
Abstract
Objective
To present the pattern of self-report and diagnosis of erectile dysfunction in the US over the time period 1990 through 1998 and examine whether the introduction of sildenafil in March 1998 influenced these findings.
Study design and methods
Retrospective database analysis. Data from the National Ambulatory Medical Care Survey (NAMCS) for the years 1990 through 1998 were used. Data from office-based physician-patient encounters for which either a complaint of erectile dysfunction as one of the reasons for requesting an encounter [National Center for Health Statistics (NCHS) code 1160.3] or a diagnosis of erectile dysfunction [International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) code 302.72 or 607.84] was documented were extracted for men aged ≥40 years. National estimates per year were derived for: (i) the number of office-based physician-patient encounters for which a complaint of erectile dysfunction was documented as a reason for requesting an encounter and the number of office-based physician-patient encounters for which a diagnosis of erectile dysfunction was documented; (ii) the rate per 1000 office-based physician-patient encounters for which a complaint of erectile dysfunction as a reason for requesting the encounter was documented and the rate per 1000 office-based physician-patient encounters for which a diagnosis of erectile dysfunction was documented; and (iii) the rate per 1000 US male population aged ≥40 years with a complaint of erectile dysfunction as a reason for requesting an encounter and the rate per 1000 US male population aged ≥40 years with a diagnosis of erectile dysfunction.
Results
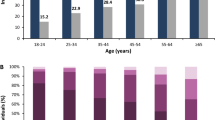
The number of office-based physician-patient encounters for which a complaint of erectile dysfunction was documented increased from 764 682 in 1990 to 1 273 730 in 1998. The number of office-based physician-patient encounters with a recorded diagnosis of erectile dysfunction more than doubled over the time period examined, from 647 418 in 1990 to 1 495 793 in 1998. Office-based encounters for which a complaint of erectile dysfunction was documented as a reason for requesting an appointment increased from 5.7 per 1000 in 1990 to 7.0 per 1000 in 1998; the rate of diagnosis of erectile dysfunction increased from 4.8 per 1000 in 1990 to 8.2 per 1000 in 1998. The population-adjusted rate of complaint of erectile dysfunction increased from 17.5 per 1000 in 1990 to 24.2 per 1000 in 1998; the rate of diagnosis increased from 14.9 per 1000 in 1990 to 28.4 per 1000 in 1998. In 1998, 2 142 776 office-based physician-patient encounters documented the prescribing of sildenafil; of these, 41% were for patients with a recorded diagnosis of erectile dysfunction.
Conclusions
The introduction of sildenafil was found not to have influenced the established upward trend in the documented rate of self-report of erectile dysfunction or the diagnosis of erectile dysfunction. However, the prescribing of sildenafil appears to offer greater insight into the actual magnitude of the problem erectile dysfunction represents in the US. Findings suggest there is a reluctance on the part of patients to discuss concerns about erectile dysfunction with their physician and a reluctance on the part of physicians to document patients’ expressed concerns regarding erectile dysfunction and/or to record a diagnosis of erectile dysfunction.






Similar content being viewed by others


References
Benet AE, Melman A. The epidemiology of erectile dysfunction. Urol Clin North Am 1995; 22: 699–709
Feldman HA, Goldstein I, Hatzichristou DG, et al. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol 1994; 151: 54–61
NIH Consensus Development Panel on Impotence. NIH Consensus Conference: impotence. JAMA 1993; 270: 83–90
Cappelleri JC, Rosen RC, Smith MD, et al. Diagnostic evaluation of the erectile function domain of the International Index of Erectile Function. Urology 1999; 54: 346–51
Lue T. Impotence: a patient’s goal-directed approach to treatment. World J Urol 1990; 8: 67–74
Schiavi RC, White D, Mandeli J, et al. Effect of testosterone administration on sexual behavior and mood in men with erectile dysfunction. Arch Sex Behav 1997; 26: 231–41
Price DE, Gingell JC, Gepi-Attee S, et al. Sildenafil: study of a novel oral treatment for erectile dysfunction in diabetic men. DiabetMed 1998; 15:821–5
