, the gradual deterioration of the immune system associated with natural age advancement. The fact that in Japan and Australia middle-aged or elderly individuals are most commonly affected may at least in part reflect the much higher average age of the population living in the BU endemic areas.
Mounting evidence exists that infection with HIV increases the risk of BU [51]. Moreover, a number of case studies report a more aggressive progression of BU in HIV-positive individuals [52,53,54]. Although helminth infections elicit an immune response potentially enhancing susceptibility to mycobacterial diseases, no association between BU and schistosomiasis was found in one study [55]. Potential associations of BU with other co-infections prevalent in African BU endemic areas or with malnutrition have not been systematically investigated so far. Studies on a potential link between susceptibility to BU and host genetic factors are in their infancy [56, 57] and are hampered by the limited number of BU cases that can be enrolled in the studies.
5 The Etiology of BU in Africa
M. ulcerans is an acid-fast mycobacterium that has evolved from an M. marinum-like progenitor through an evolutionary bottleneck event; the acquisition of a virulence plasmid, encoding the enzymatic machinery for the synthesis of the unique macrolide toxin mycolactone [58]. Subsequent genome reduction and pseudogene development is indicative of an adaptation of M. ulcerans to a more stable ecological niche [58]. Definite identification of an environmental niche is complicated by the extraordinarily long generation time of M. ulcerans. This hampers the isolation of the bacterium from potential environmental sources, as M. ulcerans is readily overgrown by other, less fastidious organisms, including other environmental mycobacteria that are also resistant to decontamination methods developed for primary isolation [59, 60]. Considering that the occurrence of BU is commonly associated with stagnant water bodies in river basins, a habitat in aquatic ecosystems seems likely. Indeed, M. ulcerans-specific DNA sequences were detected by PCR analyses in environmental samples, such as biofilms, water, soil and plants, as well as in various aquatic animals [5]. For unclear reasons, vastly different PCR positivity rates have been reported in various studies conducted in BU endemic regions of Africa [40, 61, 62]. In contrast to endemic sites in Australia, where terrestrial mammals may be implicated as reservoirs in the disease ecology of M. ulcerans [39, 63], no similar reservoir has so far been detected in Africa [6, 64]. Therefore, it has been hypothesized that shedding bacilli from large chronic lesions of BU patients into the environment may play a role in M. ulcerans transmission in African BU endemic areas [4]. While mosquitoes have been proposed as vectors of M. ulcerans in Australia, several modes of transmission including vector-mediated, but also skin trauma-induced may be involved in African settings [5]. Direct person-to-person transmission is considered unlikely.
All M. ulcerans isolates derived from lesions of BU patients from Africa have been found to belong to the classical M. ulcerans lineage. Genetic diversity of these isolates is very low and only comparative whole genome sequencing allowed resolving the population structure and evolutionary history of African M. ulcerans disease isolates. These genome analyses have identified in many BU endemic areas, local clonal complexes of M. ulcerans that show limited diversification by the accumulation of point mutations and are associated with particular hydrological drainage areas [44, 65,66,67]. After introduction of M. ulcerans in a particular area, the local clone seems to remain isolated, which allows some point mutations to become fixed in that population. Spread of these locally confined clonal complexes between endemic areas seems to occur only rarely [68, 69], speaking against the existence of a highly mobile animal reservoir. While the dominating African M. ulcerans sublineage MU_A1 has been endemic in Africa for several hundred years, another less common and geographically more restricted African sublineage (MU_A2) has been recently identified, which seems to have been introduced into the African continent in the late nineteenth and early twentieth century [66]. Sequence analyses of the virulence plasmid pMUM encoding genes for the biosynthesis of mycolactones have shown that all mycolactone producing mycobacteria have evolved from the same progenitor which has acquired the plasmid [70]. Different M. ulcerans lineages produce different species of mycolactone; the M. ulcerans disease isolates from Africa mainly produce mycolactone A/B, the most potent form of the toxin [71, 72]. There is no doubt that the ability to produce mycolactone is critical for the evolution and persistence of M. ulcerans as a human pathogen. While the combination of cytotoxic and immunosuppressive properties of mycolactone is thought to confer a fitness advantage for M. ulcerans in mammalian hosts by preventing an immune system-mediated elimination of the bacteria, it is not yet clear how the bacteria might benefit from mycolactone production in aquatic niche environments.
