
Abstract
Aim
To evaluate the clinical features, hormonal activity and natural evolution of adrenal incidentalomas (AI) in patients investigated in a single endocrinological centre and compare the prevalence of metabolic disorders and hypertension between subjects with AI and the general population.
Patients and methods
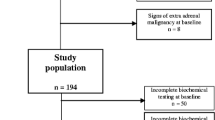
515 patients with AI evaluated between 1995 and 2010 were retrospectively included in the study. Their anthropometric, clinical, metabolic and hormonal parameters were analyzed. Follow-up data was available for 142 patients.
Results
Mean age of all participants was 53.45 ± 13.4 years (range 13–84) with strong female predominance — 376 (73%) vs. 139 (27%) males. Median size of AI was 28 mm (range 10–190 mm). Hormonal investigations revealed that 82.9% of patients harboured non-functioning adenomas, subclinical hypercortisolism was detected in 5.94%, overt Cushing’s syndrome — in 2.7%, pheochromocytoma — in 1.9% and primary aldosteronism was diagnosed in 1% of patients. Adrenal carcinoma was identified in 1.7%. The prevalence of metabolic abnormalities and hypertension did not differ between patients with subclinical Cushing’s syndrome and non-functioning adrenal adenomas. When compared to the general population, however hypertension, type 2 diabetes and metabolic syndrome were significantly more common in patients with hormonally inactive tumours. During the course of followup progression to overt hormonal hypersecretion was not observed.
Conclusion
These results confirm other contemporary studies reporting lower rates of hormonally active and malignant lesions among AI as well as increased prevalence of hypertension and metabolic abnormalities in patients with non-functioning adrenal adenomas.
Similar content being viewed by others

References
Barzon L, Sonino N, Fallo F, Palu G, Boscaro M. Prevalence and natural history of adrenal incidentalomas. Eur J Endocrinol. 2003;149(4):273–285
Kloos RT, Gross MD, Francis IR, Korobkin M, Shapiro B. Incidentally discovered adrenal masses. Endocr Rev. 1995;16(4):460–484
Prinz RA, Brooks MH, Churchill R, et al. Incidental asymptomatic adrenal masses detected by computed tomographic scanning. Is operation required? JAMA. 1982;248(6):701–704
Herrera MF, Grant CS, van Heerden JA, Sheedy PF, Ilstrup DM. Incidentally discovered adrenal tumors: an institutional perspective. Surgery. 1991;110(6):1014–1021
Caplan RH, Strutt PJ, Wickus GG. Subclinical hormone secretion by incidentally discovered adrenal masses. Arch Surg. 1994;129(3):291–296
Bovio S, Cataldi A, Reimondo G, et al. Prevalence of adrenal incidentaloma in a contemporary computerized tomography series. J Endocrinol Invest. 2006;29(4):298–302
Aron D, Terzolo M, Cawood TJ. Adrenal incidentalomas. Best Pract Res Clin Endocrinol Metab. 2012;26(1):69–82
NIH state-of-the-science statement on management of the clinically inapparent adrenal mass (“incidentaloma”). NIH Consens State Sci Statements. 2002;19(2):1–25
Terzolo M, Stigliano A, Chiodini I, et al. AME position statement on adrenal incidentaloma. Eur J Endocrinol. 2011;164(6):851–870
Zeiger MA, Thompson GB, Duh QY, et al. American Association of Clinical Endocrinologists and American Association of Endocrine Surgeons Medical Guidelines for the Management of Adrenal Incidentalomas: executive summary of recommendations. Endocr Pract. 2009;15(5):450–453
Garrapa GG, Pantanetti P, Arnaldi G, Mantero F, Faloia E. Body composition and metabolic features in women with adrenal incidentaloma or Cushing’s syndrome. J Clin Endocrinol Metab. 2001;86(11):5301–5306
