
Abstract
Eosinophilic pneumonia may manifest as chronic or transient infiltrates with mild symptoms, chronic idiopathic eosinophilic pneumonia, or the frequently severe acute eosinophilic pneumonia that may be secondary to a variety of causes (drug intake, new onset of tobacco smoking, infection) and that may necessitate mechanical ventilation. When present, blood eosinophilia greater than 1 × 109 eosinophils/L (and preferably greater than 1.5 × 109/L) is of considerable help for suggesting the diagnosis, however it may be absent, as in the early phase of idiopathic acute eosinophilic pneumonia or when patients are already taking corticosteroids. On bronchoalveolar lavage, high eosinophilia (>25 %, and preferably >40 % of differential cell count) is considered diagnostic of eosinophilic pneumonia in a compatible setting, obviating the need of video-assisted thoracic surgical lung biopsy, which is now performed only on very rare occasions with inconsistency between clinical, biological, and imaging features. Inquiry as to drug intake must be meticulous (www.pneumotox.com) and any suspected drug should be withdrawn. Laboratory investigations for parasitic causes must take into account the travel history or residence and the epidemiology of parasites. In patients with associated extrathoracic manifestations, the diagnosis of eosinophilic granulomatosis with polyangiitis or of the hypereosinophilic syndromes should be raised. Presence of airflow obstruction can be found in hypereosinophilic asthma, allergic bronchopulmonary aspergillosis, idiopathic chronic eosinophilic pneumonia, eosinophilic granulomatosis with polyangiitis, or in the recently identified syndrome of hyperosinophilic obliterative bronchiolitis. Corticosteroids remain the cornerstone of symptomatic treatment for eosinophilic pneumonias, with a generally dramatic response. Relapses are common when tapering the doses or after stopping treatment especially in idiopathic chronic eosinophilic pneumonia. Cyclophosphamide is necessary only in patients with eosinophilic granulomatosis with polyangiitis and poor-prognostic factors. Imatinib is very effective in the treatment of the myeloproliferative variant of hypereosinophilic syndromes. Anti-interleukin-5 monoclonal antibodies are promising in the spectrum of eosinophilic disorders.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Eosinophilic pneumonia
- aspergillosis
- Tropical eosinophilia
- Eosinophilic granulomatosis with polyangiitis
- Churg-Strauss syndrome
- hypereosinophilic syndrome
Introduction
The eosinophilic lung diseases (Table 15.1) are characterized by the presence and presumed pathogenetic role of eosinophils in the lesional processes. Eosinophilic pneumonias are defined by a prominent infiltration of the lung parenchyma by eosinophils. The other eosinophilic lung diseases, mainly hypereosinophilic asthma (not discussed in this chapter), allergic bronchopulmonary aspergillosis, and the recently individualized hypereosinophilic obliterative bronchiolitis, mainly involve the airways.
Eosinophil Biology
Initially thought to be especially important in the defence against parasitic infestation, eosinophil leukocytes are now considered multifunctional cells implicated in innate and adaptive immunity, including but not restricted to numerous inflammatory reactions to parasitic helminth, bacterial, and viral infections [1]. Their broad role in homeostasis function, physiology, and pathophysiology is now well appreciated.
Eosinophil precursors differentiate and mature in the bone marrow under the action of cytokines and especially of interleukin (IL)-5, IL-3, and granulocyte-macrophage colony-stimulating factor (GM-CSF) [1, 2]. Activation of the Δdbl-GATA-1 transcription factor is deemed critical in this process. Mature eosinophils then circulate in the blood for about 1 day before being attracted into tissues, successively involving chemotaxis, adhesion, and diapedesis and processes, under the control of IL-5 and eotaxin-1. In the tissues, they undergo apoptosis unless survival factors (mostly IL-5) are present.
The eosinophil contains two types of intracytoplasmic granules, the content of which can be released by degranulation, while other mediators are secreted (with involvement of vesicle-associated membrane proteins in the regulation of granule fusion within the cell). The larger granules, identified by a dense crystalloid matrix at electron microscopy, contain the characteristic cationic proteins major basic protein (MBP), eosinophil cationic protein (ECP), eosinophil-derived neurotoxin (EDN), and the enzymatic protein eosinophil peroxidase (EPO) [1, 2]. The smaller amorphous granules contain arylsulfatase and acid phosphatase. The process of degranulation by activated eosinophil releases cationic proteins into the extracellular space, with potential direct toxicity to the heart, brain, and bronchial epithelium. Degranulated eosinophils can be identified at electron microscopy by presence of cytoplasmic vacuoles, and loss of electron density of the central core of the granules (inversion or disappearance of core density). Molecular and intracellular pathways regulating eosinophil differentiation, priming, activation, degranulation, and mediator secretion, and how the release of toxic substances contributes to the pathophysiology of eosinophilic disorders, have become better understood on a molecular standpoint and are reviewed elsewhere [2]. In addition to cationic proteins, eosinophils release proinflammatory cytokines, lipid- and arachidonic acid–derived mediators, enzymes, reactive oxygen species, and matrix metalloproteases, all of which may contribute to the pathophysiology of eosinophilic lung diseases.
The eosinophil is involved in many allergic or inflammatory processes through its interaction with other cells, including especially T helper (Th) lymphocytes, but also mast cells and basophils, endothelial cells, macrophages, platelets, and fibroblasts. Intercellular signaling is mediated by surface expression of adhesion molecules, apoptotic signaling molecules, chemokines, complement receptors, chemotactic factor receptors, cytokine receptors, and immunoglobulin receptors. For instance, eosinophils are capable of regulating mast cell function and histamine release. Eosinophils have further immune properties. They express the major histocompatibility complex II protein human leukocyte antigen (HLA)–DR, can present the antigen to T-helper lymphocytes, and secrete an array of cytokines, thereby promoting effector T-cell proliferation. They can synthetise IL-4 and promote IL-4, IL-5, and IL-13 secretion by CD4+ T cells (promoting Th2 lymphocyte activation), and secrete indoleamine 2,3-dioxygenase (indirectly promoting Th1 apoptosis), modulating the Th1/Th2 balance. Abnormalities in the T-cell receptor repertoire and T-cell clonotype of BAL lymphocytes and peripheral blood lymphocytes seem to contribute to the pathophysiology of eosinophilic lung diseases [3]. Overall, the paradigm of eosinophil function has changed from a terminal effector cell in allergic airway diseases to their being involved in the initial stages of pathophysiology.
Corticosteroids shorten eosinophil survival in the blood and tissues, and are currently the most potent drugs to treat eosinophilic disorders, although lack of specificity can result in numerous adverse events. As the recruitment of eosinophils to the lung mostly implicates IL-5 and the eotaxin subfamily of chemokines (itself regulated by the Th2 cell–derived IL-13 cytokine), those are the target of several drugs in development, which can potentially change dramatically the therapeutic landscape of eosinophilic disorders in the near future [4]. Other promising targets for therapy include the IL-5 receptor, CD2 binding protein, IgE, and IL-4/IL-13 receptor, with a few agents already at the stage of clinical evaluation. Although histopathologic lesions in eosinophilic pneumonias are largely reversible, tissue damage can occur especially in allergic bronchopulmonary aspergillosis (ABPA), and in eosinophilic granulomatosis with polyangiitis (EGPA) (Churg-Strauss syndrome, CSS), with possible remodeling and fibrosis in the bronchial mucosa. It is unknown yet whether anti-IL-5 antibodies and other therapeutic agents that target eosinophil-specific molecules, may prevent tissue damage. In addition, newer drugs specifically targeting cytokines of the eosinophil lineage contribute to a better understanding of the pathogenic role of eosinophils [4].
General Features of Eosinophilic Pneumonias
Historical Perspective
Early descriptions of pulmonary “infiltration with eosinophilia” [5], of “pulmonary eosinophilia” [6], and later of “cryptogenic pulmonary eosinophilias” [7] included cases now considered as probable idiopathic chronic eosinophilic pneumonia (ICEP), EGPA, and Löffler’s syndrome. Carrington and colleagues [8] described in 1969 the syndrome of ICEP.
Clinical Presentation
Eosinophilic pneumonia is a pneumonia where the eosinophils are the most prominent inflammatory cells on histopathologic examination, whereas infiltration with lymphocytes and neutrophils is moderate. Eosinophilic pneumonias are separated into two main etiologic categories: (1) those with a definite cause; and (2) idiopathic eosinophilic pneumonias, either solitary or associated with extrathoracic manifestations that are the hallmark of EGPA, but can also be observed, to a lesser extent, in hypereosinophilic syndromes (HES), drug reactions, or infections especially parasitic infections. It is therefore mandatory that the clinician take a full history and search thoroughly for a cause with potentially practical consequences, such as parasitic infection or drug or toxic exposure.
Most eosinophilic pneumonias can be classified within one of the well-characterized and individualized syndromes. They may manifest by different clinicoradiologic syndromes, namely Löffler’s syndrome, chronic eosinophilic pneumonia, or acute eosinophilic pneumonia, mostly differing from one another by the pattern of disease onset, severity, and evolution with or without corticosteroid treatment. The vast majority of cases of eosinophilic pneumonia respond dramatically to corticosteroid treatment and heal without significant sequelae.
Pathology
Open lung biopsies that used to be performed for the diagnosis of ICEP have provided material for the few histopathologic studies published on eosinophilic pneumonia [7–9]. The pathologic features described in ICEP represent a common denominator of all categories of eosinophilic pneumonias, whatever their origin. Additional specific features may be observed depending on the etiological context (e.g. bronchocentric distribution of lesions in ABPA; presence of parasites or fungal hyphae in eosinophilic pneumonia of parasitic origin).
In ICEP, the alveolar spaces are filled with eosinophils representing the predominant inflammatory cell, together with a proteinaceous and fibrinous exudate, respecting the global architecture of the lung. The distribution of eosinophilic pneumonia is generally diffuse. Macrophages are also present in the infiltrate, with scattered multinucleated giant cells occasionally containing eosinophilic granules or Charcot-Leyden crystals [8]. An associated interstitial inflammatory cellular infiltrate is invariably present, consisting of eosinophils, lymphocytes, plasma cells, and histiocytes. Some eosinophilic microabscesses may be observed (foci of necrotic intra-alveolar eosinophils surrounded by macrophages or epithelioid cells with palisading arrangement). Degranulated eosinophils can be identified within the site of eosinophilic pneumonia by electron microscopic or immunohistochemical studies [10]. Areas of non-prominent organization of the alveolar inflammatory exudate are common [8]. Mucus plugs obstructing the small airways may be present in ICEP [8] and especially in ABPA. A mild non-necrotizing vasculitis involving both small arteries and venules is common, however necrosis and fibrosis are absent.
In idiopathic acute eosinophilic pneumonia (IAEP), the pathologic pattern includes intra-alveolar and interstitial eosinophilic infiltrates, diffuse alveolar damage, intra-alveolar fibrinous exudates, organizing pneumonia, and non-necrotizing vasculitis [11].
Diagnosis
The clinical diagnosis of eosinophilic pneumonia is suspected in patients with respiratory symptoms (dyspnea, cough, or wheezing), pulmonary opacities at chest imaging, and eosinophilia demonstrated in the peripheral blood or (preferably) in the lung.
Surgical or video-assisted thoracoscopic lung biopsy is seldom necessary. Although they can show characteristic features of eosinophilic pneumonia, transbronchial lung biopsies are generally not recommended due to the small size of the specimen that allows only partial morphologic evaluation. Bronchoalveolar lavage (BAL) is now considered a good surrogate of lung biopsy to demonstrate lung eosinophilia, although no study has definitely established a correlation between increased eosinophils at differential cell count and eosinophilic pneumonia at lung pathology. In normal subjects, BAL eosinophilia is lower than 1 % of cells at differential count. In contrast, BAL eosinophilia greater than 40 % is found mainly in patients with chronic eosinophilic pneumonia, whereas BAL eosinophilia between 3 and 40 % (and especially between 3 and 9 %) may be found in various interstitial lung diseases other than eosinophilic pneumonia. A conservative cutoff of 40 % of eosinophils at BAL differential cell count has been adopted for the diagnosis of ICEP in clinical studies [12, 13], and a cutoff of 25 % has been proposed for the diagnosis of IAEP [14]. We recommend that a clinical diagnosis of eosinophilic pneumonia be supported by alveolar eosinophilia when the eosinophils (1) are the predominant cell population of BAL cell count (macrophages excepted) and (2) represent more than 25 % of differential cell count (with greater specificity when greater than 40 %).
Blood eosinophilia or hypereosinophilia when present also contributes to the diagnosis of eosinophilic pneumonia in a patient with compatible HRCT features. It may be missing in patients who have already received systemic corticosteroids, and it is often absent at presentation in IAEP. Blood cell count must thus be done before starting corticosteroids. Blood eosinophilia is defined by an eosinophil blood count greater than 0.5 × 109/L, and hypereosinophilia by an eosinophil blood count greater than 1.5 × 109/L on two examinations at least 1 month interval, and/or tissue hypereosinophilia [15]. Blood eosinophilia greater than 1 × 109/L (and preferably hypereosinophilia) may obviate the need to perform BAL in individual cases with typical presentation. For example, BAL may occasionally be omitted to confirm Löffler’s syndrome (as it occurs in ascariasis) in a patient with mild cough, wheezes, transient pulmonary opacities at chest radiograph, and frank blood eosinophilia. However BAL is generally useful to rule out alternative diagnoses (such as bacterial or parasitic pneumonia, or pulmonary infiltrates related to Hodgkin disease), and BAL is recommended to confirm the diagnosis of eosinophilic pneumonia in most cases.
Eosinophilic Lung Disease of Undetermined Cause
ICEP is characterized by a progressive onset of symptoms over a few weeks with cough, increasing dyspnea, malaise, and weight loss, whereas IAEP presents as an acute pneumonia (similar to acute lung injury or acute respiratory distress syndrome [ARDS]) with frequent respiratory failure necessitating mechanical ventilation. Both conditions are idiopathic.
Idiopathic Chronic Eosinophilic Pneumonia
Chronic eosinophilic pneumonia was first described in detail by Carrington and colleagues [8], in a series of nine patients, and was further confirmed and detailed by several and numerous case reports.
