
Abstract
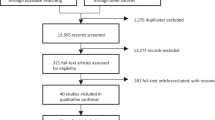
Depression is a recurrent illness in which afflicted individuals have an increased risk for recurrence as a function of a greater number of previous episodes. Consequently, prevention of future episodes is central to improving the prognosis. The current recommendation is to use antidepressants over prolonged periods of time to prevent further episodes of depression. However, the database for this practice is limited and can be interpreted in multiple ways. Review of the relevant literature was performed. MEDLINE and PubMed databases were searched from inception to 5 September 2011 for randomized, placebo-controlled trials of at least 18 months duration. After treatment of an acute depressive episode, antidepressants clearly prevent relapse back into the same depressive episode. This is demonstrated by an adequate number of randomized, blinded, placebo-controlled, 1-year continuation trials. The ability of antidepressants to prevent recurrence of future episodes is less clear. Randomized, blinded, placebo-controlled trials of 18 months or longer are infrequent-18 studies were identified. While nearly all show that antidepressant continuation is superior to placebo in preventing resurgence of depressive symptoms, nearly all of the difference occurs in the first 6 months after randomization. This pattern strongly suggests that the apparent superiority of antidepressants may be due to (i) their ability to prevent recurrence, (ii) antidepressant withdrawal (characterized by depressive symptoms) in patients switched to placebo or (iii) a combination of these phenomena.



Similar content being viewed by others

References
Solomon DA, Keller MB, Leon AC, et al. Multiple recurrences of major depressive disorder. Am J Psychiatry 2000; 157: 229–33
Mueller TI, Leon AC, Keller MB, et al. Recurrence after recovery from major depressive disorder during 15 years of observational follow-up. Am J Psychiatry 1999; 156: 1000–6
Angst J. Course ofunipolar depressive, bipolar manic-depressive and schizoaffective disorders: results of a prospective longitudinal study [in German]. Fortschr Neurol Psychiatr Grenzgeb 1980; 48: 3–30
Keller MB, Kocsis JH, Thase ME, et al. Maintenance phase efficacy of sertraline for chronic depression: a randomized controlled trial. JAMA 1998; 280(19): 1665–72
Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 12 new-generation antide-pressants: a multiple treatments meta-analysis. Lancet 2009; 373(9665): 746–58
Posternak MA, Solomon DA, Leon AC, et al. The naturalistic course of unipolar major depression in the absence of somatic therapy. J Nerv Ment Dis 2006; 194(5): 324–9
Greden JF. Physical symptoms of depression: unmet needs. J Clin Psychiatry 2003; 64 Suppl. 7: 5–11
Judd LL, Paulus MJ, Schettler PS, et al. Does incomplete recovery from first lifetime major depressive episode herald a chronic course of illness? Am J Psychiatry 2000; 157: 1501–4
Frank E, Prien RF, Jarrett RB, et al. Conceptualization and rationale for consensus definitions of terms in major depressive disorder: remission, recovery, relapse, and recurrence. Arch Gen Psychiatry 1991; 48(9): 851–5
Gilaberte I, Montejo AL, de La Gandara J, et al., for the Fluoxetine Long-Term Study Group. Fluoxetine in the prevention of depressive recurrences: a double-blind study. J Clin Psychopharmacol 2001; 21: 417–24
American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder (revision): American Psychiatric Association. Am J Psychiatry 2000; 157(4 Suppl.): 1–45
Glue P, Donovan MR, Kolluri S, et al. Meta-analysis of relapse prevention antidepressant trials in depressive disorders. Aust N Z J Psychiatry 2010; 44(8): 697–705
Geddes JR, Carney SM, Davies C, et al. Relapse prevention with antidepressant drug treatment in depressive disorders: a systematic review. Lancet 2003; 361: 653–61
Brunoni AR, Fraguas R, Fregni F. Pharmacological and combined interventions for the acute depressive episode: focus on efficacy and tolerability. Ther Clin Risk Manag 2009; 5: 897–910
Viguera AC, Baldessarini RJ, Friedberg J. Discontinuing antidepressant treatment in major depression. Harv Rev Psychiatry 1998; 5: 293–306
Papakostas GA, Charles D, Fava M. Are typical starting doses of the selective serotonin reuptake inhibitors suboptimal? A meta-analysis of randomized, double-blind, placebo-controlled, dose-finding studies in major depressive disorder. World J Biol Psychiatry 2010; 11 (2 Pt 2): 300–7
Papakostas GA, Homberger CH, Fava M. A meta-analysis of clinical trials comparing mirtazapine with selective serotonin reuptake inhibitors for the treatment of major depressive disorder. J Psychopharmacol 2008; 22(8): 843–8