Rossi R, Tauchmanova L, Luciano A, et al. Subclinical Cushing’s syndrome in patients with adrenal incidentaloma: clinical and biochemical features. J Clin Endocrinol Metab. 2000;85(4):1440–1448
Terzolo M, Pia A, Ali A, et al. Adrenal incidentaloma: a new cause of the metabolic syndrome? J Clin Endocrinol Metab. 2002;87(3):998–1003
Tauchmanova L, Rossi R, Biondi B, et al. Patients with subclinical Cushing’s syndrome due to adrenal adenoma have increased cardiovascular risk. J Clin Endocrinol Metab. 2002;87(11):4872–4878
Erbil Y, Ozbey N, Barbaros U, Unalp HR, Salmaslioglu A, Ozarmagan S. Cardiovascular risk in patients with nonfunctional adrenal incidentaloma: myth or reality? World J Surg. 2009;33(10):2099–2105
Sereg M, Szappanos A, Toke J, et al. Atherosclerotic risk factors and complications in patients with nonfunctioning adrenal adenomas treated with or without adrenalectomy: a long-term follow-up study. Eur J Endocrinol. 2009;160(4):647–655
Bernini G, Moretti A, Iacconi P, et al. Anthropometric, haemodynamic, humoral and hormonal evaluation in patients with incidental adrenocortical adenomas before and after surgery. Eur J Endocrinol. 2003;148(2):213–219
Fernandez-Real JM, Gonzalbez J, Ricart W. Metabolic abnormalities in patients with adrenal incidentaloma. J Clin Endocrinol Metab. 2001;86(2):950–952
Lazurova I, Dudasova D, Wagnerova H, Dravecka I, Petrasova D. Adrenal incidentalomas and the metabolic syndrome—are there any differences between adenoma and hyperplasia? Neoplasma. 2006;53(4):324–327
Terzolo M, Reimondo G, Bovio S, Angeli A. Subclinical Cushing’s syndrome. Pituitary. 2004;7(4):217–223
Emral R, Uysal AR, Asik M, et al. Prevalence of subclinical Cushing’s syndrome in 70 patients with adrenal incidentaloma: clinical, biochemical and surgical outcomes. Endocr J. 2003;50(4):399–408
Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, Bornstein SR. The clinically inapparent adrenal mass: update in diagnosis and management. Endocr Rev. 2004;25(2):309–340
Barzon L, Fallo F, Sonino N, Boscaro M. Development of overt Cushing’s syndrome in patients with adrenal incidentaloma. Eur J Endocrinol. 2002;146(1):61–66
Mazzuco TL, Bourdeau I, Lacroix A. Adrenal incidentalomas and subclinical Cushing’s syndrome: diagnosis and treatment. Curr Opin Endocrinol Diabetes Obes. 2009;16(3):203–210
Abdelmannan D, Aron DC. Adrenal incidentalomas and subclinical Cushing’s syndrome. Rev Endocr Metab Disord. 2010;11(2):135–140
World Health Organization: Definition and diagnosis of diabetes mellitus and intermediate hyperglycemia. Report of a WHO consultation. Geneva (Switzerland): World Health Organization, 2006
Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106(25):3143–3421
International Diabetes Federation. The IDF consensus worldwide definition of the metabolic syndrome. 2005
Borissova AM, Kovatcheva R, Shinkov A, et al. Endocrine disorders and cardiovascular risk. Endokrinologya. 2007;12(4):188–202
Borissova AM, Kovatcheva R, Shinkov A, et al. Prevalence and features of the metabolic syndrome in unselected Bulgarian population. Endokrinologya. 2007;12(2):68–77
Mantero F, Terzolo M, Arnaldi G, et al. A survey on adrenal incidentaloma in Italy. Study Group on Adrenal Tumors of the Italian Society of Endocrinology. J Clin Endocrinol Metab. 2000;85(2):637–644
Muth A, Hammarstedt L, Hellstrom M, Sigurjonsdottir HA, Almqvist E, Wangberg B. Cohort study of patients with adrenal lesions discovered incidentally. Br J Surg. 2011;98(10):1383–1391