Clinical Features
ICEP predominantes in women with a 2:1 female-to-male ratio [9, 13], with a peak of incidence in the fourth decade [9], and a mean age of 45 years at diagnosis [13]. A majority of patients with ICEP are nonsmokers [9, 13], suggesting that smoking might be protective. About half of the patients have a history of atopy [9, 13] and up to two thirds have a history of asthma [9, 12, 13, 16, 17], with no particularities in the clinical presentation of ICEP with the exception of higher total immunoglobulin (Ig) E levels in asthmatics [12]. In addition, asthma may develop concomitantly with the diagnosis of ICEP (15 % of patients) or develop after ICEP (about 15 % of patients) [12]. Asthma in patients with ICEP often gets worse and requires long-term oral corticosteroid treatment [12].
ICEP is characterized by the progressive onset of cough, dyspnea, and chest pain [9, 13], with a mean interval between the onset of symptoms and the diagnosis of 4 months [13]. Mechanical ventilation may be required on exceptional occasion. Hemoptysis is rare but can occur in up to 10 % of cases [9, 13]. Chronic rhinitis or sinusitis symptoms are present in about 20 % of patients [13]. At lung auscultation, wheezes are found in one third of patients [9] and crackles in 38 % [13]. Systemic symptoms and signs are often prominent, with fever, weight loss (>10 kg in about 10 %), and commonly asthenia, malaise, fatigue, anorexia, weakness, and night sweats.
Imaging
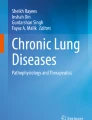
The imaging features of ICEP are characteristic, although they may overlap with those found in cryptogenic organizing pneumonia. Peripheral opacities at chest x-ray present in almost all cases [8, 9, 13, 18, 19] consist of alveolar opacities with ill-defined margins, with a density varying from ground-glass to consolidation (Fig. 15.1), and are migratory in 25 % of patients [13]. The classic pattern of “photographic negative or reversal of the shadows usually seen in pulmonary edema,” highly evocative of ICEP, is seen in only one fourth of patients [9], however peripheral and upper zone predominance of abnormalities is usually present.

Chest radiograph of a patient with idiopathic chronic eosinophilic pneumonia showing peripheral alveolar opacities predominating in the right upper lobe
Whereas the opacities are bilateral in at least 50 % of cases at chest x-ray [9], the proportion of bilateral opacities increases up to more than 95 % at high-resolution computed tomography (HRCT) [13] (Fig. 15.2). Predominance of ground-glass attenuation and consolidation in the periphery and upper lobes of the both lungs [9, 13] is very suggestive of ICEP [13, 19, 20]. Septal line thickening is common [20]. Centrilobular nodules (less than 20 % of cases) [19], consolidation with segmental or lobar atelectasis, can also be seen. Upon corticosteroid treatment, consolidation rapidly decreases in extent and density, possibly evolving to ground-glass attenuation or inhomogeneous opacities, and later to streaky or bandlike opacities parallel to the chest wall. Cavitary lesions are extremely rare and should lead to reconsideration of the diagnosis. Reverse halo sign that is very suggestive of organizing pneumonia is rare contrary in ICEP. Pleural effusions (which are common in IAEP) are rare and usually mild or moderate in ICEP. Mediastinal lymph node enlargement may be seen in 15–20 % of cases [13].

Computed tomography (CT) scan of a patient with idiopathic chronic eosinophilic pneumonia showing bilateral asymmetric peripheral alveolar opacities with airspace consolidation and ground glass opacity
Laboratory Studies
Peripheral blood eosinophilia is a diagnostic criterion of ICEP, and therefore the proportion of patients with ICEP and possible normal peripheral blood count is unknown. The mean blood eosinophilia was 5.5 × 109/L in our series [13]. Eosinophils represent 26–32 % of the total blood leukocyte count [9, 13]. C-reactive protein level is elevated [9, 13]. Total blood IgE level is increased in about half of cases and greater than 1,000 kU/L in 15 % [13]. Antinuclear antibodies may occasionally be present [13]. Urinary EDN level indicating active eosinophil degranulation is markedly increased [21].
Bronchoalveolar Lavage
BAL eosinophilia is constant and key to the diagnosis of ICEP, obviating the need for lung biopsy in the vast majority of cases (Table 15.2). The mean eosinophil percentage at BAL differential cell count was 58 % at diagnosis in the series from our group [13], however the eosinophil count drops within a few days upon corticosteroid treatment. The percentage of neutrophils, mast cells, and lymphocytes a BAL may also be increased [13]. Sputum eosinophilia may also be present.
BAL eosinophils of patients with ICEP show features of cell activation and release eosinophil proteins, which are phagocytosed by macrophages. ECP and EDN levels are increased in the BAL fluid. Eosinophils are recruited to the lung through various chemokines, and are resistant to Fas-induced apoptosis. Eosinophilic activation may be compartmentalized to the lung, as expressed by differential expression of HLA-DR molecules between alveolar and blood eosinophils. BAL lymphocytes include CD4+ memory T-cells (expressing CD45RO+, CD45RA−, CD62L−), and may present clonal rearrangement of the T-cell receptor repertoire [3].
Differential Diagnosis
Extrapulmonary manifestations when present should challenge the diagnosis of ICEP and especially to consider EGPA or overlap between ICEP and EGPA. Arthralgias, repolarization (ST-T) abnormalities on the electrocardiogram, pericarditis, altered liver biologic tests, eosinophilic lesions at liver biopsy, mononeuritis multiplex, diarrhea, skin nodules, immune complex vasculitis in the skin, and eosinophilic enteritis have been occasionally reported in ICEP [8, 13]. Furthermore, eosinophilic pneumonia may be a presenting feature of EGPA; corticosteroid treatment prescribed for ICEP may prevent the subsequent development of overt systemic vasculitis.
Lung Function Tests
An obstructive ventilatory defect is present in about half the patients [9, 13], and a restrictive ventilatory defect in the other half [13]. The CO transfer factor is decreased in half of patients, and the transfer coefficient in about one fourth. Hypoxemia (PaO2 <75 mmHg) present in two thirds of patients [13] may be due to right-to-left shunting in consolidated areas of the lung, as suggested by increased alveolar-arterial oxygen gradient [9]. With treatment, the lung function tests rapidly return to normal in most patients [9]. However, a ventilatory obstructive defect may develop over years in some patients, especially those with a markedly increased BAL eosinophilia at initial evaluation [22].
Treatment and Prognosis
Because most patients receive corticosteroids, the natural course of untreated ICEP is not well known [9]. However, spontaneous resolution of ICEP may occur [9, 13]. The clinical and radiologic response to corticosteroids is dramatic, with improvement of symptoms within 1 or 2 weeks and even within 48 h in about 80 % [13] of cases, and rapid clearance of pulmonary opacities at chest x-ray. In one series, the chest radiograph was significantly improved at 1 week in 70 % of patients, and almost all had a normal chest x-ray at their last follow-up visit [13]. Death directly resulting from ICEP is exceedingly rare.
The optimal dose of corticosteroids is not established, but treatment may be initiated with 0.5 mg/kg/day of prednisone, with slow tapering over 6–12 months based on clinical evaluation and blood eosinophil cell count. Most patients require treatment for longer than 6–12 months because of relapse in more than half of patients while decreasing below a daily dose of 10–15 mg/day of prednisone, or after stopping oral corticosteroids treatment [9, 13]. Relapses respond very well to corticosteroid treatment, that usually can be resumed at a dose of about 20 mg/day of prednisone [13].
The clinical series in which long-term follow-up is available clearly show that most patients need very prolonged corticosteroid treatment: in a series with a mean follow-up of 6.2 years, only 31 % were weaned at the last control visit [13]. Relapses of ICEP must be distinguished from asthma symptoms, and are less frequent in asthmatics, possibly because of inhaled corticosteroids prescribed after stopping oral corticosteroids [12, 13]. Inhaled corticosteroids might thus help in reducing the maintenance dose of oral corticosteroids, although they are not effective enough when given as monotherapy [23]. Long-term steroid use may lead to osteoporosis. Omalizumab, a recombinant humanized monoclonal antibody against IgE, was reported to prevent recurrence of ICEP and to spare oral corticosteroids in case reports, however caution must be exerted given recent reports of omalizumab-associated EGPA [24, 25]. The anti-IL-5 monoclonal antibody mepolizumab has not yet been evaluated in patients with ICEP.
Idiopathic Acute Eosinophilic Pneumonia
IAEP is often misdiagnosed as infectious pneumonia because of fever and bilateral opacities on chest x-ray present in all patients. However, IAEP [11, 14, 17, 26–29] markedly differs from ICEP by its acute onset, the severity of hypoxemia, the usual lack of increased blood eosinophils at presentation contrasting with highly increased eosinophil percentage at BAL, and the absence of relapse after clinical recovery. As AEP can also be due to drug exposure or infection, known causes of acute eosinophilic lung disease must be excluded for the diagnosis of IAEP to be made (Table 15.3).
Clinical Features
IAEP may present at any age [30], however the mean age at presentation is around 30 years [14, 30], with a very strong predominance in males [29]. Most patients have no prior asthma history [17]. However, taking a thorough exposure history is mandatory, as a causative role of cigarette smoke is established. Most patients have been recently exposed to dust or cigarette smoke within the days before onset of disease, and often will have begun to smoke, restarted to smoke, or increased the number of cigarettes smoked daily, especially within 1 month before the onset of “idiopathic” AEP [29, 31]. The disease is therefore often not “idiopathic”, being initiated or triggered by inhaled nonspecific causative agents in susceptible individuals, however it can occur in the absence of any inhaled exogenous trigger. AEP may develop soon after the initiation of smoking especially when starting with large quantities, and may relapse – not always – in patients who resume cigarette smoking [29, 31]. Flavoring components of smoked cigars have been suspected. In addition, the onset of IAEP seem to follow in some patients outdoor activities or peculiar exposures, such as cave exploration, plant repotting, wood pile moving, smokehouse cleaning, motocross racing in dusty conditions, indoor renovation work, gasoline tank cleaning, explosion of a tear gas bomb, or exposure to World Trade Center dust [14, 30, 32].
IAEP develops acutely or subacutely over less than 1 month in previously healthy individuals, with cough, dyspnea, fever, and chest pain at presentation [11, 30]. More than half of patients present with acute respiratory failure [29]. Abdominal complaints and also myalgias can occur [14]. Clinical signs include crackles or, less often, wheezes, and tachypnea and tachycardia.
Imaging
Imaging of patients with IAEP is quite distinct from those with ICEP. In addition to bilateral alveolar and/or interstitial opacities (Fig. 15.3) [14, 27, 28, 30], the chest x-ray commonly shows bilateral pleural effusion and Kerley B lines [14]. The chest x-ray returns to normal within 3 weeks [14, 30], with pleural effusions being the last abnormality to disappear [14]. Typical computed tomography (CT) abnormalities include ground-glass attenuation and air space consolidation (Fig. 15.4), with poorly defined nodules. Interlobular septal thickening and bilateral pleural effusion seen in a majority of patients are highly suggestive of the diagnosis in the setting of eosinophilic pneumonia [14, 18, 27, 30, 33] (or in a patient spuriously suspected to have infectious pneumonia).

Chest radiograph of a patient with idiopathic acute eosinophilic pneumonia and acute respiratory failure showing diffuse alveolar consolidation

CT scan of a patient with idiopathic acute eosinophilic pneumonia showing bilateral diffuse alveolar consolidation with air bronchogram and ground-glass opacity (a, parenchymal window) and bilateral mild pleural effusion (b, mediastinal window)
Laboratory Studies
In contrast with ICEP, peripheral blood eosinophilia is usually lacking at presentation, with white blood cell count showing increased leukocyte count with a predominance of neutrophils. However, the eosinophil count often rises within days during the course of disease [14, 17, 30], a retrospective finding very suggestive of IAEP. Eosinophilia is also present at pleural fluid differential cell count [14] and in the sputum [17]. The IgE level may be elevated. Serum levels of thymus and activation-regulated chemokine (TARC/CCL17) (and other biomarkers including KL6 and exhaled nitric oxide) are often increased in IAEP, however lack of specificity of this finding does not rule out acute lung injury or infectious pneumonia [34, 35].
Bronchoalveolar Lavage
BAL is the key to the diagnosis of IAEP, especially in patients without blood eosinophilia at presentation. The finding of greater than 25 % eosinophils at BAL generally obviates the lung biopsy, at least in immunocompetent patients The average percentage of eosinophils at BAL differential count varies between series (37 % [14] to 54 % [30]), and lymphocyte and neutrophil counts can be moderately increased. Importantly, systematic bacterial cultures of BAL fluid are sterile, and appropriate stainings are negative, ruling out infectious agents that can cause AEP. After recovery, eosinophilia at BAL may persist for several weeks.
Lung Function Tests
Hypoxemia may be severe in patients with IAEP, a majority of whom fit the definition of ARDS of various severity (except that there is no known clinical insult identified in IAEP), e.g. acute onset of respiratory failure not fully explained by cardiac failure or fluid overload (with objective exclusion of hydrostatic edema), bilateral opacities (not fully explained by effusions, lobar/lung collapse, or nodules), and a PaO2/FiO2 [fractional inspired oxygen concentration] <300 mmHg with positive end-expiratory pressure or continuous positive expiratory pressure ≥5 cm H2O [36]. However, shock is exceptional and extrapulmonary organ failure does not occur in IAEP, in sharp contrast with IAEP.
Hypoxemia is associated with right-to-left shunting in areas with consolidation, and may be refractory to breathing 100 % oxygen in some patients [26, 30]. Alveolar-arterial oxygen gradient is increased [14]. Although mechanical ventilation was necessary in a majority of patients in earlier series [14, 30], more recent series have shown that the severity of IAEP is more varied than originally reported [29].
When performed in less severe cases, lung function tests show a mild restrictive ventilatory defect with normal forced expiratory volume in 1 s–to–forced vital capacity (FEV1/FVC) ratio and reduced transfer factor. After recovery, lung function tests are generally normal, with possible ventilatory restriction in some of them [14].