6 Future Perspectives
If human BU lesions prove to be a relevant maintenance reservoir for M. ulcerans transmission, active case-finding programs, improved disease surveillance, early diagnosis, and adequate treatment may lead to a reduction in disease transmission. This hypothesis is supported by the recent decline in the number of new infections reported to WHO from many African countries and particularly from areas, where effective BU control programs have been implemented. A major challenge for the coming years will be the maintenance of established control strategies and the implementation of improved diagnostic tools and treatment approaches.
In many regions of Africa a number of tropical skin diseases, such as cutaneous leishmaniasis, leprosy, lymphatic filariasis, mycetoma, onchocerciasis, and yaws are co-endemic with BU. Screening of individuals for the presence of skin conditions in communities or schools offers the opportunity to detect these neglected diseases using a common rather than a disease-specific approach. Development of locally adapted triage criteria and diagnostic algorithms for the recognition of changes in the appearance of the skin can furthermore allow health workers at the primary health care level making appropriate decisions on either treatment or referral of patients. After specific treatment, repair of tissue damage often requires similar wound management approaches. Therefore, integrated strategies for the control and management of these diseases are now strongly promoted by the WHO Department of control of neglected tropical diseases (WHO/NTD) [73].
References
Billington WR (1970) Albert Cook 1870-1951: Uganda pioneer. Br Med J 4(5737):738–740
Clancey JK, Dodge OG, Lunn HF, Oduori ML (1961) Mycobacterial skin ulcers in Uganda. Lancet 2(7209):951–954
Clancey JK (1964) Mycobacterial skin ulcers in Uganda: description of a new Mycobacterium (Mycobacterium Buruli). J Pathol Bacteriol 88:175–187
Röltgen K, Pluschke G (2015) Epidemiology and disease burden of Buruli ulcer: a review. Res Rep Trop Med 2015(6):59–73
Merritt RW, Walker ED, Small PL, Wallace JR, Johnson PD, Benbow ME et al (2010) Ecology and transmission of Buruli ulcer disease: a systematic review. PLoS Negl Trop Dis 4(12):e911
Röltgen K, Pluschke G (2015) Mycobacterium ulcerans disease (Buruli ulcer): potential reservoirs and vectors. Curr Clin Microbiol Rep 2(1):35–43
Mulder AA, Boerma RP, Barogui Y, Zinsou C, Johnson RC, Gbovi J et al (2008) Healthcare seeking behaviour for Buruli ulcer in Benin: a model to capture therapy choice of patients and healthy community members. Trans R Soc Trop Med Hyg 102(9):912–920
Aujoulat I, Johnson C, Zinsou C, Guedenon A, Portaels F (2003) Psychosocial aspects of health seeking behaviours of patients with Buruli ulcer in southern Benin. Trop Med Int Health 8(8):750–759
Peeters Grietens K, Toomer E, Um Boock A, Hausmann-Muela S, Peeters H, Kanobana K et al (2012) What role do traditional beliefs play in treatment seeking and delay for Buruli ulcer disease?--insights from a mixed methods study in Cameroon. PLoS One 7(5):e36954