Comlekci A, Yener S, Ertilav S, et al. Adrenal incidentaloma, clinical, metabolic, follow-up aspects: single centre experience. Endocrine. 2010;37(1):40–46
Barzon L, Scaroni C, Sonino N, et al. Incidentally discovered adrenal tumors: endocrine and scintigraphic correlates. J Clin Endocrinol Metab. 1998;83(1):55–62
Yeh HC. Sonography of the adrenal glands: normal glands and small masses. AJR Am J Roentgenol. 1980;135(6):1167–1177
Cawood TJ, Hunt PJ, O’Shea D, Cole D, Soule S. Recommended evaluation of adrenal incidentalomas is costly, has high false-positive rates and confers a risk of fatal cancer that is similar to the risk of the adrenal lesion becoming malignant; time for a rethink? Eur J Endocrinol. 2009;161(4):513–527
Aso Y, Homma Y. A survey on incidental adrenal tumors in Japan. J Urol. 1992;147(6):1478–1481
Terzolo M, Bovio S, Reimondo G, et al. Subclinical Cushing’s syndrome in adrenal incidentalomas. Endocrinol Metab Clin North Am. 2005;34(2):423–439, x
Stewart PM. Is subclinical Cushing’s syndrome an entity or a statistical fallout from diagnostic testing? Consensus surrounding the diagnosis is required before optimal treatment can be defined. J Clin Endocrinol Metab. 2010;95(6):2618–2620
Zeiger MA, Siegelman SS, Hamrahian AH. Medical and surgical evaluation and treatment of adrenal incidentalomas. J Clin Endocrinol Metab. 2011;96(7):2004–2015
Nieman LK, Biller BM, Findling JW, et al. The diagnosis of Cushing’s syndrome: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2008;93(5):1526–1540
Chiodini I, Morelli V, Masserini B, et al. Bone mineral density, prevalence of vertebral fractures, and bone quality in patients with adrenal incidentalomas with and without subclinical hypercortisolism: an Italian multicenter study. J Clin Endocrinol Metab. 2009;94(9):3207–3214
Giordano R, Marinazzo E, Berardelli R, et al. Longterm morphological, hormonal, and clinical follow-up in a single unit on 118 patients with adrenal incidentalomas. Eur J Endocrinol. 2010;162(4):779–785
Vassilatou E, Vryonidou A, Michalopoulou S, et al. Hormonal activity of adrenal incidentalomas: results from a long-term follow-up study. Clin Endocrinol (Oxf). 2009;70(5):674–679
Tsuiki M, Tanabe A, Takagi S, Naruse M, Takano K. Cardiovascular risks and their long-term clinical outcome in patients with subclinical Cushing’s syndrome. Endocr J. 2008;55(4):737–745
Toniato A, Merante-Boschin I, Opocher G, Pelizzo MR, Schiavi F, Ballotta E. Surgical versus conservative management for subclinical Cushing syndrome in adrenal incidentalomas: a prospective randomized study. Ann Surg. 2009;249(3):388–391
Erbil Y, Ademoglu E, Ozbey N, et al. Evaluation of the cardiovascular risk in patients with subclinical Cushing syndrome before and after surgery. World J Surg. 2006;30(9):1665–1671
Vasilev V, Kirilov G, Zacharieva S. Impaired steroidogenesis in patients with clinically inactive adrenal adenomas, revealed by analysis of steroid precursors. Endokrinologya. 2011;16(2):68–77
Reincke M, Fassnacht M, Vath S, Mora P, Allolio B. Adrenal incidentalomas: a manifestation of the metabolic syndrome? Endocr Res. 1996;22(4):757–761
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Vasilev, V., Matrozova, J., Elenkova, A. et al. Clinical characteristics and follow-up of incidentally found adrenal tumours — results from a single tertiary centre. cent.eur.j.med 9, 292–301 (2014). https://doi.org/10.2478/s11536-013-0199-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.2478/s11536-013-0199-9