Lung Biopsy
Lung biopsy is seldom necessary when BAL demonstrates alveolar eosinophilia. In older series of patients with IAEP, lung biopsy has shown acute and organizing diffuse alveolar damage together with interstitial alveolar and bronchiolar infiltration by eosinophils, intra-alveolar eosinophils, and interstitial edema [11, 14, 37].
Treatment and Prognosis
Exclusion of possible causes of AEP, especially infections and drugs, is key to the management of patients with AEP. Recovery of IAEP can occur without corticosteroid treatment [30, 34], and therefore improvement concomitant with corticosteroid treatment is not a diagnostic criterion of IAEP. In most patients diagnosed with IAEP, a corticosteroid treatment is initiated, with initially intravenous methyl prednisolone later changed to oral prednisone or prednisolone that can be tapered over 2–4 weeks [14]. FiO2 may be decreased within a few hours of corticosteroid treatment in many patients initially requiring oxygen [14]; most patients are rapidly weaned from the ventilator. The clinical improvement begins within 3 days [29]. The chest x-ray is normalized within 1 week in 85 % of patients, but mild pulmonary infiltrates and pleural effusion may still be present at CT at 2 weeks [29]. One recent study of 137 patients suggested that a treatment duration of 2 weeks may be sufficient, with an initial daily dose of 30 mg of prednisone (or 60 mg of intravenous methylprednisolone every 6 h in patients with respiratory failure) [29]. No relapse occurs after stopping corticosteroid treatment, in contrast with ICEP (Table 15.4).
No significant clinical or imaging sequelae persist on the longer term. Mortality is rare despite the frequent initial presentation with acute respiratory failure. Identification of causative tobacco or environmental exposures is key to preventing rare recurrences, that in most cases are due to resuming of cigarette smoking after smoking cessation.
Eosinophilic Granulomatosis with Polyangiitis (Ex Churg-Strauss Syndrome)
History and Nomenclature
The first reliable case of EGPA was reported by Lamb in 1914 [38]. Churg and Strauss described in 1951 [39] the eponymous syndrome of “allergic granulomatosis, allergic angitiis, and periarteritis nodosa”, mainly from autopsied cases. In the 1992 Chapel Hill Consensus Conference on the Nomenclature of Systemic Vasculitis [40], CSS was included in the group of small vessel vasculitides. The nomenclature of the systemic vasculitides was revised in 2012 at the international Chapel Hill consensus conference [41], and the terminology of CSS was replaced by EGPA. As antineutrophil cytoplasmic antibodies (ANCA) are present in about 40 % of the cases, EGPA belongs to the pulmonary ANCA-associated vasculitides, together with microspic polyangiitis and granulomatosis with polyangiitis (Wegener’s), and together with single organ ANCA-associated vasculitis.
EGPA is defined as an eosinophil-rich and necrotizing granulomatous inflammation often involving the respiratory tract, and necrotizing vasculitis predominantly affecting small to medium vessels, and associated with asthma and eosinophilia [41]. The disease may be confined to a limited number of organs especially the upper or lower respiratory tract [41]. The terminology of EGPA underscores that it is indeed a vasculitis, although not all patients have robust criteria of documented systemic vasculitis or ANCA [42]. The current terminology and classification likely requires further refinement.
Pathology
The pathologic lesions of EGPA (CSS) observed in recent series [43, 44] only rarely comprise all the characteristic features on biopsies from organs other than the lung, which is now rarely biopsied. The diagnosis is made earlier in the course of disease, often before overt vasculitis has developed, characterized histopathologically by eosinophilic infiltration of the tissues and often perivascular eosinophils but without vasculitis. In cases with overt EGPA, typical histopathologic features include vasculitis (necrotizing or not, involving mainly the medium-sized pulmonary arteries), granulomatous eosinophilic infiltration, and extravascular granuloma with palisading histiocytes and giant cells. When present, the eosinophilic pneumonia in EGPA is similar to ICEP.
Clinical Features
EGPA is a very rare systemic disease, with no sex predominance, predominating in adults younger than 65 [45, 46], with cases occasionally reported in children and adolescents. Asthma occurs at a mean age of about 35 years [45], preceding the onset of vasculitis by 3–9 years [45, 47–49]; therefore the mean age at diagnosis of EGPA ranges from 38 to 49 years [45, 49]. The interval between asthma and the onset of vasculitis may be much longer in rare cases [47], or they may be contemporaneous [49]. Asthma is generally severe, and frequently requires oral corticosteroids; its severity typically increases progressively until the vasculitis develops, but it may attenuate when the vasculitis flourishes (possibly as a result of corticosteroids) and further increase once the vasculitis recedes [45, 47].
Chronic rhinitis (75 % of cases) [45], relapsing paranasal sinusitis (60 %) [48], and nasal polyposis with eosinophilic infiltration at histopathology are frequent. Crusty rhinitis may be present, however it is much less severe in EGPA than in granulomatosis with polyangiitis. Septal nasal perforation and saddle nose deformation are exceedingly rare.
Asthenia, weight loss, fever, arthralgias, and myalgias often herald the onset of the systemic vasculitis.
Heart damage in EGPA is undoubtedly a major source of morbidity and mortality, although its onset is often insidious and asymptomatic and diagnosed only when left ventricular failure and dilated cardiomyopathy have developed, possibly leading to cardiac failure or sudden death [45–50]. Heart involvement mostly results from eosinophilic myocarditis, and rarely from arteritis of the larger coronary arteries [51, 52]. Although marked improvement usually occurs with corticosteroid treatment, heart involvement in EGPA may require heart transplantation, with possible recurrence of eosinophilic vasculitis in the transplanted heart. A strict cardiac evaluation is therefore warranted in any patient with suspected EGPA, generally including electrocardiogram, echocardiography, serum level of troponin, and magnetic resonance imaging of the heart. Cardiac MRI frequently shows late enhancement of the myocardium [53–55], which may correspond to myocarditis, however the absence of a gold standard, it is difficult at a given point in time to differentiate irreversible scar lesions from active inflammation requiring intense immunosuppression, and incidental findings from clinically relevant myocardial involvement. Treatment decisions are eventually based on critical clinical evaluation, taking into account results from several investigations, including electrocardiogram, echocardiography, troponine level, and possibly a combination of cardiac MRI and positron emission tomography. In addition to myocardial involvement, asymptomatic pericarditis with limited effusion at echocardiography is common, with rare cases of tamponade, and the risk of venous thromboembolic events [56] is increased in patients with EGPA. Endomyocardial involvement (typically seen in idiopathic HES) is uncommon in EGPA.
Mononeuritis multiplex, present in 77 % of patients [48], is the most frequent and the most typical of peripheral neurologic involvement in EGPA, which may also consist of asymmetrical polyneuropathy in the lower extremities, or rarely cranial nerve palsies or central nervous system involvement. Digestive tract involvement (31 % of cases [48]) consists in isolated abdominal pain, and less frequently intestinal or biliary tract vasculitis, diarrhea, ulcerative colitis, gastroduodenal ulcerations, perforations (esophageal, gastric, intestinal), digestive hemorrhage, or cholecystitis. Cutaneous lesions (50 % of patients[48]) mainly consist of palpable purpura of the extremities (Fig. 15.5), subcutaneous nodules (especially of the scalp and extremities), erythematous rashes, and urticaria. Renal involvement (about 25 % of cases) consists in mild severity glomerulonephritis or glomerular hematuria [48], however renal failure is rare contrasting with the other ANCA-associated vasculitides.

Palpable purpura of the forearm in a patient with eosinophilic granulomatosis with polyangiitis
Imaging
Pulmonary opacities corresponding to eosinophilic pneumonia are present on chest x-ray in a majority of patients with EGPA (37 % [48] to 72 % [45, 57]) and consist of ill-defined opacities, sometimes migratory, transient, and of varying density [45, 47, 58, 59]. In contrast to GPA, pulmonary cavitary lesions are exceptional. The chest x-ray may remain normal throughout the course of the disease. Mild pleural effusion and phrenic nerve palsy can be observed. On thin-section CT, ground-glass attenuation and air space consolidation predominate, with peripheral or random distribution (Fig. 15.6). Bronchial wall thickening or dilation, interlobular septal thickening, hilar or mediastinal lymphadenopathy, pleural effusion, or pericardial effusion [18, 58, 59] are less commonly found. In one study, centrilobular nodules were more frequent in EGPA than in patients with ICEP [19]. However, EGPA is difficult to differentiate from other causes of eosinophilic lung diseases on the basis of HRCT imaging [18]. Importantly, pleural effusion when present may correspond to either inflammatory eosinophilic exudate directly related to EGPA or to a transudate caused by cardiomyopathy.

CT scan of a patient with eosinophilic granulomatosis with polyangiitis showing airspace consolidation and ground-glass opacity in the right lower lobe
Laboratory Studies
Peripheral blood eosinophilia is a major feature of EGPA, with generally eosinophil counts comprised between 5 and 20 × 109/L and occasionally higher values [45, 47, 48]. Blood eosinophilia usually parallels disease activity, and disappears within hours after the initiation of corticosteroid treatment. Eosinophilia, sometimes greater than 60 %, is also found on BAL differential cell count and in the pleural fluid when present.
Although EGPA belongs to the group of ANCA-associated vasculitides, ANCAs are present in only about 40 % of patients. ANCAs in EGPA are mainly perinuclear (p-ANCA) with myeloperoxidase specificity, and rarely cytoplasmic ANCAs (c-ANCA) with proteinase 3 specificity [48, 49, 60–62]. Although nonspecific and not validated as useful biomarkers, the serum IgE level, the erythrocyte sedimentation rate, and the C-reactive protein level, and serum levels of IgG4, CCL17/TARC, and CCL26/Eotaxin-3 are increased. Anemia is common. High levels of urinary EDN may represent an activity index of disease.
Pathogenesis
EGPA is considered an autoimmune process involving T cells, endothelial cells, and eosinophils. Defects have been identified in regulatory CD4+ CD25+ or CD4+ CD25− T-cell lymphocytes (producing IL-10 and IL-2) that may influence progression of disease, and supporting an immunological hypothesis of disease. Furthermore, clonal CD8+/Vβ+ T cell expansions with effector memory phenotype and expressing markers of cytotoxic activity were found in peripheral blood lymphocytes, as well as T cell receptor-beta gene rearrangement. Patients carrying the major histopathology complex DRB4 allele, involved in acquired specific immunity, are prone to develop EGPA. Familial EGPA has been reported.
Contrasting to common belief, evidence of allergy demonstrated by specific IgE together with a corresponding clinical history is present in less than one third of patients. When present in EGPA, allergy mainly consists of perennial allergies to Dermatophagoides, whereas seasonal allergies are less frequent than in the general asthmatic patient [63].
Some vaccines or desensitization may trigger or play a role as adjuvant factors [64]. Other possible triggering factors include Aspergillus, allergic bronchopulmonary candidiasis, Ascaris, bird exposure, or smoked cocaine. Some drugs have been suspected to induce EGPA, especially sulfonamides (used together with antiserum), diflunisal, macrolides, diphenylhydantoin, and more recently the anti-IgE antibody omalizumab [65]. In addition, leukotriene-receptor antagonists (montelukast, zafirlukast, pranlukast) have been suspected to be involved in the development of EGPA, although their role is controversial [49, 66–70]. The occurrence of EGPA is more frequent in patients receiving leukotriene receptor antagonists, however there is conflicting evidence whether the association is coincidental, whether some cases of smoldering EGPA flare because of reducing oral or inhaled corticosteroids, or whether these drugs really exert a direct facilitating or triggering role on the vasculitis [24, 68]. A possible mechanistic link has been proposed [71]. Since EGPA may follow montelukast treatment in asthmatic patients without smoldering EGPA, may recur on rechallenge with the drug, and may remit on its withdrawal [66, 68], a causal relationship cannot be excluded [70], and we advocate that leukotriene receptor antagonists be avoided in patients with asthma, eosinophilia, and/or established or smoldering extrapulmonary manifestations.
Diagnosis
The classical description of EGPA follows three stages: asthma and rhinitis; tissue eosinophilia (such as a pulmonary disease resembling ICEP); and extrapulmonary eosinophilic disease with vasculitis. Diagnosing EGPA may be challenging in patients with early disease corresponding to the so-called formes frustes [72], who often already receive oral corticosteroids for asthma, thereby masking the underlying smoldering vasculitis. The diagnosis is more straightforward at a later stage of disease with overt systemic manifestations, however it is extremely important that the diagnosis be established before severe organ involvement (especially cardiac) is present.
There are currently no established diagnostic criteria for EGPA. Lanham and associates [45] have proposed three diagnostic criteria including (1) asthma, (2) eosinophilia exceeding 1.5 × 109/L, and (3) systemic vasculitis of two or more extrapulmonary organs, however those do not include ANCAs, which when present do contribute to the diagnosis. Classification criteria (which are not diagnostic criteria) have been proposed by the American College of Rheumatology [73] (Table 15.5), but they cannot be readily used for diagnosis in an individual with suspected EGPA. Provisional diagnostic criteria including ANCA have been recently proposed [42]. Although a pathologic diagnosis is desirable and can be obtained from the skin, nerve, or muscle [48], it is not mandatory in patients with characteristic features of EGPA. Because cutaneous lesions are easy to access (when not involving the face), a skin biopsy is commonly performed to obtain pathologic evidence of vasculitis when they are present (See Clinical Vignette). Conversely, lung biopsy either transbronchial or video-assisted is seldom done.