Awah PK, Boock AU, Mou F, Koin JT, Anye EM, Noumen D et al (2018) Developing a Buruli ulcer community of practice in Bankim, Cameroon: a model for Buruli ulcer outreach in Africa. PLoS Negl Trop Dis 12(3):e0006238
Renzaho AM, Woods PV, Ackumey MM, Harvey SK, Kotin J (2007) Community-based study on knowledge, attitude and practice on the mode of transmission, prevention and treatment of the Buruli ulcer in Ga West District. Ghana Trop Med Int Health 12(3):445–458
Pearson G (2018) Understanding perceptions on ‘Buruli’ in northwestern Uganda: a biosocial investigation. PLoS Negl Trop Dis 12(7):e0006689
WHO (2012) Treatment of Mycobacterium ulcerans disease (Buruli ulcer): guidance for health workers. World Health Organization, Geneva
WHO (2000) Buruli ulcer: mycobacterium ulcerans infection. World Health Organization, Geneva
Hayriye IŞik HN (2013) Health care system and health financing structure, the case of Cameroon. Int Anatol Acad Online J Health Sci 1(2):24–44
Bertrand NAS (2012) Analysis of determinants of public hospitals efficiency in Cameroon. Int J Econ Commer Res 2(2):31–65
Junghanss T, Johnson RC, Pluschke G (2014) Mycobacterium ulcerans disease. In: Farrar J, Hotez PJ, Junghanss T, Kang G, Lalloo D, White NJ (eds) Manson’s tropical diseases, 23rd edn. Saunders, Edinburgh, pp 519–531
Tabah EN, Nsagha DS, Bissek AC, Njamnshi AK, Bratschi MW, Pluschke G et al (2016) Buruli ulcer in Cameroon: the development and impact of the national control programme. PLoS Negl Trop Dis 10(1):e0004224
Muelder K (1988) Buruli ulcer in Benin. Trop Dr 18(2):53
Muelder K, Nourou A (1990) Buruli ulcer in Benin. Lancet 336(8723):1109–1111
Ravisse P (1977) Skin ulcer caused by Mycobacterium ulcerans in Cameroon. I. Clinical, epidemiological and histological study. Bull Soc Pathol Exot Fil 70(2):109–124
Bratschi MW, Njih Tabah E, Bolz M, Stucki D, Borrell S, Gagneux S et al (2012) A case of cutaneous tuberculosis in a Buruli ulcer-endemic area. PLoS Negl Trop Dis 6(8):e1751
Toutous Trellu L, Nkemenang P, Comte E, Ehounou G, Atangana P, Mboua DJ et al (2016) Differential diagnosis of skin ulcers in a Mycobacterium ulcerans endemic area: data from a prospective study in Cameroon. PLoS Negl Trop Dis 10(4):e0004385
Klis S, Stienstra Y, Phillips RO, Abass KM, Tuah W, van der Werf TS (2014) Long term streptomycin toxicity in the treatment of Buruli ulcer: follow-up of participants in the BURULICO drug trial. PLoS Negl Trop Dis 8(3):e2739
Chukwu JN, Meka AO, Nwafor CC, Oshi DC, Madichie NO, Ekeke N et al (2017) Financial burden of health care for Buruli ulcer patients in Nigeria: the patients’ perspective. Int Health 9(1):36–43
Grietens KP, Boock AU, Peeters H, Hausmann-Muela S, Toomer E, Ribera JM (2008) “It is me who endures but my family that suffers”: social isolation as a consequence of the household cost burden of Buruli ulcer free of charge hospital treatment. PLoS Negl Trop Dis 2(10):e321
Stienstra Y, van Roest MH, van Wezel MJ, Wiersma IC, Hospers IC, Dijkstra PU et al (2005) Factors associated with functional limitations and subsequent employment or schooling in Buruli ulcer patients. Tropical Med Int Health 10(12):1251–1257
Owusu AaA C (2012) The socioeconomic burden of Buruli ulcer disease in the GA West District of Ghana. Ghana J Dev Stud 9(1):5–20