Morales A, Gingell C, Collins M, et al. Clinical safety of oral sildenafil citrate (VIAGRA) in the treatment of erectile dysfunction. Int J Impot Res 1998; 10: 69–73
Lue TF. Erectile dysfunction. N Engl J Med 2000; 342: 1802–13
Kaiser FE, Viosca SP, Morley JE, et al. Impotence and aging: clinical and hormonal factors. J Am Geriatr Soc 1988; 36: 511–9
Spector IP, Carey MP. Incidence and prevalence of the sexual dysfunctions: a critical review of the empirical literature. Arch Sex Behav 1990; 19: 389–408
Fugl-Meyer AR, Lodnert G, Branholm IB, et al. On life satisfaction in male erectile dysfunction. Int J Impot Res 1997; 9: 141–8
National Center for Health Statistics. 1990 summary: National Ambulatory Medical Care Survey, United States. Advance data from Vital Health Stat; no. 213. Hyattsville (MD): National Center for Health Statistics, 1992
Schappert SM. National Ambulatory Medical Care Survey, 1991 summary. National Center for Health Statistics. Vital Health Stat 1994; 13: 1–110
Schappert SM. National Ambulatory Medical Care Survey, 1992 summary. Advance data from Vital Health Stat; no. 253. Hyattsville (MD): National Center for Health Statistics, 1994
Woodwell DW, Schappert SM. National Ambulatory Medical Care Survey, 1993 summary. Advance data from Vital Health Stat; no. 270. Hyattsville (MD): National Center for Health Statistics, 1995
Schappert SM. National Ambulatory Medical Care Survey, 1994 summary. Advance data from Vital Health Stat; no. 273. Hyattsville (MD): National Center for Health Statistics, 1996
Woodwell DA. National Ambulatory Medical Care Survey, 1995 summary. Advance data from Vital Health Stat; no. 286. Hyattsville (MD): National Center for Health Statistics, 1997
Woodwell DA. National Ambulatory Medical Care Survey, 1996 summary. Advance data from Vital Health Stat; no. 295. Hyattsville (MD): National Center for Health Statistics, 1997
Woodwell DA. National Ambulatory Medical Care Survey, 1997 summary. Advance data from Vital Health Stat; no. 305. Hyattsville (MD): National Center for Health Statistics, 1999
Woodwell DA. National Ambulatory Medical Care Survey, 1998 summary. Advance data from Vital Health Stat; no. 315. Hyattsville (MD): National Center for Health Statistics, 2000
Bryant E, Shimizu I. Sampling design, sampling variance, and estimation procedures for the National Ambulatory Medical Care Survey. National Center for Health Statistics, Vital Health Stat 1988; 2: 1–39
US Public Health Service and Health Care Financing Administration. International classification of diseases, 9th revision, clinical modification, volume 1. DHHS publication no. (PHS) 89–1260. Washington, DC: Public Health Service, 1989
Schneider D, Appleton L, McLemore T. A reason for visit classification for ambulatory care. National Center for Health statistics. Vital Health Stat 1979; 2(78): 1–63
Instruction manual: reason for visit classification and coding manual, 1994. National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey. Hyattsville (MD): National Center for Health Statistics, 1995
SAS Institute Inc. SAS system software. Version 6.12. Cary, NC: SAS Institute, 1995
US Census Bureau. Population estimates for the U.S., regions, divisions, and states by 5-year age groups and sex: annual time series estimates, July 1, 1990 to July 1, 1998. Internet release date: June 15, 1999: <http://www.census.gov/population/estimates/state/5age9890.txt>
Smith KJ, Roberts MS. The cost-effectiveness of sildenafil. Ann Intern Med 2000; 132: 933–7
Stolk EA, Busschbach JJ, Caffa M, et al. Cost utility analysis of sildenafil compared with papaverine-phentolamine injections. BMJ 2000; 320: 1165–8
Tan HL. Economic cost of male erectile dysfunction using a decision analytic model: for a hypothetical managed-care plan of 100,000 members. Pharmacoeconomics 2000; 17: 77–107
Plumb JM, Guest JF. Annual cost of erectile dysfunction to UK society. Pharmacoeconomics 1999; 16: 699–709
Keith A. The economics of Viagra. Health Aff (Millwood) 2000; 19: 147–57
Kwok YS, Kim C. Valuing Viagra: what is restoring potency worth? Eff Clin Pract 1999; 2: 171–5
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Skaer, T.L., Sclar, D.A., Robison, L.M. et al. Trends in the Rate of Self-Report and Diagnosis of Erectile Dysfunction in the United States 1990–1998. Dis-Manage-Health-Outcomes 9, 33–41 (2001). https://doi.org/10.2165/00115677-200109010-00004
Published:
Issue Date:
DOI: https://doi.org/10.2165/00115677-200109010-00004