Clinical Vignette
A 32-year old female, never-smoker, with a 8-year history of chronic rhinosinusitis with nasal polyposis, and asthma for the last 4 years, was admitted for acute onset of dyspnea and skin manifestations. She had no history of allergic manifestations. Severity of asthma had increased over the past year, and montelukast had been prescribed 4 months ago by her general physician in addition to her long-term treatment with inhaled long-acting corticosteroids and bronchodilators. On admission, she presented with acute exacerbation of asthma, nasal obstruction with nasal crusts, asthenia, arthralgia, palpable purpura of the lower extremities, and was further diagnosed with mononeuritis multiplex. The chest radiograph showed areas of ground glass opacity, with further patchy peripheral bilateral alveolar consolidation at chest CT. Peripheral blood eosinophils were 5.6 × 109/L. Differential cell count of bronchoalveolar lavage demonstrated 65 % eosinophils, 4 % neutrophils, 7 % lymphocytes, and 24 % macrophages. Skin biopsy showed leukocytoclastic vasculitis. Antineutrophil cytoplasmic antibodies were negative. Electrocardiogram, echocardiography, and serum troponine level were normal. Pulmonary function tests showed airflow obstruction, with marginal improvement with inhaled bronchodilators. The patient was diagnosed with eosinophilic granulomatosis with polyangiitis and was treated with oral prednisolone (1 mg/kg per day for 1 month then progressively tapered). Montelukast was discontinued. Complete remission was obtained. Three years later, the patient complains of chronic rhinosinusitis, dyspnea on exertion with nonreversible moderate airflow obstruction despite high-dose inhaled anti-asthmatic therapy and 5 mg/day of oral prednisolone. Peripheral blood eosinophils are in the normal range. There are no sequelae of systemic manifestations.
Differential Diagnosis
Differentiating EGPA from the other ANCA-associated vasculitides and the other eosinophilic syndromes can be difficult. ANCA-negative EGPA without typical polyangiitis features and “formes frustes” (often consisting of cases in which the disease has been controlled to a greater or lesser extent by corticosteroids given for asthma) may overlap with unclassified systemic eosinophilic disease especially ICEP with minor extrathoracic symptoms. ICEP may also progress to EGPA. Furthermore, pathological features of mild non-necrotizing vasculitis are common in patients with ICEP [8]. EGPA can also overlap with idiopathic HES. When present, ANCA or the finding of a vasculitis and granulomas on biopsy contribute to the diagnosis of EGPA, whereas molecular biology or c-ANCA with proteinase-3 specificity may argue in favor of a diagnosis of idiopathic HES or GPA, respectively.
In addition to contribute to the diagnosis of vasculitis, the presence (in 40 % of cases) or absence (in 60 % of the cases) of ANCAs is associated with distinct clinical phenotypes in EGPA [61, 62, 74] (Table 15.6). Patients with ANCA have a vasculitic phenotype of disease with an increased frequency of extracapillary glomerular lesions, peripheral neuropathy, purpura, and biopsy-proven vasculitis. In contrast, patients without ANCA have more frequent cardiac and pulmonary involvement (and fever), suggesting an eosinophilic tissue disease phenotype, and conceivably representing a variant of the HES with systemic manifestations [61]. Interestingly, genetic predisposition affects the phenotype of EGPA. The vasculitic phenotype of EGPA is more frequent in individuals carrying the major histopathology complex DRB4 allele, whereas the IL-10-3575/1082/592 TAC haplotype is associated with ANCA-negative EGPA phenotype.
Treatment and Prognosis
Treatment of EGPA is based on corticosteroids, which suffice in a large number of cases [45, 75–77]. In the most severe cases, treatment is initiated with methylprednisolone pulses, for 1–3 days, followed by oral corticosteroids, usually started with 1 mg/kg/day of prednisone, and continued for several months with progressive reduction of doses. Relapses are common despite corticosteroids or after treatment has been discontinued, and may consist in relapses of the systemic vasculitis (usually accompanied by increased peripheral blood eosinophilia greater than 1 × 109), or more frequently in remitting or persistent difficult asthma that may require long-term low-dose oral corticosteroids despite optimal inhaled asthma therapy.
Patients with poor prognostic factors at onset that could result in mortality or severe morbidity should receive intravenous pulses of cyclophosphamide therapy (better tolerated than oral cyclophosphamide administration) in addition to corticosteroids. Four factors have been associated with a poor prognosis in patients with EGPA in a study of patients with either polyarteritis nodosa or EGPA, namely age >65 years, cardiac symptoms based on easily detectable clinical parameters, gastrointestinal involvement, and renal insufficiency with stabilized peak creatinine >150 μmol/L, whereas ear, nose and throat symptoms were associated with a lower risk of death EGPA (“revisited five factor score”) [78]. Immunosuppressive therapy with cyclophosphamide is therefore warranted in patients with a five factor score >1 and especially those with heart failure [79, 80]. Cardiomyopathy is indeed the main predictor of mortality [74], especially in case of heart failure [79]. Disease control is improved by combination of immunosuppressors with corticosteroids, with the caveat of a higher risk of infections.
Long-term follow-up is warranted due to the risk of relapse of the vasculitis, which is not prevented by cytotoxic agents, and is higher in patients with ANCA [74] and lower in those with baseline eosinophils >3.0 × 109/L [80]. Although 12 cyclophosphamide pulses are better able to control the disease, a 6-pulses regimen is generally preferred when complete remission of the vasculitis is obtained, followed by maintenance therapy with oral azathioprine (or weekly intramuscular methotrexate) in addition to corticosteroids.
In recent series, almost 80 % of patients were alive at 5 years [49, 74, 75], and 97 % were alive at 5 years in EGPA without poor-prognosis factors [81]. Mortality is associated with disease severity. Most deaths during the first year of treatment are due to cardiac involvement [82]. Long-term morbidity is related to side effects of oral corticosteroids [81], and to frequent uncontrolled asthma with airflow obstruction (that may still be partly reversible with increased oral corticosteroid treatment [83]) despite corticosteroids and inhaled therapy [83, 84].
Some selected cases of severe EGPA refractory to corticosteroids and/or cyclophosphamide may benefit from subcutaneous interferon-alfa, high-dose intravenous immunoglobulins, cyclosporin A, or rituximab, however with low-level of evidence. In addition, the anti-IgE omalizumab has been used successfully to treat persistent asthma in patients with EGPA; careful clinical monitoring is warranted, because omalizumab does not control the systemic disease. Mepolizumab is under evaluation.
Hypereosinophilic Syndrome
The “idiopathic” HES was historically defined in 1975 by Chusid and coworkers [85] as (1) a persistent eosinophilia greater than 1.5 × 109/L for longer than 6 months, or death before 6 months associated with the signs and symptoms of hypereosinophilic disease, (2) a lack of evidence for parasitic, allergic, or other known causes of eosinophilia, and (3) presumptive signs and symptoms of organ involvement, including hepatosplenomegaly, organic heart murmur, congestive heart failure, diffuse or focal central nervous system abnormalities, pulmonary fibrosis, fever, weight loss, or anemia. As a treatment is often considered before irreversible systemic complications occur, the diagnosis of HES is now considered in patients with blood hypereosinophilia (greater than 1.5 × 109/L) on at least two occasions in the absence of other etiologies for the eosinophilia, allowing earlier diagnosis and management.
Pathogenensis
HES may result from a clonal cell proliferation, involving either the lymphocyte lineage in the “lymphocytic variant” of HES whereby clonal lymphocytes produce eosinophilopoetic chemokines, or the eosinophil cell lineage itself in chronic eosinophilic leukemia (the “myeloproliferative variant” of HES). In such cases, the HES may be considered as a premalignant T-cell disorder [86, 87] or a chronic leukemia, respectively. The term idiopathic is now restricted to cases that cannot be classified in either category, and further innovative diagnostic tools will likely contribute in the future to differentiate these cases from other causes of eosinophilia of determined cause.
In the “lymphocytic variant” of HES (about 30 % of patients with HES), chemokines (especially IL-5) produced by clonal Th2 lymphocytes bearing clonal rearrangement of the TCR with an aberrant immunologic phenotype (such as CD3− CD4+) promote the accumulation of eosinophils. Lymphocyte phenotyping by flow cytometry to detect a phenotypically aberrant T-cell subset, and analysis of the rearrangement of the TCR genes in search of T-cell clonality on the peripheral blood (and possibly bone marrow), are therefore key to the diagnosis. Demonstration of increased IL-5 expression from cultured T-cells can also contribute to the diagnosis. Papules or urticarial plaques infiltrated by lymphocytes and eosinophils (and rarely, a cutaneous T-cell lymphoma or the Sezary syndrome) are frequently present. Serum levels of IL-5, TARC, and total IgE are increased but nonspecific.
In the chronic eosinophilic leukaemia (“myeloproliferative variant” of HES) (about 20–30 % of cases), an interstitial chromosomal deletion of a region in the long arm of chromosome 4 (q12) is causing a fusion protein by fusion of FiplLl – PDGFR-α, with the constitutive activation of the tyrosine kinase domain. Patients frequently present with hepatomegaly, splenomegaly, mucosal ulcerations, severe cardiac manifestations resistant to corticosteroid treatment, anemia, thrombocytemia, increased serum vitamin B12, leukocyte alkaline phosphatase and serum tryptase, circulating leukocyte precursors, and pronounced mastocytosis (lacking KIT mutations). Cutaneous manifestations are infrequent. Because the deletion is not detectable by karyotype analysis [88, 89], an analysis of chromosomal deletion using FISH probes to the gene CHIC2 encompassed in the deleted sequence, and of the expression of the FiplLl – PDGFR-α fusion gene is required for the diagnosis. The tyrosine kinase activity of the fusion protein is inhibited by imatinib, which proved efficient in treating HES in patients refractory to corticosteroids, hydroxyurea, and/or interferon-α.
Clinical and Imaging Features
The pulmonary involvement in patients with eosinophilia of clonal origin has not been studied specifically in the two variants of the HES, and most data available derive from older studies. Lung or pleural involvement is uncommon in the lymphocytic variant of the HES [86, 87]. However, pulmonary involvement is present at chest CT in about 40 % of patients with chronic eosinophilic leukemia [85, 90].
The HES occurs much more commonly in men than in women (9:1), usually between 20 and 50 years, with insidious onset or incidental discovery of peripheral eosinophilia [90]. The mean eosinophil count at presentation was 20.1 × 109/L in one series [91],, with occasionally extremely high values in excess of 100 × 109/L [85].
Patients present with weakness and fatigue (26 %), cough (24 %), dyspnea (16 %) [90], or asthmatic symptoms (25 %) [92]. Morbidity and mortality in HES are driven by cardiovascular involvement, with characteristic endomyocardial fibrosis [90] (which differs from the eosinophilic myocarditis seen in EGPA), causing dyspnea, congestive heart failure, mitral regurgitation, cardiomegaly [90], and typical features at echocardiography [93]. The other manifestations of HES include neurologic manifestations (thromboemboli, central nervous system dysfunction, and peripheral neuropathies), cutaneous manifestations (erythematous pruritic papules and nodules, urticaria, and angioedema).
Pulmonary involvement [85, 90] may manifest as pleural effusion, pulmonary emboli, interstitial opacities at imaging, or especially cough, which can be the predominant feature, be associated with bronchospasm, and be severe, with possibly frequent coughing attacks [91]. CT findings vary and are poorly specific [18], but most commonly consist of patchy ground-glass opacities and consolidation [92]. Small nodules, focal and peripheral areas of ground-glass attenuation, and occasionally a halo of ground-glass attenuation, may be observed. Notably, imaging features corresponding to eosinophilic lung involvement must be differentiated from those related to pulmonary edema resulting from cardiac involvement.
Laboratory Studies
Blood eosinophilia is typically very high, exceeding 3–5 × 109/L, with higher values than in other eosinophilic lung diseases. Eosinophilia may be only mild at BAL, however suggesting that eosinophilia may be compartmentalized. Elevated serum levels of mast cell tryptase, and dysplastic mast cells may be present in the bone marrow, with some patients meeting minor criteria for systemic mastocytosis.
Treatment and Prognosis
In patients with chronic eosinophilic leukemia, imatinib is the first-line therapy, with more frequent response when the Fip1L1 – PDGFR-α fusion protein is present [88, 89, 94]. Long-term continuation of treatment is required in some patients to maintain remission, with possible tapering of the dose, whereas imatinib can be stopped without relapse in others [95]. In patients with the “lymphocytic variant” of HES, corticosteroids remain the mainstay of treatment, although a response is obtained in only about half of them. Mepolizumab, an anti-IL5 antibody, is beneficial as a corticosteroid-sparing agent in HES patients negative for the FiplLl – PDGFR-α fusion gene and requiring 20–60 mg/day of prednisone to maintain a stable clinical status and a blood eosinophil count of less than 1 × 109/L [96, 97]. Chemotherapeutic agents (hydroxyurea, vincristine, etoposide), cyclosporin A, and interferon-α either as monotherapy or in association with hydroxyurea, may be beneficial particularly in the myeloproliferative variant.
The long-term prognosis of HES has improved considerably, with a 3-year survival of only 12 % in the first published series [85], to about 80 % survival at 5 years and 50–70 % survival at 10 years in later series [90, 91]. Further improvement in the long-term outcome and survival with this condition can be anticipated from recent advances in gene molecular biology that rapidly translate into innovative therapies.
Idiopathic Hypereosinophilic Obliterative Bronchiolitis
Hypereosinophilic obliterative bronchiolitis is a recently individualized entity [98], currently defined by provisional working criteria (Table 15.7), associating demonstration of bronchiolitis, of peripheral blood and/or alveolar eosinophilia, and persistent airflow obstruction despite high-dose inhaled bronchodilators and corticosteroids. Demonstration of a bronchiolitis may be obtained by lung biopsy [98–100] and/or HRCT showing direct signs of bronchiolitis (e.g. centrilobular nodules and branching opacities) [98] (Fig. 15.7). Hypereosinophilic obliterative bronchiolitis can be idiopathic, but may also occur in the setting of EGPA, ABPA, drug-induced eosinophilic lung disease (such as minocycline), and possibly in severe asthma [98].

CT scan of a patient with idiopathic hypereosinophilic bronchiolitis showing bronchiectasis in the right middle lobe and mucoid impaction in the left lower lobe
Patients report cough and exercise dyspnea but generally do not present with intermittent asthma symptoms or wheezes. The blood eosinophil cell count (with a mean value of 2.7 × 109/L), and the mean eosinophil differential percentage at BAL (with a mean value of 63 %) are elevated [98]. Airflow obstruction is often severe but reversible in all cases with initiation of oral corticosteroid therapy or increasing its daily dose, however clinical and functional manifestations often recur when the daily dose of oral prednisone is tapered to less than 10–15 mg. Unrecognised untreated hypereosinophilic obliterative bronchiolitis might be a cause of irreversible airflow obstruction in chronic eosinophilic respiratory diseases. Notably, whitish tracheal and bronchial granulations or bronchial ulcerative lesions can be present with prominent eosinophilia at bronchial biopsy [98].