Dreyer A, Roltgen K, Dangy JP, Ruf MT, Scherr N, Bolz M et al (2015) Identification of the Mycobacterium ulcerans protein MUL_3720 as a promising target for the development of a diagnostic test for Buruli ulcer. PLoS Negl Trop Dis 9(2):e0003477
Vogel M, Bayi PF, Ruf MT, Bratschi MW, Bolz M, Um Boock A et al (2016) Local heat application for the treatment of Buruli ulcer: results of a phase II open label single center non comparative clinical trial. Clin Infect Dis 62(3):342–350
Johnson RC, Sopoh GE, Barogui Y, Dossou A, Fourn L, Zohoun T (2008) Surveillance system for Buruli ulcer in Benin: results after four years. Sante 18(1):9–13
Kanga JM, Kacou ED, Kouame K, Kassi K, Kaloga M, Yao JK et al (2006) Fighting against Buruli ulcer: the Cote-d’Ivoire experience. Bull Soc Pathol Exot 99(1):34–38
Amofah G, Bonsu F, Tetteh C, Okrah J, Asamoa K, Asiedu K et al (2002) Buruli ulcer in Ghana: results of a national case search. Emerg Infect Dis 8(2):167–170
Ackumey MM, Kwakye-Maclean C, Ampadu EO, de Savigny D, Weiss MG (2011) Health services for Buruli ulcer control: lessons from a field study in Ghana. PLoS Negl Trop Dis 5(6):e1187
Marion E, Carolan K, Adeye A, Kempf M, Chauty A, Marsollier L (2015) Buruli ulcer in South Western Nigeria: a retrospective cohort study of patients treated in Benin. PLoS Negl Trop Dis 9(1):e3443
Ayelo GA, Anagonou E, Wadagni AC, Barogui YT, Dossou AD, Houezo JG et al (2018) Report of a series of 82 cases of Buruli ulcer from Nigeria treated in Benin, from 2006 to 2016. PLoS Negl Trop Dis 12(3):e0006358
Otuh PI, Soyinka FO, Ogunro BN, Akinseye V, Nwezza EE, Iseoluwa-Adelokiki AO et al (2018) Perception and incidence of Buruli ulcer in Ogun State, South West Nigeria: intensive epidemiological survey and public health intervention recommended. Pan Afr Med J 29:166
Yeboah-Manu D, Aboagye SY, Asare P, Asante-Poku A, Ampah K, Danso E et al (2018) Laboratory confirmation of Buruli ulcer cases in Ghana, 2008-2016. PLoS Negl Trop Dis 12(6):e0006560
Fyfe JA, Lavender CJ, Handasyde KA, Legione AR, O’Brien CR, Stinear TP et al (2010) A major role for mammals in the ecology of Mycobacterium ulcerans. PLoS Negl Trop Dis 4(8):e791
Bratschi MW, Ruf MT, Andreoli A, Minyem JC, Kerber S, Wantong FG et al (2014) Mycobacterium ulcerans persistence at a village water source of Buruli ulcer patients. PLoS Negl Trop Dis 8(3):e2756
Oluwasanmi JO, Itayemi SO, Alabi GO (1975) Buruli (Mycobacterial) Ulcers in Caucasians in Nigeria. Brit J Plast Surg 28(2):111–113
Monson MH, Gibson DW, Connor DH, Kappes R, Hienz HA (1984) Mycobacterium ulcerans in Liberia: a clinicopathologic study of 6 patients with Buruli ulcer. Acta Trop 41(2):165–172
Marion E, Landier J, Boisier P, Marsollier L, Fontanet A, Le Gall P et al (2011) Geographic expansion of Buruli ulcer disease. Cameroon Emerg Infect Dis 17(3):551–553
Röltgen K, Pluschke G (2010) Single nucleotide polymorphism typing of Mycobacterium ulcerans reveals focal transmission of Buruli ulcer in a highly endemic region of Ghana. PLoS Negl Trop Dis 4(7):e751
