
Abstract
▴ Certolizumab pegol is a PEGylated humanized Fab′ monoclonal antibody that targets and neutralizes both membrane-bound and soluble tumor necrosis factor (TNF)-α, preventing inflammation and consequently the destruction of cartilage and bone. Certolizumab pegol has a relatively long elimination half-life of ≈2 weeks, allowing subcutaneous administration once every 2 or 4 weeks.
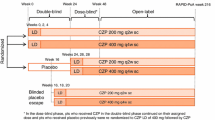
▴ In two randomized, phase III trials in patients with active rheumatoid arthritis despite previous methotrexate therapy (RAPID 1 and 2), the combination of subcutaneous certolizumab pegol 400 mg at weeks 0, 2, and 4, followed by a 200 or 400 mg dose every 2 weeks and a stable dosage of methotrexate, was more effective than placebo plus methotrexate for improving the signs and symptoms of arthritis at weeks 24 (RAPID 1 and 2) and 52 (RAPID 1), according to American College of Rheumatology (ACR) criteria. Improvements in ACR response rates were seen as early as 1 week and at all timepoints measured up to 52 weeks.
▴ In RAPID 1 and RAPID 2, radiographic progression was also significantly inhibited with certolizumab pegol plus methotrexate treatment compared with placebo and methotrexate according to van der Heijde modified Total Sharp Scores at 24 and 52 weeks after treatment initiation.
▴ In patients with active rheumatoid arthritis who had previously failed to respond to treatment with ≥1 disease-modifying anti-rheumatic drug, certolizumab pegol 400 mg every 4 weeks as monotherapy effectively improved ACR responses at all measured timepoints up to 24 weeks, according to data from the randomized, phase III FAST4WARD trial.
▴ Certolizumab pegol was generally well tolerated in combination with methotrexate or as monotherapy in phase III trials in patients with rheumatoid arthritis, with most adverse events being of mild to moderate intensity. Infections were the most frequently reported adverse events.



Similar content being viewed by others


References
Scott DL, Kingsley GH. Tumor necrosis factor inhibitors for rheumatoid arthritis. N Engl J Med 2006 Aug 17; 355(7): 704–12
National Institute for Health and Clinical Excellence. Rheumatoid arthritis: a national clinical guideline for management and treatment in adults [online]. Available from URL: http://www.nice.org.uk/nicemedia/pdf/CG79FullGuideline.pdf [Accessed 2009 Jul 3]
Osterhaus JT, Purcaru O, Richard L. Discriminant validity, responsiveness and reliability of the rheumatoid arthritis-specific Work Productivity Survey (WPS-RA). Arthritis Res Ther 2009 May 20; 11(3): R73
Klinkhoff A. Biological agents for rheumatoid arthritis: targeting both physical function and structural damage. Drugs 2004; 64(12): 1267–83
Voll RE, Kalden JR. Do we need new treatment that goes beyond tumor necrosis factor blockers for rheumatoid arthritis? Ann N Y Acad Sci 2005 Jun; 1051: 799–810
Fleischmann R, Iqbal I, Nandeshwar P, et al. Safety and efficacy of disease-modifying anti-rheumatic agents: focus on the benefits and risks of etanercept. Drug Saf 2002; 25(3): 173–97
Weaver AL. The impact of new biologicals in the treatment of rheumatoid arthritis. Rheumatology (Oxford) 2004 Jun; 43Suppl. 3: iii17–23
Oldfield V, Plosker GL. Golimumab: in the treatment of rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis. Biodrugs 2009; 23(2): 125–35
Jazayeri JA, Carroll GJ. Fc-based cytokines: prospects for engineering superior therapeutics. Biodrugs 2008; 22(1): 11–26
Mohler KM, Murray KM, Mann DL, et al. Use of targeted anticytokine treatments in heart failure. Circulation 2000 Aug 29; 102(9): E65
Tracey D, Klareskog L, Sasso EH, et al. Tumor necrosis factor antagonist mechanisms of action: a comprehensive review. Pharmacol Ther 2008 Feb; 117(2): 244–79