Sinyor M, Levitt AJ, Cheung AH, et al. Does inclusion of a placebo arm influence response to active antidepressant treatment in randomized controlled trials? Results from pooled and meta-analyses. J Clin Psychiatry 2010; 71(3): 270–9
Thase ME, Prichett YL, Ossanna MJ, et al. Efficacy of duloxetine and selective serotonin reuptake inhibitors: comparisons as assessed by remission rates in patients with major depressive disorder. J Clin Psychopharmacol 2007; 27(6): 672–6
Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry 2006; 163: 1905–17
Hennings JM, Owashi T, Binder EB, et al. Clinical characteristics and treatment outcome in a representative sample of depressed inpatients: findings from the Munich Antidepressant Response Signature (MARS) project. J Psychiatr Res 2009; 43(3): 215–29
Gitlin MJ, Abulseoud O, Frye MA. Improving the design of maintenance studies for bipolar disorder. Curr Med Res Opin 2010; 26(8): 1835–42
Hirschfeld RM. Clinical importance of long-term antidepressant treatment. Br J Psychiatry Suppl 2001; 42: S4–8
Warden D, Rush AJ, Trivedi MH, et al. The STAR*D project results: a comprehensive review of findings. Curr Psychiatry Rep 2007; 9(6): 449–59
Kane JM, Quitkin FM, Rifkin A, et al. Lithium carbonate and imipramine in the prophylaxis of unipolar and bipolar II illness: a prospective, placebo-controlled comparison. Arch Gen Psychiatry 1982; 39: 1065–9
Prien RF, Kupfer DJ, Mansky PA, et al. Drug therapy in the prevention of recurrences in unipolar and bipolar affective disorders: report of the NIMH Collaborative Study Group comparing lithium carbonate, imipramine, and a lithium carbonate-imipramine combination. Arch Gen Psychiatry 1984; 41: 1096–104
Frank E, Kupfer DJ, Perel JM, et al. Three-year outcomes of maintenance therapies in recurrent depression. Arch Gen Psychiatry 1990; 47: 1093–9
Kupfer DJ, Frank E, Perel JM, et al. Five-year outcome for maintenance therapies in recurrent depression. Arch Gen Psychiatry 1992; 49: 769–73
Glen AI, Johnson AL, Shepherd M. Continuation therapy with lithium and amitriptyline in unipolar depressive illness: a randomized, double-blind, controlled trial. Psychol Med 1984; 14: 37–50
Alexopoulos GS, Meyers BS, Young RC, et al. Executive dysfunction and long-term outcomes of geriatric depression. Arch Gen Psychiatry 2000; 57: 285–90
Reynolds III CF, Ellen F, Perel J, et al. Nortriptyline and interpersonal psychotherapy as maintenance therapies for recurrent major depression: a randomized controlled trial in patients older than 59 years. JAMA 1999; 281: 39–45
Old Age Depression Interest Group. How long should the elderly take antidepressants? A double-blind placebo-controlled study of continuation/prophylaxis therapy with dothiepin. Br J Psychiatry 1993; 162: 175–82
Kishimoto A, Mizukawa R, Matsuzaki F, et al. Prophylactic effect of mianserin on recurrent depression. Acta Psychiatr Scand 1994; 89: 46–51
Robinson DS, Lerfald S, Bennett B, et al. Continuation and maintenance treatment of major depression with the monoamine oxidase inhibitor phenelzine: a double-blind placebo-controlled discontinuation study. Psychopharmacol Bull 1991; 27: 31–9
Gilaberte I, Montejo AL, de la Gandara J, et al. Flouxetine in the prevention of depressive recurrences: a double-blind study. J Clin Psychopharmacol 2001; 21: 417–24
Doogan DP, Caillard V. Sertraline in the prevention of depression. Br J Psychiatry 1992; 160: 217–22
Wilson KCM, Mottram PG, Ashworth L, et al. Older community residents with depression: long-term treatment with sertraline. Br J Psychiatry 2003; 182: 492–7
Hochstrasser B, Isaksen PM, Koponen H, et al. Prophylactic effect of citalopram in unipolar recurrent depression: placebo-controlled study of maintenance therapy. Br J Psychiatry 2001; 178: 304–10
Reynolds III CF, Dew MA, Pollock BG, et al. Maintenance treatment of major depression in old age. N Engl J Med 2006; 354: 1130–8
Kocsis JH, Thase ME, Trivedi MH, et al. Prevention of recurrent episodes of depression with venlafaxine ER in a 1-year maintenance phase from the PREVENT study. J Clin Psychiatry 2007; 68: 1014–23
Keller MB, Trivedi MH, Thase ME, et al. The Prevention of Recurrent Episodes of depression with VENlafaxine for Two years (PREVENT) study: outcome from the 2-year and combined maintenance phases. J Clin Psychiatry 2007; 68: 1246–56
Segal ZV, Bieling P, Young T, et al. Antidepressant monotherapy vs sequential pharmacotherapy and mind-fulness-based cognitive therapy, or placebo, for relapse prophylaxis in recurrent depression. Arch Gen Psychiatry 2010; 67(12): 1256–64