N’Krumah RTAS, Kone B, Cisse G, Tanner M, Utzinger J, Pluschke G et al (2017) Characteristics and epidemiological profile of Buruli ulcer in the district of Tiassale, south Cote d’Ivoire. Acta Trop 175:138–144
Barker DJ (1971) Buruli disease in a district of Uganda. J Trop Med Hyg 74(12):260–264
Bratschi MW, Bolz M, Minyem JC, Grize L, Wantong FG, Kerber S et al (2013) Geographic distribution, age pattern and sites of lesions in a cohort of Buruli ulcer patients from the Mape Basin of Cameroon. PLoS Negl Trop Dis 7(6):e2252
Debacker M, Aguiar J, Steunou C, Zinsou C, Meyers WM, Scott JT et al (2004) Mycobacterium ulcerans disease: role of age and gender in incidence and morbidity. Tropical Med Int Health 9(12):1297–1304
Röltgen K, Bratschi MW, Pluschke G (2014) Late onset of the serological response against the 18 kDa small heat shock protein of Mycobacterium ulcerans in children. PLoS Negl Trop Dis 8(5):e2904
Ampah KA, Nickel B, Asare P, Ross A, De-Graft D, Kerber S et al (2016) A sero-epidemiological approach to explore transmission of Mycobacterium ulcerans. PLoS Negl Trop Dis 10(1):e0004387
Johnson RC, Nackers F, Glynn JR, de Biurrun Bakedano E, Zinsou C, Aguiar J et al (2008) Association of HIV infection and Mycobacterium ulcerans disease in Benin. AIDS 22(7):901–903
Toll A, Gallardo F, Ferran M, Gilaberte M, Iglesias M, Gimeno JL et al (2005) Aggressive multifocal Buruli ulcer with associated osteomyelitis in an HIV-positive patient. Clin Exp Dermatol 30(6):649–651
Kibadi K, Colebunders R, Muyembe-Tamfum JJ, Meyers WM, Portaels F (2010) Buruli ulcer lesions in HIV-positive patient. Emerg Infect Dis 16(4):738–739
Komenan K, Elidje EJ, Ildevert GP, Yao KI, Kanga K, Kouame KA et al (2013) Multifocal Buruli Ulcer associated with secondary infection in HIV positive patient. Case Rep Med 2013:348628
Stienstra Y, van der Werf TS, van der Graaf WT, Secor WE, Kihlstrom SL, Dobos KM et al (2004) Buruli ulcer and schistosomiasis: no association found. Am J Trop Med Hyg 71(3):318–321
Capela C, Dossou AD, Silva-Gomes R, Sopoh GE, Makoutode M, Menino JF et al (2016) Genetic variation in autophagy-related genes influences the risk and phenotype of Buruli ulcer. PLoS Negl Trop Dis 10(4):e0004671
Bibert S, Bratschi MW, Aboagye SY, Collinet E, Scherr N, Yeboah-Manu D et al (2017) Susceptibility to Mycobacterium ulcerans disease (Buruli ulcer) is associated with IFNG and iNOS gene polymorphisms. Front Microbiol 8:1903
Stinear TP, Seemann T, Pidot S, Frigui W, Reysset G, Garnier T et al (2007) Reductive evolution and niche adaptation inferred from the genome of Mycobacterium ulcerans, the causative agent of Buruli ulcer. Genome Res 17(2):192–200
Yeboah-Manu D, Bodmer T, Mensah-Quainoo E, Owusu S, Ofori-Adjei D, Pluschke G (2004) Evaluation of decontamination methods and growth media for primary isolation of Mycobacterium ulcerans from surgical specimens. J Clin Microbiol 42(12):5875–5876
Yeboah-Manu D, Danso E, Ampah K, Asante-Poku A, Nakobu Z, Pluschke G (2011) Isolation of Mycobacterium ulcerans from swab and fine-needle-aspiration specimens. J Clin Microbiol 49(5):1997–1999
Williamson HR, Benbow ME, Campbell LP, Johnson CR, Sopoh G, Barogui Y et al (2012) Detection of Mycobacterium ulcerans in the environment predicts prevalence of Buruli ulcer in Benin. PLoS Negl Trop Dis 6(1):e1506