Eosinophilic Lung Disease of Determined Cause
Once the diagnosis of eosinophilic pneumonia has been made, a thorough evaluation is necessary to investigate possible causes. A more comprehensive description of eosinophilic pneumonia related to fungi or parasites can be found elsewhere [101].
Eosinophilic Pneumonias of Parasitic Origin [101, 102]
The most common cause of eosinophilic pneumonia in the world, eosinophilic pneumonias related to parasite infestation arises mainly in humans infected by helminths and especially nematodes (roundworms).
Tropical Eosinophilia [103]
Tropical eosinophilia caused by the filarial nematodes Wuchereria bancrofti and Brugia malayi is endemic in tropical and subtropical areas of Asia, Pacific, Africa, and less commonly in South and Central America. It has been reported mostly in Indians, and occasionally in patients originating from India or Asia and living in western countries. It is characterized by severe spasmodic bronchitis or chronic dry cough (exacerbated at night), often associated with expiratory dyspnea and wheezing, fever, loss of weight, anorexia, leukocytosis, high blood eosinophilia, and disseminated bilateral opacities at chest x-ray. Eosinophilic pneumonia is generally seen 1–3 months after infestation. Blood eosinophilia is prominent, with more than 2 × 109 eosinophils/L in all cases, and up to 60 × 109/L in some cases. BAL shows intense alveolitis with a mean percentage of 54 % of eosinophils with marked degranulation. Because the circulating microfilariae are trapped in the lung vasculature, they are usually not found in the blood or the lung. BAL eosinophils drop within 2 weeks upon anti-parasitic treatment. Lung function tests show a restrictive ventilatory defect, with a reversible obstructive ventilatory defect and hypoxemia in about a quarter of the patients. Nonspecific opacities are present on chest x-ray and CT in a majority of patients; irregular basilar opacities may persist for longer than 1 year. The diagnosis is made by the combination of cough worse at night; residence in a filarial endemic area; eosinophil count greater than 3,300 cells/mm3; and clinical and hematologic response to diethylcarbamazine. The latter is the only effective drug for tropical eosinophilia. Association of corticosteroids to diethylcarbamazine may be beneficial.
Ascaris Pneumonia
The most common helminth infecting humans, Ascaris lumbricoides is transmitted through food or water contaminated by human feces. Transient pulmonary infiltrates with blood eosinophilia (Löffler’s syndrome) may develop during the migration of the larvae of the parasite through the lung, with usually mild pulmonary symptoms (cough and wheezing), transient fever, possible pruritic eruption at the time of respiratory symptoms. Blood eosinophilia may be as high as 22 × 109/L. Symptoms spontaneously resolve in a few days, whereas blood eosinophilia may remain elevated for several weeks. The diagnosis is made by the delayed finding of the worm or ovae in the stool within 3 months of the pulmonary manifestations. Intestinal ascariasis is treated with oral mebendazole.
Eosinophilic Pneumonia in Larva Migrans Syndrome
Visceral larva migrans is caused by Toxocara canis, and occurs mainly in children infected by eggs contaminating the soil of public playgrounds in urban areas. Whereas the majority of patients remain asymptomatic and undiagnosed, some present with fever, cough, dyspnea, seizures, fatigue, wheezes or crackles at pulmonary auscultation, and pulmonary opacities at chest x-ray. Corticosteroids may be beneficial in rare severe cases in adults necessitating mechanical ventilation. Blood eosinophilia may be present initially, or may develop only in the following days. The diagnosis is difficult, as both IgG and IgM antibodies may reflect residual immunity rather than recent infection and do not have diagnostic significance [104]. Only symptomatic treatment is generally required. The use of antihelmintics is controversial. Corticosteroids seem beneficial in cases with severe pulmonary involvement.
Strongyloides stercoralis Infection
Prevalent in the tropical and subtropical areas, infection with the intestinal nematode Strongyloides stercoralis is acquired through the skin by contact with the soil of beaches or mud, and may persist for years, often without peripheral eosinophilia that is mostly present in recently infected patients. Löffler’s syndrome occurs when larvae migrate through the lungs after acute infection. Immunocompromised patients or those receiving immunosuppressive therapy are at risk of severe disseminated strongyloidiasis, which may affect all organs (hyperinfection syndrome). The diagnosis depends on the demonstration of larvae in the feces or in sputum and BAL fluid. Immuno-diagnostic assays by ELISA methods may be useful for diagnosis and screening. All infected patients should be treated using ivermectin.
Eosinophilic Pneumonias in Other Infections
Löffler’s syndrome can also be caused by the human hookworms Ancylostoma duodenale and Necator americanus. Simple pulmonary eosinophilia may be due to cutaneous helminthiasis (creeping eruption) related to the dog hookworm Ancylostoma brasiliense. Transient multiple small pulmonary nodules at chest imaging and eosinophilia may occur in early acute schistosomiasis due to Schistosoma haematobium or S. mansoni, whereas post-treatment eosinophilic pneumonitis (also called reactionary Löffler’s-like pneumonitis) may develop in chronic schistosomiasis (in addition to the risk of portopulmonary hypertension) [105]. Other parasites causing rare pulmonary manifestations with eosinophilia include the filarial parasite of dog Dirofilaria immitis (the pulmonary fluke), Paragonimus westermani, Trichomonas tenax, Capillaria aerophila, and Clonorchis sinensis.
Pulmonary infection with eosinophilia has been reported occasionally with Pneumocystis jirovecii, fungi (Coccidioides immitis, Bipolaris australiensis, Aspergillus niger and Bipolaris spicifera), bacteria (tuberculosis, brucellosis), and viruses (respiratory syncytial virus, influenza infection).
Allergic Bronchopulmonary Aspergillosis
ABPA is a distinct condition characterized by asthma, eosinophilia, and bronchopulmonary manifestations with bronchiectasis due to the fungus Aspergillus fumigatus, and differing from invasive pulmonary aspergillosis, aspergilloma, Aspergillus-associated asthma, or chronic necrotizing aspergillosis, although it may be associated to the latter. ABPA is related to a complex allergic and immune reaction to Aspergillus colonizing the airways in susceptible hosts, namely 1–2 % of adults with previous asthma and 7–10 % [106, 107] of patients with cystic fibrosis. In addition, rare cases have been recently reported in patients with chronic obstructive pulmonary disease. Five stages have been described (acute, remission, recurrent exacerbations, corticosteroid-dependent asthma, and fibrotic end stage), however not reflecting the natural course of disease in many patients, and alternative staging systems have been proposed [108]. Allergic Aspergillus sinusitis, a sinus equivalent of ABPA [109], can be associated with ABPA in a syndrome called sinobronchial allergic aspergillosis.
Pathogenesis
ABPA results from damage to the bronchial epithelium, submucosa, and adjacent pulmonary parenchyma caused by a chronic inflammatory reaction in the bronchi and the surrounding parenchyma. It is mediated by type I and type III immunologic response of the host (mediated by IgE, and IgG and IgA antibodies, respectively), together with a Th2 CD4+ T-cell mediated immune response and sustained IL-17 expression [110] to antigens from Aspergillus growing in mucous plugs in the airways. In addition to mechanisms associated with innate and acquired immunity, ABPA can occur preferentially in genetically susceptible hosts, as suggested by increased prevalence of heterozygotic cystic fibrosis transmembrane conductance regulator (CFTR) gene mutations [111, 112], and association with a polymorphism within the IL-4 receptor α-chain gene and HLA DR subtypes. Infection with nontuberculous mycobacteria [113], infliximab therapy for sarcoidosis [114], and occupational exposures (in workers in the bagasse-containing sites in sugar cane mills) [115] may also contribute to the pathogenesis of ABPA. In addition to Aspergillosis, other fungi or yeasts can cause a similar syndrome of allergic bronchopulmonary disease (reviewed in [116]), with difficulties in assessing the sensitization to the specific fungi probably accounting for part of the low frequency of this condition as compared to ABPA.
Diagnostic Criteria
Revised criteria, which still need validation, have recently been proposed recently (Table 15.8) [108]. The diagnosis is generally made on the combination of clinical and biologic features. The classical diagnostic criteria include asthma, history of pulmonary infiltrates, proximal bronchiectasis, elevated serum IgE, and immunologic hypersensitivity to A. fumigatus (immediate reaction to prick test for Aspergillus antigen, precipitating antibodies against A. fumigatus, elevated specific IgE against A. fumigatus [117, 118]). The expectoration of mucous plugs, the presence of Aspergillus in sputum, and late skin reactivity to Aspergillus antigen [117] are also frequent findings that contribute to the diagnosis when present. Typical proximal bronchiectasis may be absent in cases designated ABPA-seropositive [119]. Of note, patients who are negative for Aspergillus fumigatus-specific IgE are unlikely to have ABPA, a feature that is helpful to rule out the disease in severe asthmatics [108]. However, since manifestations of ABPA are nonspecific, a high index of suspicion should be exerted in any asthmatic patient.
Biology
Pulmonary infiltrates with alveolar eosinophilia and/or peripheral blood eosinophilia may be present only during the acute phase or recurrent exacerbations of the disease. Blood eosinophilia is generally greater than 1 × 109/L. Sputum and expectorated plugs contain eosinophils and Charcot-Leyden crystals. Serum levels of TARC are elevated and might be used as a marker for identification and monitoring of ABPA.
Demonstration of immediate and/or late immunologic hypersensitivity to A. fumigatus is key to the diagnosis of ABPA. Out of about 40 antigenic components of Aspergillus that can bind with IgE antibodies, out of which 22 are available as recombinant allergens (named Asp f1 to Asp f22) [119], two seem to be the most helpful for diagnostic purposes (e.g. specific antibodies to recombinant Asp f4 and Asp f6) [120].
Imaging
Proximal bronchiectasis on CT (in the medial half of the lung from the hilum to the chest wall) predominating in the upper lobes [121] are considered a hallmark of ABPA, although they lack both sensitivity and specificity, and may be absent especially in early disease [108], although it has been suggested that serological ABPA (without bronchiectasis) may correspond to a variant rather than an early stage of disease [122]. Bronchiectasis represent the ultimate consequence of damage to the large bronchi by chronic inflammation. Mucoid impaction of high attenuation on CT represent mucous plugs containing Aspergillus obstructing the airways with subsequent atelectasis. Mosaic attenuation, centrilobular nodules, and tree-in-bud opacities are also commonly seen. The presence of bronchiectasis, centrilobular nodules, and mucoid impaction on CT scan are highly suggestive of ABPA in an asthmatic (Figs. 15.8, 15.9 and 15.10) [123]. Agarwal et al. have suggested a classification based on CT imaging pattern between serological ABPA (without bronchiectasis), ABPA with bronchiectasis, ABPA with high-attenuation mucus, and ABPA with pleuropulmonary fibrosis [108].

CT scan of a patient with allergic bronchopulmonary aspergillosis showing central bronchiectasis and tree-in-bud pattern in the right upper lobe, with alveolar consolidation corresponding to eosinophilic pneumonia in the left upper lobe

CT scan of a patient with allergic bronchopulmonary aspergillosis showing central bronchiectasis predominating in the left upper lobe, with mild subpleural alveolar consolidation

CT scan of a patient with allergic bronchopulmonary aspergillosis showing peripheral tree-in-bud and branching pattern in the right upper lobe
On imaging, fleeting infiltrates due to eosinophilic pneumonia or mucus plugging with ensuing segmental or lobar atelectasis are frequent during the initial stage of the disease, however the diagnosis is rarely made at this stage. A V-shaped lesion with the vertex pointing toward the hilum suggests mucoid bronchial impaction, which may be associated to atelectasis.
Treatment
Management of asthma is of primary importance in ABPA, often requiring high dose inhaled corticosteroids (which may reduce the need for long-term oral corticosteroids) and long acting bronchodilators. In addition, oral corticosteroids are used during acute exacerbations, with rapid tapering. Oral corticosteroids are maintained on the long-term only in patients with frequent symptomatic attacks or chronic symptoms, with the objective of preventing the progression to the fibrotic end stage, although with low-level evidence. In two double-blind, randomized, placebo-controlled studies [124, 125], oral itraconazole allowed reduction of the doses of corticosteroids, decrease in the number of exacerbations [125], and improvement of biologic (sputum eosinophils, sputum ECP levels, serum IgE levels, and serum IgG levels to A. fumigatus) and physiologic criteria, suggesting a clinical benefit in approximatively 60 % of patients with ABPA [126], especially those with corticosteroid-dependent ABPA; no significant effect was observed on pulmonary infiltrates [127]. Itraconazole is therefore recommended in ABPA in asthmatics [128]. It may also be useful in ABPA patients with cystic fibrosis [126, 129]. Itraconazole therapy is generally continued for a minimum of 4–6 months. Monitoring total serum IgE level may be helpful, with an objective of reducing the serum total IgE level by ≥25 % with therapy [108]. Itraconazole interacts with many medications, with a risk of adrenal insufficiency; due to frequent drug interactions, the use of oral prednisone, and inhaled beclomethasone or ciclesonide, should be preferred to that of oral methylprednisolone and inhaled budesonide or fluticasone [126].
In spite of total IgE levels that frequently exceed 1,000 IU/mL, the anti-IgE recombinant antibody omalizumab may be useful in some cases to reduce the number of episodes of exacerbation and the steroid dose [130, 131]. In isolated difficult cases, some clinical benefit was suggested with pulses of intravenous corticosteroids (to treat exacerbations), voriconazole, posaconazole, or nebulised liposomal amphotericin B.
Bronchocentric Granulomatosis
Bronchocentric granulomatosis [132] is a chronic inflammatory granulomatous and destructive process extending from the bronchiolar walls into the surrounding peribronchiolar lung parenchyma [133]. Pathology demonstrates destruction and necrosis of the mucosa and walls of bronchioles, often surrounded by palisading histiocytes and dense peribronchial inflammatory infiltrate, with occasionally scattered fungal hyphae stained by Grocott, and possible vascular inflammation and mucoid impaction [133]. In asthmatics, eosinophils are prominent within the inflammatory infiltrate of bronchocentric granulomatosis, whereas they are less conspicuous in non asthmatics. Patients with bronchocentric granulomatosis often present clinically as asthmatics who have fever, chronic cough, and peripheral blood eosinophilia greater than 1 × 109 eosinophils/L [133]. Imaging features consist of masses, alveolar opacities, or consolidation, and possible reticulonodular opacities. Abnormalities all predominate in the upper lung zones and are generally unilateral [134]. Management is based on oral corticosteroids. As most of these patients also fulfill the criteria for ABPA, this condition may be underdiagnosed. However, prognosis is excellent, with common recurrences.