Veronese FM, Mero A. The impact of PEGylation on biological therapies. Biodrugs 2008; 22(5): 315–29
Bourne T, Fossati G, Nesbitt A. A PEGylated Fab′ fragment against tumor necrosis factor for the treatment of Crohn disease: exploring a new mechanism of action. Biodrugs 2008; 22(5): 331–7
Cimzia™ (certolizumab pegol): US prescribing information. Georgia: UCB, Inc. [online]. Available from URL: http://www.cimzia.com/crohnsdisease/pdf/Prescribing_Information.pdf [Accessed 2009 May 14]
Blick SK, Curran MP. Certolizumab pegol: in Crohn's disease. Biodrugs 2007; 21(3): 195–201
UCB. UCBs Cimzia™ (certolizumab pegol) approved by Health Canada for adult patients suffering from moderate to severe rheumatoid arthritis [online]. Available from URL: http://smr.newswire.ca/en/ucb-canada-inc [Accessed 2009 Oct 15]
European Medicines Agency. Cimzia 200 mg solution for injection: summary of product characteristics [online]. Available from URL: http://www.emea.europa.eu/humandocs/PDFs/EPAR/cimzia/emea-combined-h1037en.pdf [Accessed 2009 Oct 28]
Nesbitt A, Fossati G, Bergin M, et al. Mechanism of action of certolizumab pegol (CDP870): in vitro comparison with other anti-tumor necrosis factor alpha agents. Inflamm Bowel Dis 2007 Nov; 13(11): 1323–32
Choy EH, Hazleman B, Smith M, et al. Efficacy of a novel PEGylated humanized anti-TNF fragment (CDP870) in patients with rheumatoid arthritis: a phase II double-blinded, randomized, dose-escalating trial. Rheumatology (Oxford) 2002 Oct; 41(10): 1133–7
Keystone E, Heijde D, Mason Jr D, et al. Certolizumab pegol plus metho-trexate is significantly more effective than placebo plus methotrexate in active rheumatoid arthritis: findings of a fifty-two-week, phase III, multicenter, randomized, double-blind, placebo-controlled, parallel-group study. Arthritis Rheum 2008 Nov; 58(11): 3319–29
Smolen JS, Landewe RB, Mease PJ, et al. Efficacy and safety of certolizumab pegol plus methotrexate in active rheumatoid arthritis: the RAPID 2 study -a randomised controlled trial. Ann Rheum Dis 2009 Jun; 68(6): 797–804
Fleischmann R, Vencovsky J, van Vollenhoven R, et al. Efficacy and safety of certolizumab pegol monotherapy every 4 weeks in patients with rheumatoid arthritis failing previous disease-modifying antirheumatic therapy: the FAST4WARD study. Ann Rheum Dis 2008 Nov 17; 68: 805–11
Parton T, King L, Parker G, et al. The PEG moiety of certolizumab pegol is rapidly cleared from the blood of humans by the kidneys once it is cleaved from the Fab′ [abstract no. THU0051]. Ann Rheum Dis 2009; 68Suppl. 3: 189
Barnes T, Moots R. Targeting nanomedicines in the treatment of rheumatoid arthritis: focus on certolizumab pegol. Int J Nanomed 2007; 2(1): 3–7
Kavanaugh A, Smolen JS, Emery P, et al. Effect of certolizumab pegol with methotrexate on home and workplace productivity and social activities in patients with active rheumatoid arthritis. Arthritis Care Res 2009; 61(11): 1592–600
Acknowledgments and Disclosures
The manuscript was reviewed by: R.M. Fleischmann, Department of Internal Medicine, University of Texas Southwestern Medical Center, Dallas, Texas, USA; A.J. Gstör, Department of Rheumatology, Addenbrooke’s Hospital, Cambridge, UK.
The preparation of this review was not supported by any external funding. During the peer review process, the manufacturer of the agent under review was offered an opportunity to comment on this article. Changes resulting from comments received were made on the basis of scientific and editorial merit.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Duggan, S.T., Keam, S.J. Certolizumab Pegol. BioDrugs 23, 407–417 (2009). https://doi.org/10.2165/11202800-000000000-00000
Published:
Issue Date:
DOI: https://doi.org/10.2165/11202800-000000000-00000