Vandelannoote K, Durnez L, Amissah D, Gryseels S, Dodoo A, Yeboah S et al (2010) Application of real-time PCR in Ghana, a Buruli ulcer-endemic country, confirms the presence of Mycobacterium ulcerans in the environment. FEMS Microbiol Lett 304(2):191–194
Roltgen K, Pluschke G, Johnson PDR, Fyfe J (2017) Mycobacterium ulcerans DNA in bandicoot excreta in Buruli ulcer-endemic area, Northern Queensland. Aust Emerg Infect Dis 23(12):2042–2045
Durnez L, Suykerbuyk P, Nicolas V, Barriere P, Verheyen E, Johnson CR et al (2010) Terrestrial small mammals as reservoirs of Mycobacterium ulcerans in benin. Appl Environ Microbiol 76(13):4574–4577
Vandelannoote K, Jordaens K, Bomans P, Leirs H, Durnez L, Affolabi D et al (2014) Insertion sequence element single nucleotide polymorphism typing provides insights into the population structure and evolution of Mycobacterium ulcerans across Africa. Appl Environ Microbiol 80(3):1197–1209
Vandelannoote K, Meehan CJ, Eddyani M, Affolabi D, Phanzu DM, Eyangoh S et al (2017) Multiple introductions and recent spread of the emerging human pathogen Mycobacterium ulcerans across Africa. Genome Biol Evol 9(3):414–426
Bolz M, Bratschi MW, Kerber S, Minyem JC, Um Boock A, Vogel M et al (2015) Locally confined clonal complexes of mycobacterium ulcerans in two Buruli ulcer endemic regions of Cameroon. PLoS Negl Trop Dis 9(6):e0003802
Ablordey AS, Vandelannoote K, Frimpong IA, Ahortor EK, Amissah NA, Eddyani M et al (2015) Whole genome comparisons suggest random distribution of Mycobacterium ulcerans genotypes in a Buruli ulcer endemic region of Ghana. PLoS Negl Trop Dis 9(3):e0003681
Lamelas A, Ampah KA, Aboagye S, Kerber S, Danso E, Asante-Poku A et al (2016) Spatiotemporal co-existence of two Mycobacterium ulcerans clonal complexes in the Offin River Valley of Ghana. PLoS Negl Trop Dis 10(7):e0004856
Doig KD, Holt KE, Fyfe JA, Lavender CJ, Eddyani M, Portaels F et al (2012) On the origin of Mycobacterium ulcerans, the causative agent of Buruli ulcer. BMC Genomics 13:258
Mve-Obiang A, Lee RE, Portaels F, Small PL (2003) Heterogeneity of mycolactones produced by clinical isolates of Mycobacterium ulcerans: implications for virulence. Infect Immun 71(2):774–783
Scherr N, Gersbach P, Dangy JP, Bomio C, Li J, Altmann KH et al (2013) Structure-activity relationship studies on the macrolide exotoxin mycolactone of Mycobacterium ulcerans. PLoS Negl Trop Dis 7(3):e2143
Mitja O, Marks M, Bertran L, Kollie K, Argaw D, Fahal AH et al (2017) Integrated control and management of neglected tropical skin diseases. PLoS Negl Trop Dis 11(1):e0005136
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2019 The Author(s)
About this chapter

Cite this chapter
Tabah, E.N., Johnson, C.R., Degnonvi, H., Pluschke, G., Röltgen, K. (2019). Buruli Ulcer in Africa. In: Pluschke, G., Röltgen, K. (eds) Buruli Ulcer. Springer, Cham. https://doi.org/10.1007/978-3-030-11114-4_2
Download citation
DOI: https://doi.org/10.1007/978-3-030-11114-4_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-11113-7
Online ISBN: 978-3-030-11114-4
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)