
Abstract
Background and objective
In day-to-day practice, asthma treatment and self-management often fall short of the objectives defined by clinical practice guidelines. The objective of this study was to determine whether a population-based asthma disease management program, using broad-based educational interventions, can have a favorable impact on physician and patient adherence to guidelines-based care.
Methods
A longitudinal, before-and-after design was used to evaluate program impacts on pharmacotherapy and health status. Patients with asthma (n = 35 450) were enrolled in the program from September 2000 through to June 2001. Patients were identified for the study based on a 12-month retrospective analysis of pharmacy claims. Patients were members of prescription benefit plans managed by Medco Health and were aged 5 years and older. Patients in the intervention group received asthma education materials during the 12-month period following enrollment. The materials emphasized guidelines-based principles of asthma pharmacotherapy, self-management, trigger avoidance and patient-physician partnership. Physicians received guidelines-based flow sheets to facilitate therapy tracking, and pharmacotherapy review. Asthma drug utilization was measured during the 12-month period prior to enrollment and the 12-month period following enrollment. Utilization data on controller and reliever medications were derived from a pharmacy claims database. Drug utilization changes for the intervention group were compared with those for matched controls. A health survey was conducted on a random sample of program participants at enrollment and at 12-month follow-up. The health survey included questions on asthma-related quality of life (QOL), medical utilization, productivity, and self-management skills.
Main outcome measures and results
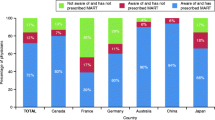
The percentage of patients who started controller therapy during the study period was significantly higher for the intervention group than the control group (20.7% versus 18.1%, p < 0.001). The controller prescription fill rate increased significantly in the intervention group compared with controls (p < 0.0001); the increase was primarily driven by increased refill rates for patients already using controllers. Reliever prescription fill rates decreased for both the intervention group and controls. Program participants reported significant improvements in asthma-related QOL (p < 0.05) and self-management skills. Self-reported medical utilization decreased for office visits (p < 0.05) and emergency room visits (p < 0.01).
Conclusions
A population-based asthma disease management program can improve controller prescribing rates (new therapy starts), controller adherence rates (refill persistency), and self-management skills. These changes in physician and patient behavior help close the gaps between guidelines and practice in asthma therapy.






Similar content being viewed by others


References
American Lung Association, Epidemiology and Statistics Unit. Trends in asthma morbidity and mortality. New York (NY): American Lung Association, 2003 Mar
National Heart, Lung, and Blood Institute. Morbidity and mortality: 2002 chart book on cardiovascular, lung, and blood diseases. Bethesda (MD): National Institutes of Health, 2002 May
National Asthma Education and Prevention Program (NAEPP). Guidelines for the diagnosis and management of asthma. Bethesda, (MD): National Institutes of Health, National Heart, Lung, and Blood Institute, 1997 Apr: NIH publication 97-4051
British Thoracic Society, British Paediatric Association, Research Unit of the Royal College of Physicians of London, et al. Guidelines on the management of asthma. Thorax 1993; 48 (2 Suppl.): S1–24
Global Initiative for Asthma. Asthma management and prevention: a practical guide for public health officials and health care professionals. Bethesda (MD): National Institutes of Health, National Heart, Lung, and Blood Institute, and World Health Organization, 1995 Dec: NIH publication 96-3659A
National Asthma Education Program (NAEP). Guidelines for the diagnosis and management of asthma. Bethesda (MD): National Institutes of Health, National Heart, Lung, and Blood Institute, 1991: NIH publication 91-3042
National Asthma Education and Prevention Program (NAEPP). NAEPP expert panel report: guidelines for the diagnosis and management of asthma: update on selected topics 2002. Bethesda (MD): National Institutes of Health, National Heart, Lung, and Blood Institute, 2002 Jul: NIH publication 02-5075
Haahtela T, Jarvinen M, Kava T, et al. Comparison of a beta-agonist, terbutaline, with an inhaled corticosteroid, budesonide, in newly detected asthma. N Engl J Med 1991; 325: 388–92
Van Essen-Zandvliet EE, Hughes MD, Waalkens HJ, et al. Effects of 22 months of treatment with inhaled corticosteroids and/or beta-2-agonists on lung function, airway responsiveness, and symptoms in children with asthma. Am Rev Respir Dis 1992; 146: 547–54
Donahue JG, Weiss ST, Livingston JM, et al. Inhaled steroids and the risk of hospitalization for asthma. JAMA 1997; 277: 887–91
Balkrishnan R, Norwood GJ, Anderson A. Outcomes and cost benefits associated with the introduction of inhaled corticosteroid therapy in a Medicaid population of asthmatic patients. Clin Ther 1998; 20(3): 567–80