Drug, Toxic Agents, and Radiation-Induced Eosinophilic Pneumonias
Eosinophilic pulmonary infiltrates can be caused by a number of drugs (Table 15.9, see www.pneumotox.com), with demonstration of causality for only a few of them. The typical patient will present with acute (or chronic) onset of eosinophilic pneumonia following the recent initiation of treatment with nonsteroidal anti-inflammatory drugs or antibiotics. Simple pulmonary eosinophilia (Löffler’s syndrome with transient pulmonary infiltrates), or chronic eosinophilic pneumonia, can also be induced by drugs. Associated extrapulmonary iatrogenic manifestations, especially cutaneous rashes, fever, or nausea, may be present. Pleural effusion is possible. Systemic eosinophilic vasculitis involving the lung and closely resembling EGPA has been reported. Cases with severe pulmonary involvement may require mechanical ventilation, or present with systemic manifestations (drug reaction with eosinophilia and systemic symptoms, DRESS) [135, 136].
A thorough history is required to suspect drug-induced eosinophilic lung disease, as the offending drug may have been taken in the weeks or months preceding the clinical syndrome, or may be denied by the patient as in the case of illicit drugs (cocaine, heroin). Pulmonary manifestations may regress after withdrawal of the suspected drug, confirming the diagnosis, however this may take a long time, and therefore corticosteroids are also frequently given. Reintroduction of the suspected drug can be dangerous and should generally be avoided, although it may be carefully be considered in rare occasions.
The toxic oil syndrome and the eosinophilia-myalgia syndrome related to preparations of L-tryptophan are historical causes of toxic-induced eosiphilic lung disease that occurred in Spain in 1981 and in the United States in 1989, respectively.
A syndrome similar to ICEP can develop up to 10 months after radiotherapy for breast cancer in women. Patients often have a history of asthma or allergy, presumably with a Th2-oriented lymphocyte response. Pulmonary opacities at imaging may be unilateral (irradiated lung) or bilateral, and occasionally migrate. Peripheral blood eosinophilia greater than 1.0 × 109/L and/or eosinophilia greater than 40 % on the BAL differential cell count distinguish this syndrome from organizing pneumonia primed by radiation therapy to the breast. Rapid improvement is obtained with oral corticosteroids, with possible relapse after treatment withdrawal.
Miscellaneous Lung Diseases with Associated Eosinophilia
Eosinophilia in blood and/or in BAL has been found in several conditions not associated with typical eosinophilic pneumonia. For example, some overlap can occur between organizing pneumonia and ICEP, with usually moderate eosinophilia in BAL in organizing pneumonia, with foci of organizing pneumonia in ICEP or conspicuous eosinophils in organizing pneumonia at pathology, or evolution of untreated CEP to organizing pneumonia.
Eosinophilic inflammation of the airways is frequent in asthma, plays a role in disease pathogeny [137], and correlates with the severity of disease [138]. Asthma is frequent in eosinophilic lung diseases, especially ABPA, ICEP, and EGPA. BAL has shown mildly increased levels of eosinophils (usually <5 %) on differential cell count in asthmatics. The eosinophilic phenotype of asthma, with eosinophilic airway inflammation and often little or no increase in the peripheral blood eosinophil numbers, is a marker of steroid-responsive disease, with a high risk of exacerbations, and may respond to anti-IL5 monoclonal antibodies [139]. Patients with asthma and high-level blood hypereosinophilia (i.e., >1.0 and especially >1.5.10−9) or alveolar eosinophilia (>25 % and especially >40 %), considered to have “hypereosinophilic asthma” [140, 141], frequently require high-dose inhaled or even oral corticosteroids, and should be monitored closely as they may progress to EGPA, ABPA, hypereosinophilic obliterative bronchiolitis, or ICEP.
Eosinophilic bronchitis (without asthma) is defined by a high percentage of eosinophils in sputum with normal lung function and absence of bronchial hyperreactivity [142]; eosinophilic bronchitis is clearly distinct from asthma and from hypereosinophilic obliterative bronchiolitis, however it can cause chronic cough responsive to inhaled corticosteroid treatment [143], and rarely may evolve to irreversible airflow obstruction [144, 145]. Treatment with an antagonist of the eotaxin tissue receptor CCR3, the receptor for eotaxin and other chemokines, may be beneficial [146]. Eosinophilic bronchitis is distinct from bronchial asthma.
Mildly increased levels of eosinophils may be found at BAL differential cell count, or may be focally present histopathologically in the idiopathic interstitial pneumonias. In pulmonary Langerhans cell histiocytosis, the pathologic lesions consist of nodules with a bronchiolocentric stellate shape composed of Langerhans cells with variable numbers of eosinophils, especially in the initial active stage and at the periphery of the lesions. Eosinophilic alveolitis in lung transplant recipients may be indicative of acute rejection (tissue eosinophilia is involved in rejection after renal, cardiac, hepatic, and pancreatic transplantation). BAL eosinophilia of 2 % or greater is associated with a poor outcome in lung transplantation [147], or may result from infection.
References
Hogan SP, Rosenberg HF, Moqbel R, Phipps S, Foster PS, Lacy P, Kay AB, Rothenberg ME. Eosinophils: biological properties and role in health and disease. Clin Exp Allergy. 2008;38:709–50.
Blanchard C, Rothenberg ME. Biology of the eosinophil. Adv Immunol. 2009;101:81–121.
Freymond N, Kahn JE, Legrand F, Renneville A, Cordier JF, Cottin V. Clonal expansion of T cells in patients with eosinophilic lung disease. Allergy. 2011;66:1506–8.
Wechsler ME, Fulkerson PC, Bochner BS, Gauvreau GM, Gleich GJ, Henkel T, Kolbeck R, Mathur SK, Ortega H, Patel J, Prussin C, Renzi P, Rothenberg ME, Roufosse F, Simon D, Simon HU, Wardlaw A, Weller PF, Klion AD. Novel targeted therapies for eosinophilic disorders. J Allergy Clin Immunol. 2012;130:563–71.
Reeder WH, Goodrich BE. Pulmonary infiltration with eosinophilia (PIE syndrome). Ann Intern Med. 1952;36:1217–40.
Crofton JW, Linvingstone JL, Oswald NC, Roberts ATM. Pulmonary eosinophilia. Thorax. 1952;7:1–35.
McCarthy DS, Pepys J. Cryptogenic pulmonary eosinophilias. Clin Allergy. 1973;3:339–51.
Carrington CB, Addington WW, Goff AM, Madoff IM, Marks A, Schwaber JR, Gaensler EA. Chronic eosinophilic pneumonia. N Engl J Med. 1969;280:787–98.
Jederlinic PJ, Sicilian L, Gaensler EA. Chronic eosinophilic pneumonia. A report of 19 cases and a review of the literature. Medicine (Baltimore). 1988;67:154–62.
Olopade CO, Crotty TB, Douglas WW, Colby TV, Sur S. Chronic eosinophilic pneumonia and idiopathic bronchiolitis obliterans organizing pneumonia: comparison of eosinophil number and degranulation by immunofluorescence staining for eosinophil-derived major basic protein. Mayo Clin Proc. 1995;70:137–42.
Tazelaar HD, Linz LJ, Colby TV, Myers JL, Limper AH. Acute eosinophilic pneumonia: histopathologic findings in nine patients. Am J Respir Crit Care Med. 1997;155:296–302.
Marchand E, Etienne-Mastroianni B, Chanez P, Lauque D, Leclerq P, Cordier JF. Idiopathic chronic eosinophilic pneumonia and asthma: how do they influence each other ? The Groupe d’Etudes et de Recherche sur les Maladies “Orphelines” Pulmonaires (GERM“O”P). Eur Respir J. 2003;22:8–13.
Marchand E, Reynaud-Gaubert M, Lauque D, Durieu J, Tonnel AB, Cordier JF. Idiopathic chronic eosinophilic pneumonia. A clinical and follow-up study of 62 cases. The Groupe d’Etudes et de Recherche sur les Maladies “Orphelines” Pulmonaires (GERM“O”P). Medicine (Baltimore). 1998;77:299–312.
Pope-Harman AL, Davis WB, Allen ED, Christoforidis AJ, Allen JN. Acute eosinophilic pneumonia. A summary of 15 cases and review of the literature. Medicine (Baltimore). 1996;75:334–42.
Valent P, Klion AD, Horny HP, Roufosse F, Gotlib J, Weller PF, Hellmann A, Metzgeroth G, Leiferman KM, Arock M, Butterfield JH, Sperr WR, Sotlar K, Vandenberghe P, Haferlach T, Simon HU, Reiter A, Gleich GJ. Contemporary consensus proposal on criteria and classification of eosinophilic disorders and related syndromes. J Allergy Clin Immunol. 2012;130:607–12.
Liebow AA, Carrington CB. The eosinophilic pneumonias. Medicine (Baltimore). 1969;48:251–85.
Hayakawa H, Sato A, Toyoshima M, Imokawa S, Taniguchi M. A clinical study of idiopathic eosinophilic pneumonia. Chest. 1994;105:1462–6.
Johkoh T, Muller NL, Akira M, Ichikado K, Suga M, Ando M, Yoshinaga T, Kiyama T, Mihara N, Honda O, Tomiyama N, Nakamura H. Eosinophilic lung diseases: diagnostic accuracy of thin-section CT in 111 patients. Radiology. 2000;216:773–80.
Furuiye M, Yoshimura N, Kobayashi A, Tamaoka M, Miyazaki Y, Ohtani Y, Miyake S, Inase N, Yoshizawa Y. Churg-Strauss syndrome versus chronic eosinophilic pneumonia on high-resolution computed tomographic findings. J Comput Assist Tomogr. 2010;34:19–22.
Arakawa H, Kurihara Y, Niimi H, Nakajima Y, Johkoh T, Nakamura H. Bronchiolitis obliterans with organizing pneumonia versus chronic eosinophilic pneumonia: high-resolution CT findings in 81 patients. AJR Am J Roentgenol. 2001;176:1053–8.
Cottin V, Deviller P, Tardy F, Cordier JF. Urinary eosinophil-derived neurotoxin/protein X: a simple method for assessing eosinophil degranulation in vivo. J Allergy Clin Immunol. 1998;101:116–23.
Durieu J, Wallaert B, Tonnel AB. Long term follow-up of pulmonary function in chronic eosinophilic pneumonia. Eur Respir J. 1997;10:286–91.
Minakuchi M, Niimi A, Matsumoto H, Amitani R, Mishima M. Chronic eosinophilic pneumonia: treatment with inhaled corticosteroids. Respiration. 2003;70:362–6.
Wechsler ME, Wong DA, Miller MK, Lawrence-Miyasaki L. Churg-strauss syndrome in patients treated with omalizumab. Chest. 2009;136:507–18.
Cazzola M, Mura M, Segreti A, Mattei MA, Rogliani P. Eosinophilic pneumonia in an asthmatic patient treated with omalizumab therapy: forme-fruste of Churg-Strauss syndrome? Allergy. 2009;64:1389–90.
Allen JA. Acute eosinophilic pneumonia. Semin Respir Crit Care Med. 2006;27:142–7.
Cheon JE, Lee KS, Jung GS, Chung MH, Cho YD. Acute eosinophilic pneumonia: radiographic and CT findings in six patients. AJR Am J Roentgenol. 1996;167:1195–9.
King MA, Pope-Harman AL, Allen JN, Christoforidis GA, Christoforidis AJ. Acute eosinophilic pneumonia: radiologic and clinical features. Radiology. 1997;203:715–9.
Rhee CK, Min KH, Yim NY, Lee JE, Lee NR, Chung MP, Jeon K. Clinical characteristics and corticosteroid treatment of acute eosinophilic pneumonia. Eur Respir J. 2013;41:402–9.
Philit F, Etienne-Mastroianni B, Parrot A, Guerin C, Robert D, Cordier JF. Idiopathic acute eosinophilic pneumonia: a study of 22 patients. The Groupe d’Etudes et de Recherche sur les Maladies “Orphelines” Pulmonaires (GERM“O”P). Am J Respir Crit Care Med. 2002;166:1235–9.
Uchiyama H, Suda T, Nakamura Y, Shirai M, Gemma H, Shirai T, Toyoshima M, Imokawa S, Yasuda K, Ida M, Nakano Y, Inui N, Sato J, Hayakawa H, Chida K. Alterations in smoking habits are associated with acute eosinophilic pneumonia. Chest. 2008;133:1174–80.
Rom WN, Weiden M, Garcia R, Yie TA, Vathesatogkit P, Tse DB, McGuinness G, Roggli V, Prezant D. Acute eosinophilic pneumonia in a New York City firefighter exposed to World Trade Center dust. Am J Respir Crit Care Med. 2002;166:797–800.
Daimon T, Johkoh T, Sumikawa H, Honda O, Fujimoto K, Koga T, Arakawa H, Yanagawa M, Inoue A, Mihara N, Tomiyama N, Nakamura H, Sugiyama Y. Acute eosinophilic pneumonia: thin-section CT findings in 29 patients. Eur J Radiol. 2008;65:462–7.
Miyazaki E, Nureki S, Ono E, Ando M, Matsuno O, Fukami T, Ueno T, Kumamoto T. Circulating thymus- and activation-regulated chemokine/CCL17 is a useful biomarker for discriminating acute eosinophilic pneumonia from other causes of acute lung injury. Chest. 2007;131:1726–34.
Lee JE, Rhee CK, Lim JH, Lee SM, Shim YS, Lee CT, Won LS. Fraction of exhaled nitric oxide in patients with acute eosinophilic pneumonia. Chest. 2012;141:1267–72.
Thompson BT, Moss M. A new definition for the acute respiratory distress syndrome. Semin Respir Crit Care Med. 2013;34:441–7.