Briscoe B, El-Mallakh RS. The evidence base for the long-term use of antidepressants as prophylaxis against future depressive episodes. Presented at the Annual Meeting of the American Psychiatric Association; 2010 May 24–26; New Orleans, (LA)
Greenhouse JB, Stangl D, Kupfer DJ, et al. Methodologic issues in maintenance therapy clinical trials. Arch Gen Psychiatry 1991; 48: 313–8
Lépine J-P, Caillard V, Bisserbe J-C, et al., for the PRE-VERS Investigators. A randomized, placebo-controlled trial of sertraline for prophylactic treatment of highly recurrent major depressive disorder. Am J Psychiatry 2004; 161: 836–42
Littrell J. Relationship between time since reuptake-blocker antidepressant discontinuation and relapse. Exp Clin Psychopharmacol 1994; 2(1): 82–94
Franks MA, Macritchie KA, Mahmood T, et al. Bouncing back: is the bipolar rebound phenomenon peculiar to lithium? A retrospective naturalistic study. J Psychopharmacol 2008; 22(4): 452–6
Schatzberg AF, Blier P, Delgado PL, et al. Antidepressant discontinuation syndrome: consensus panel recommendations for clinical management and additional research. J Clin Psychiatry 2006; 67 Suppl. 4: 27–30
Delgado PL. Monoamine depletion studies: implications for antidepressant discontinuation syndrome. J Clin Psychiatry 2006; 67 Suppl. 4: 22–6
Rosenbaum JF, Fava M, Hoog SL, et al. Selective serotonin reuptake inhibitor discontinuation syndrome: a randomized clinical trial. Biol Psychiatry 1998; 44(2): 77–87
Tint A, Haddad PM, Anderson IM. The effect of rate of antidepressant tapering on the incidence of discontinuation symptoms: a randomised study. J Psychopharmacol 2008; 22(3): 330–2
Baldessarini RJ, Tondo L, Ghiani C, et al. Illness risk following rapid versus gradual discontinuation of antidepressants. Am J Psychiatry 2010; 167(8): 934–41
Valuck RJ, Orton HD, Libby AM. Antidepressant discontinuation and risk of suicide attempt: a retrospective, nested case-control study. J Clin Psychiatry 2009; 70(8): 1069–77
Galbally M, Lewis AJ, Lum J, et al. Serotonin discontinuation syndrome following in utero exposure to antidepressant medication: prospective controlled study. Aust N Z J Psychiatry 2009; 43(9): 846–54
Hale TW, Kendall-Tackett K, Cong Z, et al. Discontinuation syndrome in newborns whose mothers took antidepressants while pregnant or breastfeeding. Breastfeed Med 2010; 5: 283–8
El-Mallakh RS, Roberts RJ, Swann A, et al. Tardive dysphoria: antidepressant-induced chronic depression. Irish J Psychol Med. In press
El-Mallakh RS, Gao Y, Roberts RJ. Tardive dysphoria: the role of long term antidepressant use in inducing chronic depression. Med Hypotheses 2011; 76(6): 769–73
Meshul CK, Casey DE. Regional, reversible ultrastructural changes in rat brain with chronic neuroleptic treatment. Brain Res 1989; 489: 338–46
El-Mallakh RS, Peters C, Waltrip C. Antidepressant treatment and neural plasticity. J Child Adoles Psychopharmacol 2000; 10: 287–94
Getz A, Xu F, Zaidi W, et al. The antidepressant fluoxetine but not citalopram suppresses synapse formation and synaptic transmission between Lymnaea neurons by perturbing presynaptic and postsynaptic machinery. Eur J Neurosci 2011; 34(2): 221–34
Djordjevic A, Djordjevic J, Elaković I, et al. Fluoxetine affects hippocampal plasticity, apoptosis and depressive-like behavior of chronically isolated rats. Prog Neuropscyhopharmacol Biol Psychiatry 2012 Jan 10; 36(1): 92–100
Homberg JR, Olivier JD, Blom T, et al. Fluoxetine exerts age-dependent effects on behavior and amygdala neuro-plasticity in the rat. PLoS One 2011; 6(1): e16646
Wang Y, Neumann M, Hansen K, et al. Fluoxetine increases hippocampal neurogenesis and induces epigenetic factors but does not improve functional recovery after traumatic brain injury. J Neurotrauma 2011; 28(2): 259–68
Bessa JM, Ferreira D, Melo I, et al. The mood-improving actions of antidepressants do not depend on neurogenesis but are associated with neuronal remodeling. Mol Psychiatry 2009; 14(8): 764–73
Acknowledgements
Dr Briscoe does not have any conflicts of interest to report. Over the last 5 years, Dr El-Mallakh has received honoraria for being on the speakers’ bureau of the following pharmaceutical companies: Angelini Labopharm, AstraZeneca, Bristol Myers Squibb, Lilly, Merck, Novartis and Pfizer. There are no other conflict of interests to report. This preparation of this review was not supported by any extramural funds.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
El-Mallakh, R.S., Briscoe, B. Studies of Long-Term Use of Antidepressants. CNS Drugs 26, 97–109 (2012). https://doi.org/10.2165/11599450-000000000-00000
Published:
Issue Date:
DOI: https://doi.org/10.2165/11599450-000000000-00000