Suissa S, Ernst P. Inhaled corticosteroids: impact on asthma morbidity and mortality. J Allergy Clin Immunol 2001; 107: 937–44
Legorreta AP, Christian-Herman J, O’Connor RD, et al. Compliance with national asthma management guidelines and specialty care: a health maintenance organization experience. Arch Intern Med 1998; 158: 457–64
Diette GB, Wu AW, Skinner EA, et al. Treatment patterns among adult patients with asthma: factors associated with overuse of inhaled beta-agonists and underuse of inhaled corticosteroids. Arch Intern Med 1999; 159: 2697–704
Bousquet J, Knani J, Henry C, et al. Undertreatment in a nonselected population of adult patients with asthma. J Allergy Clin Immunol 1996; 98: 514–21
Hartert TV, Windom HH, Peebles Jr RS, et al. Inadequate outpatient medical therapy for patients with asthma admitted to two urban hospitals. Am J Med 1996; 100: 386–94
Lauman JM, Bjornson DC. Treatment of Medicaid patients with asthma: comparison with treatment guidelines using disease-based drug utilization review methodology. Ann Pharmacother 1998; 32: 1290–4
Taylor DM, Auble TE, Calhoun WJ, et al. Current outpatient management of asthma shows poor compliance with international consensus guidelines. Chest 1999; 116: 1638–44
Sullivan SD, Kreling DH, Hazlet TK. Noncompliance with medication regimens and subsequent hospitalizations: a literature analysis and cost of hospitalization estimate. J Res Pharm Econ 1990; 2(2): 19–33
Bender B, Milgrom H, Rand C. Nonadherence in asthmatic patients: is there a solution to the problem? Ann Allergy Asthma Immunol 1997; 79: 177–86
Salmeron S, Liard R, Elkharrat D, et al. Asthma severity and adequacy of management in accident and emergency departments in France: a prospective study. Lancet 2001; 358: 629–35
Bailey WC, Richards Jr JM, Brooks CM, et al. A randomized trial to improve self-management practices of adults with asthma. Arch Intern Med 1990; 150: 1664–8
Wilson SR, Scamagas P, German DF, et al. A controlled trial of two forms of self-management education for adults with asthma. Am J Med 1993; 94: 564–76
Kotses H, Bernstein IL, Bernstein DI, et al. A self-management program for adult asthma: Part I. development and evaluation. J Allergy Clin Immunol 1995; 95: 529–40
Boulet L-P, Boutin H, Cote J, et al. Evaluation of an asthma self-management education program. J Asthma 1995; 32(3): 199–206
Cote J, Cartier A, Robichaud P, et al. Influence on asthma morbidity of asthma education programs based on self-management plans following treatment optimization. Am J Respir Crit Care Med 1997; 155: 1509–14
Buchner DA, Butt LT, De Stefano A, et al. Effects of an asthma management program on the asthmatic member: patient-centered results of a 2-year study in a managed care organization. Am J Manag Care 1998; 4: 1288–97
Legorreta AP, Leung K-M, Berkbigler D, et al. Outcomes of a population-based asthma management program: quality of life, absenteeism, and utilization. Ann Allergy Asthma Immunol 2000; 85: 28–34
Feifer RA, Gutierrez B, Verbrugge RR. Impacts of a PBM-based disease management program on asthma medication use. J Manag Care Pharm 2001; 7(6): 460–7
Suh D-C, Shin S-K, Okpara I, et al. Impact of a targeted asthma intervention program on treatment costs in patients with asthma. Am J Manag Care 2001; 7: 897–906
Algatt-Bergstrom PJ, Markson LE, Murray RK, et al. A population-based approach to asthma disease management. Dis Manag Health Outcomes 2000; 7(4): 179–86
Groban MD, Evans RM, Edgren B, et al. Clinical benefits and cost reduction associated with a comprehensive asthma management programme at a managed care organisation. Dis Manag Health Outcomes 1998; 4(2): 93–100
D’Agostino Jr RB. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat Med 1998; 17: 2265–81
Dehejia RH, Wahba S. Propensity score matching methods for non-experimental causal studies. Cambridge (MA): National Bureau of Economic Research, 1998: NBER Working Paper 6829
Ad Hoc Committee on Health Literacy for the Council on Scientific Affairs, American Medical Association. Health literacy: report of the Council on Scientific Affairs. JAMA 1999; 281: 552–7
Juniper EF, Guyatt GH, Cox FM, et al. Development and validation of the mini asthma quality of life questionnaire. Eur Respir J 1999; 14(1): 32–8
National Center for Health Statistics, Centers for Disease Control and Prevention. 1999 National Health Interview Survey, Version 99.1 [online]. Available from URL: http://www.cdc.gov/nchs/nhis.htm [Accessed 2003 Nov 21]
Ungar WJ, Coyte PC, Pharmacy Medication Monitoring Program Advisory Board. Measuring productivity loss days in asthma patients. Health Econ 2000; 9: 37–46
Acknowledgements
This study evaluates the outcomes of a disease management program offered by Medco Health with financial support from Integrated Therapeutics Group (ITG), a subsidiary of Schering-Plough Corporation. The authors would like to thank the following individuals for their contributions during the development and evaluation of this program: Berhanu Alemayehu, Stacy Ferrari, Les Paul, and Melinda Thiel. The authors have no conflicts of interest directly relevant to the content of this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Feifer, R.A., Verbrugge, R.R., Khalid, M. et al. Improvements in Asthma Pharmacotherapy and Self-Management. Dis-Manage-Health-Outcomes 12, 93–102 (2004). https://doi.org/10.2165/00115677-200412020-00003
Published:
Issue Date:
DOI: https://doi.org/10.2165/00115677-200412020-00003