Mochimaru H, Kawamoto M, Fukuda Y, Kudoh S. Clinicopathological differences between acute and chronic eosinophilic pneumonia. Respirology. 2005;10:76–85.
Lamb AR. Periarteritis nodosa. A clinical and pathological review of the disease. With a report of two cases. Arch Intern Med. 1914;14:481–516.
Churg J, Strauss L. Allergic granulomatosis, allergic angiitis, and periarteritis nodosa. Am J Pathol. 1951;27:277–301.
Jennette JC, Falk RJ, Andrassy K, Bacon PA, Churg J, Gross WL, Hagen EC, Hoffman GS, Hunder GG, Kallenberg CG, et al. Nomenclature of systemic vasculitides. Proposal of an international consensus conference. Arthritis Rheum. 1994;37:187–92.
Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, Flores-Suarez LF, Gross WL, Guillevin L, Hagen EC, Hoffman GS, Jayne DR, Kallenberg CG, Lamprecht P, Langford CA, Luqmani RA, Mahr AD, Matteson EL, Merkel PA, Ozen S, Pusey CD, Rasmussen N, Rees AJ, Scott DG, Specks U, Stone JH, Takahashi K, Watts RA. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013;65:1–11.
Cordier JF, Cottin V, Guillevin L, Bel E, Bottero P, Dalhoff K, Humbert M, Lazor R, Sinico RA, Sivasothy P, Wechsler ME. L5. Eosinophilic granulomatosis with polyangiitis (Churg-Strauss). Presse Med. 2013;42:507–10.
Katzenstein AL. Diagnostic features and differential diagnosis of Churg-Strauss syndrome in the lung. A review. Am J Clin Pathol. 2000;114:767–72.
Churg A. Recent advances in the diagnosis of Churg-Strauss syndrome. Mod Pathol. 2001;14:1284–93.
Lanham JG, Elkon KB, Pusey CD, Hughes GR. Systemic vasculitis with asthma and eosinophilia: a clinical approach to the Churg-Strauss syndrome. Medicine (Baltimore). 1984;63:65–81.
Reid AJ, Harrison BD, Watts RA, Watkin SW, McCann BG, Scott DG. Churg-Strauss syndrome in a district hospital. QJM. 1998;91:219–29.
Chumbley LC, Harrison Jr EG, DeRemee RA. Allergic granulomatosis and angiitis (Churg-Strauss syndrome). Report and analysis of 30 cases. Mayo Clin Proc. 1977;52:477–84.
Guillevin L, Cohen P, Gayraud M, Lhote F, Jarrousse B, Casassus P. Churg-Strauss syndrome. Clinical study and long-term follow-up of 96 patients. Medicine (Baltimore). 1999;78:26–37.
Keogh KA, Specks U. Churg-Strauss syndrome: clinical presentation, antineutrophil cytoplasmic antibodies, and leukotriene receptor antagonists. Am J Med. 2003;115:284–90.
Courand PY, Croisille P, Khouatra C, Cottin V, Kirkorian G, Bonnefoy E. Churg-Strauss syndrome presenting with acute myocarditis and cardiogenic shock. Heart Lung Circ. 2012;21:178–81.
Ginsberg F, Parrillo JE. Eosinophilic myocarditis. Heart Fail Clin. 2005;1:419–29.
Kajihara H, Tachiyama Y, Hirose T, Takada A, Saito K, Murai T, Yasui W. Eosinophilic coronary periarteritis (vasospastic angina and sudden death), a new type of coronary arteritis: report of seven autopsy cases and a review of the literature. Virchows Arch. 2013;462:239–48.
Dennert RM, van Paassen P, Schalla S, Kuznetsova T, Alzand BS, Staessen JA, Velthuis S, Crijns HJ, Tervaert JW, Heymans S. Cardiac involvement in Churg-Strauss syndrome. Arthritis Rheum. 2010;62:627–34.
Neumann T, Manger B, Schmid M, Kroegel C, Hansch A, Kaiser WA, Reinhardt D, Wolf G, Hein G, Mall G, Schett G, Zwerina J. Cardiac involvement in Churg-Strauss syndrome: impact of endomyocarditis. Medicine (Baltimore). 2009;88:236–43.
Marmursztejn J, Vignaux O, Cohen P, Guilpain P, Pagnoux C, Gouya H, Mouthon L, Legmann P, Duboc D, Guillevin L. Impact of cardiac magnetic resonance imaging for assessment of Churg-Strauss syndrome: a cross-sectional study in 20 patients. Clin Exp Rheumatol. 2009;27:S70–6.
Allenbach Y, Seror R, Pagnoux C, Teixeira L, Guilpain P, Guillevin L. High frequency of venous thromboembolic events in Churg-Strauss syndrome, Wegener’s granulomatosis and microscopic polyangiitis but not polyarteritis nodosa: a systematic retrospective study on 1130 patients. Ann Rheum Dis. 2009;68:564–7.
Chung MP, Yi CA, Lee HY, Han J, Lee KS. Imaging of pulmonary vasculitis. Radiology. 2010;255:322–41.
Choi YH, Im JG, Han BK, Kim JH, Lee KY, Myoung NH. Thoracic manifestation of Churg-Strauss syndrome: radiologic and clinical findings. Chest. 2000;117:117–24.
Kim YK, Lee KS, Chung MP, Han J, Chong S, Chung MJ, Yi CA, Kim HY. Pulmonary involvement in Churg-Strauss syndrome: an analysis of CT, clinical, and pathologic findings. Eur Radiol. 2007;17:3157–65.
Sablé-Fourtassou R, Cohen P, Mahr A, Pagnoux C, Mouthon L, Jayne D, Blockmans D, Cordier JF, Delaval P, Puechal X, Lauque D, Viallard JF, Zoulim A, Guillevin L. Antineutrophil cytoplasmic antibodies and the Churg-Strauss syndrome. Ann Intern Med. 2005;143:632–8.
Sinico RA, Di Toma L, Maggiore U, Bottero P, Radice A, Tosoni C, Grasselli C, Pavone L, Gregorini G, Monti S, Frassi M, Vecchio F, Corace C, Venegoni E, Buzio C. Prevalence and clinical significance of antineutrophil cytoplasmic antibodies in Churg-Strauss syndrome. Arthritis Rheum. 2005;52:2926–35.
Healy B, Bibby S, Steele R, Weatherall M, Nelson H, Beasley R. Antineutrophil cytoplasmic autoantibodies and myeloperoxidase autoantibodies in clinical expression of Churg-Strauss syndrome. J Allergy Clin Immunol. 2013;131:571–6.e1–6.
Bottero P, Bonini M, Vecchio F, Grittini A, Patruno GM, Colombo B, Sinico RA. The common allergens in the Churg-Strauss syndrome. Allergy. 2007;62:1288–94.
Guillevin L, Guittard T, Bletry O, Godeau P, Rosenthal P. Systemic necrotizing angiitis with asthma: causes and precipiting factors in 43 cases. Lung. 1987;165:165–72.
Ruppert AM, Averous G, Stanciu D, Deroide N, Riehm S, Poindron V, Pauli G, Debry C, de Blay F. Development of Churg-Strauss syndrome with controlled asthma during omalizumab treatment. J Allergy Clin Immunol. 2008;121:253–4.
Nathani N, Little MA, Kunst H, Wilson D, Thickett DR. Churg-Strauss syndrome and leukotriene antagonist use: a respiratory perspective. Thorax. 2008;63:883–8.
Hauser T, Mahr A, Metzler C, Coste J, Sommerstein R, Gross WL, Guillevin L, Hellmich B. The leukotriene-receptor antagonist montelukast and the risk of Churg-Strauss syndrome: a case-crossover study. Thorax. 2008;63(8):677–82.
Beasley R, Bibby S, Weatherall M. Leukotriene receptor antagonist therapy and Churg-Strauss syndrome: culprit or innocent bystander? Thorax. 2008;63:847–9.
Harrold LR, Patterson MK, Andrade SE, Dube T, Go AS, Buist AS, Chan KA, Weller PF, Wechsler ME, Yood RA, Davis KJ, Platt R, Walker AM. Asthma drug use and the development of Churg-Strauss syndrome (CSS). Pharmacoepidemiol Drug Saf. 2007;16:620–6.
Bibby S, Healy B, Steele R, Kumareswaran K, Nelson H, Beasley R. Association between leukotriene receptor antagonist therapy and Churg-Strauss syndrome: an analysis of the FDA AERS database. Thorax. 2010;65:132–8.
Jiang Y, Borrelli LA, Kanaoka Y, Bacskai BJ, Boyce JA. CysLT2 receptors interact with CysLT1 receptors and down-modulate cysteinyl leukotriene dependent mitogenic responses of mast cells. Blood. 2007;110:3263–70.
Churg A, Brallas M, Cronin SR, Churg J. Formes frustes of Churg-Strauss syndrome. Chest. 1995;108:320–3.
Masi AT, Hunder GG, Lie JT, Michel BA, Bloch DA, Arend WP, Calabrese LH, Edworthy SM, Fauci AS, Leavitt RY, Lightfoot Jr RW, McShane DJ, Mills JA, Stevens MB, Wallace SL, Zvaifler NJ. The American College of Rheumatology 1990 criteria for the classification of Churg-Strauss syndrome (allergic granulomatosis and angiitis). Arthritis Rheum. 1990;33:1094–100.
Comarmond C, Pagnoux C, Khellaf M, Cordier JF, Hamidou M, Viallard JF, Maurier F, Jouneau S, Bienvenu B, Puechal X, Aumaitre O, Le Guenno G, Le Quellec A, Cevallos R, Fain O, Godeau B, Seror R, Dunogue B, Mahr A, Guilpain P, Cohen P, Aouba A, Mouthon L, Guillevin L. Eosinophilic granulomatosis with polyangiitis (Churg-Strauss): clinical characteristics and long-term followup of the 383 patients enrolled in the French Vasculitis Study Group cohort. Arthritis Rheum. 2013;65:270–81.
Guillevin L, Lhote F, Gayraud M, Cohen P, Jarrousse B, Lortholary O, Thibult N, Casassus P. Prognostic factors in polyarteritis nodosa and Churg-Strauss syndrome. A prospective study in 342 patients. Medicine (Baltimore). 1996;75:17–28.
Abu-Shakra M, Smythe H, Lewtas J, Badley E, Weber D, Keystone E. Outcome of polyarteritis nodosa and Churg-Strauss syndrome. Arthritis Rheum. 1994;37:1798–803.
Cohen P, Pagnoux C, Mahr A, Mouthon L, Le Guern V, Andre MH, et al. Treatment of Churg-Strauss syndrome (CSS) without poor prognosis factor at baseline with corticosteroids (CS) alone. Preliminary results of a prospective multicenter trial. Arthritis Rheum. 2003;48:S209.
Guillevin L, Pagnoux C, Seror R, Mahr A, Mouthon L, Le Toumelin P. The Five-Factor Score revisited: assessment of prognoses of systemic necrotizing vasculitides based on the French Vasculitis Study Group (FVSG) cohort. Medicine (Baltimore). 2011;90:19–27.
Moosig F, Richardt G, Gross WL. A fatal attraction: eosinophils and the heart. Rheumatology (Oxford). 2013;52:587–9.
Samson M, Puechal X, Devilliers H, Ribi C, Cohen P, Stern M, Pagnoux C, Mouthon L, Guillevin L. Long-term outcomes of 118 patients with eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome) enrolled in two prospective trials. J Autoimmun. 2013;43:60–9.
Ribi C, Cohen P, Pagnoux C, Mahr A, Arene JP, Lauque D, Puechal X, Letellier P, Delaval P, Cordier JF, Guillevin L. Treatment of Churg-Strauss syndrome without poor-prognosis factors: a multicenter, prospective, randomized, open-label study of seventy-two patients. Arthritis Rheum. 2008;58:586–94.
Bourgarit A, Le Toumelin P, Pagnoux C, Cohen P, Mahr A, Le Guern V, Mouthon L, Guillevin L. Deaths occurring during the first year after treatment onset for polyarteritis nodosa, microscopic polyangiitis, and Churg-Strauss syndrome: a retrospective analysis of causes and factors predictive of mortality based on 595 patients. Medicine (Baltimore). 2005;84:323–30.
Cottin V, Khouatra C, Dubost R, Glerant JC, Cordier JF. Persistent airflow obstruction in asthma of patients with Churg-Strauss syndrome and long-term follow-up. Allergy. 2009;64:589–95.
Szczeklik W, Sokolowska BM, Zuk J, Mastalerz L, Szczeklik A, Musial J. The course of asthma in Churg-Strauss syndrome. J Asthma. 2011;48:183–7.
Chusid MJ, Dale DC, West BC, Wolff SM. The hypereosinophilic syndrome: analysis of fourteen cases with review of the literature. Medicine (Baltimore). 1975;54:1–27.
Simon HU, Plotz SG, Dummer R, Blaser K. Abnormal clones of T cells producing interleukin-5 in idiopathic eosinophilia. N Engl J Med. 1999;341:1112–20.
Roufosse F, Schandene L, Sibille C, Willard-Gallo K, Kennes B, Efira A, Goldman M, Cogan E. Clonal Th2 lymphocytes in patients with the idiopathic hypereosinophilic syndrome. Br J Haematol. 2000;109:540–8.
Cools J, DeAngelo DJ, Gotlib J, Stover EH, Legare RD, Cortes J, Kutok J, Clark J, Galinsky I, Griffin JD, Cross NC, Tefferi A, Malone J, Alam R, Schrier SL, Schmid J, Rose M, Vandenberghe P, Verhoef G, Boogaerts M, Wlodarska I, Kantarjian H, Marynen P, Coutre SE, Stone R, Gilliland DG. A tyrosine kinase created by fusion of the PDGFRA and FIP1L1 genes as a therapeutic target of imatinib in idiopathic hypereosinophilic syndrome. N Engl J Med. 2003;348:1201–14.
Griffin JH, Leung J, Bruner RJ, Caligiuri MA, Briesewitz R. Discovery of a fusion kinase in EOL-1 cells and idiopathic hypereosinophilic syndrome. Proc Natl Acad Sci U S A. 2003;100:7830–5.
