
Abstract
Objectives
To quantify the impact of clopidogrel plus aspirin on the individual outcomes of death, myocardial infarction, or stroke in patients with established cardiovascular disease, or in patients with multiple risk factors for vascular disease.
Background
Randomized trials have demonstrated a reduction in composite outcomes when clopidogrel is added to aspirin therapy in patients with coronary artery disease; however, the magnitude of benefit on individual outcomes is unknown.
Methods
We conducted a meta-analysis on randomized, controlled trials that compared aspirin plus clopidogrel with aspirin plus placebo for the treatment of coronary artery disease.
Results
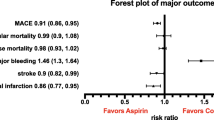
This analysis included five randomized trials (CURE, CREDO, CLARITY, COMMIT, and CHARISMA) in 79 624 patients. The incidence of all-cause mortality was 6.3% in the aspirin plus clopidogrel group versus 6.7% in the aspirin group (odds ratio [OR] 0.94; 95% CI 0.89, 0.99; p = 0.026). The incidence of myocardial infarction was 2.7% and 3.3% (OR 0.82; 95% CI 0.75, 0.89; p < 0.0001), and stroke was 1.2% and 1.4% (OR 0.82; 95% CI 0.73, 0.93; p = 0.002). Similarly, the incidence of major bleeding was 1.6% and 1.3% (OR 1.26; 95% CI 1.11, 1.41; p < 0.0001), and fatal bleeding was 0.28% and 0.27% (OR 1.04; 95% CI 0.76, 1.43; p = 0.79).
Conclusion
The addition of clopidogrel to aspirin results in a small reduction in all-cause mortality in patients with ST-elevation myocardial infarction and a modest reduction in myocardial infarction and stroke in patients with cardiovascular disease. The overall incidence of major bleeding however is increased, although there is no excess of fatal bleeds or hemorrhagic strokes.









Similar content being viewed by others

References
Lewis Jr HD, Davis JW, Archibald DG, et al. Protective effects of aspirin against acute myocardial infarction and death in men with unstable angina: results of a Veterans Administration Cooperative Study. N Engl J Med 1983; 309: 396–403.
Antiplatelet Trialists’ Collaboration. Collaborative overview of randomised trials of antiplatelet therapy: I. Prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in various categories of patients. BMJ 1994; 308: 81–106.
The PURSUIT Trial Investigators. Inhibition of platelet glycoprotein IIb/IIIa with eptifibatide in patients with acute coronary syndromes: platelet glycoprotein IIb/IIIa in unstable angina. Receptor suppression using integrilin therapy. N Engl J Med 1998; 339: 436–43.
Yusuf S, Zhao F, Mehta SR, et al. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med 2001; 345: 494–502.
Steinhubl SR, Berger PB, Mann 3rd JT, et al. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. JAMA 2002; 288: 2411–20.
Sabatine MS, Cannon CP, Gibson CM, et al. Addition of clopidogrel to aspirin and fibrinolytic therapy for myocardial infarction with ST-segment elevation. N Engl J Med 2005; 352: 1179–89.
Chen ZM, Jiang LX, Chen YP, et al. Addition of clopidogrel to aspirin in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet 2005; 366: 1607–21.
Bhatt DL, Fox KA, Hacke W, et al. Clopidogrel for and aspirin versus aspirin alone for the prevention of atherothrombotic events (CHARISMA) trial. N Engl J Med 2006; 354: 1706–17.
Bavry AA, Kumbhani DJ, Helton TJ, et al. Late thrombosis of drug-eluting stents: a meta-analysis of randomized clinical trials. Am J Med 2006; 11: 1056–61.
Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA 2005; 293: 2126–30.
Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA guidelines for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Unstable Angina). J Am Coll Cardiol 2000; 36: 970–1062.
Bovill EG, Terrin ML, Stump DC, et al. Hemorrhagic events during therapy with recombinant tissue-type plasminogen activator, heparin, and aspirin for acute myocardial infarction. Results of the Thrombolysis in Myocardial Infarction (TIMI), Phase II Trial. Ann Intern Med 1991; 115: 256–65.
CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). Lancet 1996; 348: 1329–39.
Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet 2004; 364: 331–7.
Bertrand ME, Rupprecht HJ, Urban P, et al. Double-blind study of the safety of clopidogrel with and without a loading dose in combination with aspirin compared with ticlopidine in combination with aspirin after coronary stenting: the clopidogrel aspirin stent international cooperative study (CLASSICS). Circulation 2000; 102: 624–9.
Hall P, Nakamura S, Maiello L, et al. A randomized comparison of combined ticlopidine and aspirin therapy versus aspirin therapy alone after successful intravascular ultrasound-guided stent implantation. Circulation 1996; 93: 215–22.
Juergens CP, Wong AM, Leung DY, et al. A randomized comparison of clopidogrel and aspirin versus ticlopidine and aspirin after coronary stent implantation. Am Heart J 2004; 147: E15.
Machraoui A, Germing A, Lindstaedt M, et al. Efficacy and safety of ticlopidine monotherapy versus ticlopidine and aspirin after coronary artery stenting: follow-up results of a randomized study. J Invasive Cardiol 2001; 13: 431–6.
