
Abstract
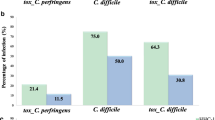
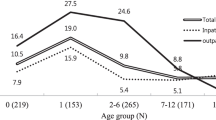
The aim of the research was to determine the intestinal carriers of C. difficile in different human population groups in Serbia. The research enrolled 877 persons with formed stools: (newborn children in maternity hospitals for up to two weeks old) (23), group A; children aged from two weeks to two years (121), group B; children aged two to 10 years (54), group C, healthy individuals aged 10 and over (516), group D; patients hospitalized for at least 48 hours (100), group E; staff of the Clinical Center in Nis, Serbia, (63), group F. The toxins A and B of C. difficile were detected by ELISA-ridascreen Clostridium difficile Toxin A/B (R — Biopharm AG, Darmstadt, Germany). The toxin A of C. difficile was detected using ColorPAC Toxin A test (BectonDickinson, New Jersey, USA). Out of the total number of persons (877), the carriers of certain types of toxin-producing strains of C. difficile were distributed as: 6.04% (A−/B−), 1.83% (A+/B+) and 0.11% (A−/B+). In most groups (5/6), the dominance of non-toxigenic (A−/B−) isolates was established, with the rate of carriers 1.75 – 30.43% depending on the group. Toxigenic isolates were prevalent only in the group F in relation to non — toxigenic (7.94% versus 4.76% of persons). In other groups, the carriers of toxigenic strains ranged from 0.00 – 17.45%. The presence of asymptomatic intestinal carriers of C. difficile in the human population, indicate the possible reservoirs and sources of infection.
Similar content being viewed by others

References
Bouza E, Munoz P, Alonso R. Clinical manifestations, tretment and control of infections caused by Clostridium difficile. Clin Microbiol Infec 2005;11(4):57–64
Bolton R, Tait S, Dear P, Losowsky MS. Asymptomatic neonatal colonisation by Clostridium difficile. Arch Dis Child 1984; 59(5):466–72
Kato H, Kita H, Karasawa T, Maegawa T, Koino Y, Takakuwa H et al. Colonisation and transmission of Clostridium difficile in healthy individuals examined by ribotiping and pulsed-field gel electrophoresis. J Med Microbiol 2001; 50(8):720–727
Simor A, Yeke S, Tsimidis K. Infection due to Clostridium difficile among elderly of a Long-termcare facilities. Clin Infect Dis 1993; 17(4):672–678
Simor A, Bradley S, Strausbaugh LJ, Crossley K, Nicolle L. Clostridium difficile in Long-term-care facilities for the elderly. Infect Contr Hosp Epidem 2002; 23(11):696–703
Larson H, Barcley F, Honour P, Hill I. Epidemiology of Clostridium difficile in infants. J Infect Dis 1982; 146(6):727–733
Matsuki S, Ozaki E, Shouzi M, Inoue M, Shimizu S, Yamaguchi N et al. Colonization by Clostridium difficile in a hospital, and infants and children in three day-care facilities of Kanazawa, Japan. Internac Microbiol 2005; 8(1):43–48
El Mohandes A, Keiser J, Refat M, Jackson B. Prevalence and toxigenicity of Clostridium difficile isolates in fecal microflora of preterm infants care nursery. Biol Neonate 1993; 63(4):225–229
Riggs M, Seithi A, Zabarsky T, Eckstein E, Jump R, Donskey C. Asymptomatic carriers are a potential source for transmission of epidemic and nonepidemic Clostridium difficile strains among Long-term care facility residents. Clinic Infect Dis 2007; 45(8):992–998
Nakamura S, Mikawa M, Nakashio S, Takabatake M, Okaida I, Yamakawa K et al. Isolation of Clostridium difficile from feces and the antibody in sera of young and elderly adults. Microbiol Immun 1981; 25(4):345–351
Larson H, Price A, Honour P, Borellio S. Clostridium difficile and the aetiology of pseudomembranous colitis. Lancet 1978; 1(8073):1063–1066
Ryan J, Murphy C, Twomey C, Paul Ross R, Rea M, MacSharry J et al. Asymptomatic carriage of Clostridium difficile in a Irish continuing care institution for the elderl: prevalence and characteristics. Ir J Med Sci 2010; 179(2):245–250
Walker K, Gilliland S, Vance-Bryan K, Moody J, Larsson A, Rotschafer J et al. Clostridium difficile in residents of long-term care facilities: prevalence and risk factors. J Am Geriatr Soc 1993; 41(9):940–946
Rudensky B, Rosoner S, Sonnenblick M, van Dijk Y, Shapira E, Isaacsohn M. The prevalence and nosocomial acquisition of Clostridium difficile in elderly hospitalized patients. Postgrad Med J 1993; 69(807):45–47
McFarland L, Mulligan M, Kwok R, Stamm W. Nosocomial aquisition of Clostridium dificile infection. N Engl J Med 1989; 320(4):204–210
Thibault A, Miller MA, Gaese C. Risk factors for the development of Clostridium diffcile-associated diarrhea during a hospital outbreak. Infect Control Hospital Epidemiol 1991; 12(6):345–348
Clabots R, Johnson S, Olson MM, Peterson LR, Gerding DL. Acquisition of Clostridium difficile by hospitalized patients: evidence for colonized new admissions as source of infection. J Infect Dis 1992; 166(3):561–567
Brooks SE, Veal RO, Kramer M, Dore L, Schupf N, Adachi M. Reduction in the incidence of Clostridium diffcile-associated diarrhea in acute care hospital and a skilled nursing facility following replacement of electronic thermometers with single use disposable. Infect Control Hospital Epidemiol 1992; 13(2):98–103
Aslam S, Hamill R, Musher D. Treatment of Clostridium difficile-associated disease: Old therapies and new strategies. Lancet Infect Dis 2005; 5(9):549–557
Kyne L, Warny M, Qamar A, Kelly CP. Association between antibody response to toxin A and protection against recurrent Clostridium difficile diarrhoea. Lancet 2001; 357(9251):189–193
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Stojanović, P., Stojanović, N., Kocic, B. et al. Asymptomatic carriers of clostridium difficile in serbian population. cent.eur.j.med 7, 769–774 (2012). https://doi.org/10.2478/s11536-012-0067-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.2478/s11536-012-0067-z