Fauci AS, Harley JB, Roberts WC, Ferrans VJ, Gralnick HR, Bjornson BH. The idiopathic hypereosinophilic syndrome: clinical, pathophysiologic and therapeutic considerations. Ann Intern Med. 1982;97:78–92.
Spry CJF, Davies J, Tai PC, Olsen EGJ, Oakley CM, Goodwin JF. Clinical features of fifteen patients with the hypereosinophilic syndrome. Q J Med. 1983;205:1–22.
Dulohery MM, Patel RR, Schneider F, Ryu JH. Lung involvement in hypereosinophilic syndromes. Respir Med. 2011;105:114–21.
Ommen SR, Seward JB, Tajik AJ. Clinical and echocardiographic features of hypereosinophilic syndromes. Am J Cardiol. 2001;86:110–3.
Ogbogu PU, Bochner BS, Butterfield JH, Gleich GJ, Huss-Marp J, Kahn JE, Leiferman KM, Nutman TB, Pfab F, Ring J, Rothenberg ME, Roufosse F, Sajous MH, Sheikh J, Simon D, Simon HU, Stein ML, Wardlaw A, Weller PF, Klion AD. Hypereosinophilic syndrome: a multicenter, retrospective analysis of clinical characteristics and response to therapy. J Allergy Clin Immunol. 2009;124:1319–25.e3.
Legrand F, Renneville A, Macintyre E, Mastrilli S, Ackermann F, Cayuela JM, Rousselot P, Schmidt-Tanguy A, Fain O, Michel M, de Jaureguiberry JP, Hatron PY, Cony-Makhoul P, Lefranc D, Sene D, Cottin V, Hamidou M, Lidove O, Baruchel A, Dubucquoi S, Bletry O, Preudhomme C, Capron M, Prin L, Kahn JE. The spectrum of FIP1L1-PDGFRA-associated chronic eosinophilic leukemia: new insights based on a survey of 44 cases. Medicine (Baltimore) 2013. Epub ahead of print
Rothenberg ME, Klion AD, Roufosse FE, Kahn JE, Weller PF, Simon HU, Schwartz LB, Rosenwasser LJ, Ring J, Griffin EF, Haig AE, Frewer PI, Parkin JM, Gleich GJ. Treatment of patients with the hypereosinophilic syndrome with mepolizumab. N Engl J Med. 2008;358:1215–28.
Roufosse FE, Kahn JE, Gleich GJ, Schwartz LB, Singh AD, Rosenwasser LJ, Denburg JA, Ring J, Rothenberg ME, Sheikh J, Haig AE, Mallett SA, Templeton DN, Ortega HG, Klion AD. Long-term safety of mepolizumab for the treatment of hypereosinophilic syndromes. J Allergy Clin Immunol. 2013;131:461–7.e1–5.
Cordier JF, Cottin V, Khouatra C, Revel D, Proust C, Freymond N, Thivolet-Bejui F, Glerant JC. Hypereosinophilic obliterative bronchiolitis: a distinct, unrecognised syndrome. Eur Respir J. 2013;41:1126–34.
Takayanagi N, Kanazawa M, Kawabata Y, Colby TV. Chronic bronchiolitis with associated eosinophilic lung disease (eosinophilic bronchiolitis). Respiration. 2001;68:319–22.
Fukushima Y, Kamiya K, Tatewaki M, Fukushima F, Hirata H, Ishii Y, Fukuda T. A patient with bronchial asthma in whom eosinophilic bronchitis and bronchiolitis developed during treatment. Allergol Int. 2010;59:87–91.
Cordier JF, Cottin V. Eosinophilic pneumonias. In: Schwarz MI, King Jr TE, editors. Interstitial lung disease. 5th ed. Shelton: People’s Medical Publishing House-USA; 2011. p. 833–93.
Vijayan VK. How to diagnose and manage common parasitic pneumonias. Curr Opin Pulm Med. 2007;13:218–24.
Vijayan VK. Tropical pulmonary eosinophilia: pathogenesis, diagnosis and management. Curr Opin Pulm Med. 2007;13:428–33.
Fillaux J, Magnaval JF. Laboratory diagnosis of human toxocariasis. Vet Parasitol. 2013;193:327–36.
Graham BB, Chabon J, Bandeira A, Espinheira L, Butrous G, Tuder RM. Significant intrapulmonary Schistosoma egg antigens are not present in schistosomiasis-associated pulmonary hypertension. Pulm Circ. 2011;1:456–61.
Geller DE, Kaplowitz H, Light MJ, Colin AA. Allergic bronchopulmonary aspergillosis in cystic fibrosis: reported prevalence, regional distribution, and patient characteristics. Chest. 1999;116:639–46.
Mastella G, Rainisio M, Harms HK, Hodson ME, Koch C, Navarro J, Strandvik B, McKenzie SG. Allergic bronchopulmonary aspergillosis in cystic fibrosis. A European epidemiological study. Epidemiologic Registry of Cystic Fibrosis. Eur Respir J. 2000;16:464–71.
Agarwal R, Chakrabarti A, Shah A, Gupta D, Meis JF, Guleria R, Moss R, Denning DW. Allergic bronchopulmonary aspergillosis: review of literature and proposal of new diagnostic and classification criteria. Clin Exp Allergy. 2013;43:850–73.
Leonard CT, Berry GJ, Ruoss SJ. Nasal-pulmonary relations in allergic fungal sinusitis and allergic bronchopulmonary aspergillosis. Clin Rev Allergy Immunol. 2001;21:5–15.
Murdock BJ, Falkowski NR, Shreiner AB, Sadighi Akha AA, McDonald RA, White ES, Toews GB, Huffnagle GB. Interleukin-17 drives pulmonary eosinophilia following repeated exposure to Aspergillus fumigatus conidia. Infect Immun. 2012;80:1424–36.
Marchand E, Verellen-Dumoulin C, Mairesse M, Delaunois L, Brancaleone P, Rahier JF, Vandenplas O. Frequency of cystic fibrosis transmembrane conductance regulator gene mutations and 5 T allele in patients with allergic bronchopulmonary aspergillosis. Chest. 2001;119:762–7.
Agarwal R, Khan A, Aggarwal AN, Gupta D. Link between CFTR mutations and ABPA: a systematic review and meta-analysis. Mycoses. 2012;55:357–65.
Mussaffi H, Rivlin J, Shalit I, Ephros M, Blau H. Nontuberculous mycobacteria in cystic fibrosis associated with allergic bronchopulmonary aspergillosis and steroid therapy. Eur Respir J. 2005;25:324–8.
Judson MA. Allergic bronchopulmonary aspergillosis after infliximab therapy for sarcoidosis: a potential mechanism related to T-helper cytokine balance. Chest. 2009;135:1358–9.
Mehta SK, Sandhu RS. Immunological significance of Aspergillus fumigatus in cane-sugar mills. Arch Environ Health. 1983;38:41–6.
Chowdhary A, Agarwal K, Kathuria S, Gaur SN, Randhawa HS, Meis JF. Allergic bronchopulmonary mycosis due to fungi other than Aspergillus: a global overview. Crit Rev Microbiol. 2014;40:30–48.
Rosenberg M, Patterson R, Mintzer R, Cooper BJ, Roberts M, Harris KE. Clinical and immunologic criteria for the diagnosis of allergic bronchopulmonary aspergillosis. Ann Intern Med. 1977;86:405–14.
Patterson R, Grammer LC. Immunopathogenesis of allergic bronchopulmonary aspergillosis. In: Patterson R, Greenberger PA, Roberts ML, editors. Allergic bronchopulmonary aspergillosis. Providence: OceanSide Publications Inc.; 1995. p. 35–8.
Greenberger PA. Allergic bronchopulmonary aspergillosis. J Allergy Clin Immunol. 2002;110:685–92.
Crameri R, Weichel M, Fluckiger S, Glaser AG, Rhyner C. Fungal allergies: a yet unsolved problem. Chem Immunol Allergy. 2006;91:121–33.
Mitchell TA, Hamilos DL, Lynch DA, Newell JD. Distribution and severity of bronchiectasis in allergic bronchopulmonary aspergillosis (ABPA). J Asthma. 2000;37:65–72.
Agarwal R, Garg M, Aggarwal AN, Saikia B, Gupta D, Chakrabarti A. Serologic allergic bronchopulmonary aspergillosis (ABPA-S): long-term outcomes. Respir Med. 2012;106:942–7.
Ward S, Heyneman L, Lee MJ, Leung AN, Hansell DM, Muller NL. Accuracy of CT in the diagnosis of allergic bronchopulmonary aspergillosis in asthmatic patients. AJR Am J Roentgenol. 1999;173:937–42.
Salez F, Brichet A, Desurmont S, Grosbois JM, Wallaert B, Tonnel AB. Effects of itraconazole therapy in allergic bronchopulmonary aspergillosis. Chest. 1999;116:1665–8.
Wark P. Pathogenesis of allergic bronchopulmonary aspergillosis and an evidence-based review of azoles in treatment. Respir Med. 2004;98:915–23.
Moss RB. Treatment options in severe fungal asthma and allergic bronchopulmonary aspergillosis. Eur Respir J. 2014;43:1487–500.
Stevens DA, Schwartz HJ, Lee JY, Moskovitz BL, Jerome DC, Catanzaro A, Bamberger DM, Weinmann AJ, Tuazon CU, Judson MA, Platts-Mills TA, DeGraff Jr AC. A randomized trial of itraconazole in allergic bronchopulmonary aspergillosis. N Engl J Med. 2000;342:756–62.
Wark PA, Gibson PG, Wilson AJ. Azoles for allergic bronchopulmonary aspergillosis associated with asthma. Cochrane Database Syst Rev. 2004;(3):CD001108.
Elphick HE, Southern KW. Antifungal therapies for allergic bronchopulmonary aspergillosis in people with cystic fibrosis. Cochrane Database Syst Rev. 2012;(6):CD002204.
Tillie-Leblond I, Germaud P, Leroyer C, Tetu L, Girard F, Devouassoux G, Grignet JP, Prudhomme A, Dusser D, Wallaert B. Allergic bronchopulmonary aspergillosis and omalizumab. Allergy. 2011;66:1254–6.
Perez-de-Llano LA, Vennera MC, Parra A, Guallar J, Marin M, Asensio O, Ausin P, Borderias L, Fernandez C, Granel C, Perez-Pimiento A, Rubio M. Effects of omalizumab in Aspergillus-associated airway disease. Thorax. 2011;66:539–40.
Liebow AA. Pulmonary angiitis and granulomatosis. Am Rev Respir Dis. 1973;108:1–18.
Katzenstein AL, Askin FB. Katzenstein and Askin’s surgical pathology of non-neoplastic lung disease. 3rd ed. Philadelphia: W.B. Saunders; 1997.
Ward S, Heyneman LE, Flint JD, Leung AN, Kazerooni EA, Muller NL. Bronchocentric granulomatosis: computed tomographic findings in five patients. Clin Radiol. 2000;55:296–300.
Husain Z, Reddy BY, Schwartz RA. DRESS syndrome: part I. Clinical perspectives. J Am Acad Dermatol. 2013;68:693 e1–14; quiz 706–8.
Husain Z, Reddy BY, Schwartz RA. DRESS syndrome: part II. Management and therapeutics. J Am Acad Dermatol. 2013;68:709 e1–9; quiz 718–20.
Bousquet J, Chanez P, Vignola AM, Lacoste JY, Michel FB. Eosinophil inflammation in asthma. Am J Respir Crit Care Med. 1994;150:533–8.
Bousquet J, Chanez P, Lacoste JY, Barneon G, Ghavanian N, Enander I, Venge P, Ahlstedt S, Simony-Lafontaine J, Godard P. Eosinophilic inflammation in asthma. N Engl J Med. 1990;323:1033–9.
Pavord ID. Eosinophilic phenotypes of airway disease. Ann Am Thorac Soc. 2013;10(Suppl):S143–9.
Cordier JF. Asthmes hyperéosinophiliques. Rev Fr Allergol Immunol Clin. 2004;44:92–5.
Cordier JF, Freymond N, Cottin V. Asthme hyperéosinophilique [Hypereosinophilic asthma]. Rev Prat. 2011;61:325–6.
Gibson PG, Dolovich J, Denburg J, Ramsdale EH, Hargreave FE. Chronic cough: eosinophilic bronchitis without asthma. Lancet. 1989;1:1346–8.
Brightling CE. Chronic cough due to nonasthmatic eosinophilic bronchitis: ACCP evidence-based clinical practice guidelines. Chest. 2006;129:116S–21.
Park SW, Lee YM, Jang AS, Lee JH, Hwangbo Y, Kim DJ, Park CS. Development of chronic airway obstruction in patients with eosinophilic bronchitis: a prospective follow-up study. Chest. 2004;125:1998–2004.
Brightling CE, Woltmann G, Wardlaw AJ, Pavord ID. Development of irreversible airflow obstruction in a patient with eosinophilic bronchitis without asthma. Eur Respir J. 1999;14:1228–30.
Neighbour H, Boulet LP, Lemiere C, Sehmi R, Leigh R, Sousa AR, Martin J, Dallow N, Gilbert J, Allen A, Hall D, Nair P. Safety and efficacy of an oral CCR3 antagonist in patients with asthma and eosinophilic bronchitis: a randomized, placebo-controlled clinical trial. Clin Exp Allergy. 2014;44:508–16.
Verleden SE, Ruttens D, Vandermeulen E, van Raemdonck DE, Vanaudenaerde BM, Verleden GM, Vos R. Elevated bronchoalveolar lavage eosinophilia correlates with poor outcome after lung transplantation. Transplantation. 2014;97:83–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer-Verlag London
About this chapter
Cite this chapter
Cottin, V., Cordier, JF. (2015). Eosinophilic Pneumonia. In: Cottin, V., Cordier, JF., Richeldi, L. (eds) Orphan Lung Diseases. Springer, London. https://doi.org/10.1007/978-1-4471-2401-6_15
Download citation
DOI: https://doi.org/10.1007/978-1-4471-2401-6_15
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-4471-2400-9
Online ISBN: 978-1-4471-2401-6
eBook Packages: MedicineMedicine (R0)