Muller C, Buttner HJ, Petersen J, et al. A randomized comparison of clopidogrel and aspirin versus ticlopidine and aspirin after the placement of coronary-artery stents. Circulation 2000; 101: 590–3.
Scrutinio D, Cimminiello C, Marubini E, et al. Ticlopidine versus aspirin after myocardial infarction (STAMI) trial. J Am Coll Cardiol 2001; 37: 1259–65.
Van de Loo A, Nauck M, Noory E, et al. Enhancement of platelet inhibition of ticlopidine plus aspirin vs aspirin alone given prior to elective PTCA. Eur Heart J 1998; 19: 96–102.
GUSTO Investigators. An International randomized trial comparing four thrombolytic strategies for acute myocardial infarction. N Engl J Med 1993; 329: 673–82.
Rothberg M. Cost-effectiveness of clopidogrel plus aspirin versus aspirin alone [letter]. Ann Intern Med 2005; 143: 464.
Califf RM, DeMets DL. Principles from clinical trials relevant to clinical practice: part I. Circulation 2002; 106: 1015–21.
Peters RJ, Mehta SR, Fox KA, et al. Effects of aspirin dose when used alone or in combination with clopidogrel in patients with acute coronary syndromes: observations from the Clopidogrel in Unstable angina to prevent Recurrent Events (CURE) study. Circulation 2003; 108: 1682–7.
Bavry AA, Lincoff AM. Is clopidogrel cardiovascular medicine’s double edged sword? Circulation 2006; 113: 1638–40.
Fox KA, Mehta SR, Peters R, et al. Benefits and risks of the combination of clopidogrel and aspirin in patients undergoing surgical revascularization for non-ST-elevation acute coronary syndrome: the Clopidogrel in Unstable angina to prevent Recurrent ischemic Events (CURE) Trial. Circulation 2004; 110: 1202–8.
Acknowledgments
Dr Bhatt was the primary investigator for the CHARISMA study and received research grants from both Bristol Myers Squib (New York, USA) and Sanofi Aventis (Paris, France). He was also the co-primary investigator on the LANCELOT and CHAMPION studies and received research grants from Eisai (Woodcliff Lake, NJ, USA) and The Medicines Company (Parsippany, NJ, USA), respectively. All research grant funds were given directly to the institution (Cleveland Clinic) and not to Dr Bhatt personally, for the above studies.
In addition, Dr Bhatt has received within the past 5 years honoraria for consulting on scientific advisory boards and lecture fees from both Sanofi Aventis (Paris, France) and Bristol Myers Squibb (New York, USA), the makers of clopidogrel and honoraria for consulting on scientific advisory boards from Astra Zeneca (Wilmington, DE, USA) and Eli Lilly (Indianapolis, IN, USA), who are aiming to develop compounds similar to clopidogrel. In addition, in the past 5 years Dr Bhatt has received honoraria for consulting on scientific advisory boards and lecture fees from The Medicines Company, and honoraria for consulting on scientific advisory boards from Millennium (Cambridge, MA, USA) and Schering Plough (Kenilworth, NJ, USA), all of whom are involved in developing antiplatelet compounds. He has also received honoraria for consulting on scientific advisory boards from Centocor (Horsham, PA, USA), Daiichi-Sankyo (Parsippany, NJ, USA), Eisai (Woodcliff Lake, NJ, USA), Glaxo Smith Kline (Philadelphia, PA, USA), Otsuka (Rockville, MD, USA), Paringenix (Tucson, AZ, USA), and PDL (Fremont, CA, USA). Finally, Dr Bhatt has provided expert testimony regarding clopidogrel (the compensation was donated to a non-profit organization).
Dr Bavry has received honoraria from consulting with Genesis Associates, HRA, The Frankel Group (New York, USA), Propagate Pharma (Surrey, Enland) and Hagen/Sinclair Research Recruiting (Santa Rosa, CA, USA) for an amount of <$US10 000.
Drs Helton, Roukoz, and Duggal have no potential conflicts of interest to disclose.
No sources of funding were used in the preparation of the current meta-analysis. This manuscript represents original work of the authors and is not under consideration elsewhere. None of the paper’s contents have been previously published but results were presented as an oral abstract at the American Heart Association Scientific Sessions on 14 November 2006 in Chicago (IL).
The authors do meet criteria for authorship and accept responsibility for scientific content of the manuscript. Dr Helton designed the study, abstracted and analyzed the data, and drafted the manuscript. Drs Bavry, Kumbhani, and Bhatt were involved in the design of the study, analyzed the data and revised the manuscript. Drs Duggal and Roukoz abstracted and analyzed the data and revised the manuscript. All authors have read and approved the final version of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Helton, T.J., Bavry, A.A., Kumbhani, D.J. et al. Incremental Effect of Clopidogrel on Important Outcomes in Patients with Cardiovascular Disease. Am J Cardiovasc Drugs 7, 289–297 (2007). https://doi.org/10.2165/00129784-200707040-00006
Published:
Issue Date:
DOI: https://doi.org/10.2165/00129784-200707040-00006