
Abstract
Background: Asthma is a major public health problem in developed countries. In Canada, the prevalence of asthma is approximately 5 to 7%, with some provincial variation. A retrospective study using data collected in 1990 estimated the total costs of asthma in Canada to be between $Can504 million and $Can648 million (1990 dollars). 61% of all asthma costs were direct costs ($Can306 million). Of these, drugs were the single largest component ($Can124 million). Illness-related disability ($Can76 million) was the largest contributor to indirect costs.
Objective: To obtain individual patient-derived data on productivity loss and level of function related to severity of asthma symptoms, and briefly review the published data on the role of education and drug therapy in asthma management.
Design: This was a community-based prospective study of outpatients identified from the bronchial inhaler study of the Canadian Pharmacy Medication Monitoring Program.
Methods: Study patients recruited through community pharmacies were monitored for 6 months. Data were collected through structured telephone interviews at 1, 3 and 6 months.
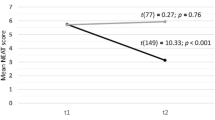
Primary Outcome Measures and Results: The primary outcome measures were symptom-free days (SFDs), productivity-loss days (PLDs) and patientreported function level. Patients who did not use inhaled corticosteroids had similar numbers of SFDs and PLDs compared with patients who did. Daily corticosteroid usage was a surrogate measure for severe disease because this group also reported fewer SFDs and more PLDs than patients who use corticosteroids as needed and patients who did not use inhaled corticosteroids.
Discussion: The evidence suggests that the greatest impact on productivity for the majority of patients comes from the number of days symptoms interfere with usual daily activities as opposed to actual days missed from work. Further, if corticosteroids are used appropriately in current nonusers who are not optimally controlled, a decrease in PLD and an increase in SFD may be seen. Results from another Canadian study have depicted the under-prescribing of inhaled corticosteroids, and the effectiveness of asthma education on improving the quality of life. A meta-analysis of relevant studies has confirmed that education improves important clinical outcomes in adults with asthma.
Conclusions: Better patient management in asthma is needed to reduce the economic burden of this disease.
Similar content being viewed by others

References
Ernst P, FitzGerald JM, Spier S. Canadian asthma consensus conference summary of recommendations. Can Respir J 1996; 3: 89–99
Erzen D, Carriere KC, Dik N, et al. Income level and asthma prevalence and care patterns. Am J Respir Crit Care Med 1997; 155: 1060–5
Trakas K, Shear NH, Oh PL. Characterization of the Canadian asthmatic population utilizing the National Population Health Survey (NPHS) [abstract]. Can J Clin Pharmacol 1997; 4: 54
Johansson H, Dutta M, Mao Y, et al. An investigation of the increase of preschool-age asthma in Manitoba, Canada. Health Rep 1992; 4: 379–402
Mao Y, Semenciw R, Morrison H, et al. Increased rates of illness and death from asthma in Canada. Can Med Assoc J 1987; 137: 620–4
Krahn MD, Berka C, Langlois P, et al. Direct and indirect costs of asthma in Canada, 1990. Can Med Assoc J 1996; 154: 821–31
Mellis CM, Peat JK, Woolcock AJ. The cost of asthma. Can it be reduced? Pharmacoeconomics 1993; 3: 205–19
Canadian Public Health Association. Economic burden of illness in Canada, 1993. Ottawa: Health Canada, 1997
Liljas B. How to calculate indirect costs in economic evaluations. Pharmacoeconomics 1998; 13: 1–7
Mellis CM, Peat JK, Bauman AE, et al. The cost of asthma in New South Wales. Med J New S Wales 1991; 155: 522–8
Weiss KB, Gergen PJ, Hodgson TA. An economic evaluation of asthma in the United States. N Engl JMed 1992; 326:862–6
Neutel CI. Drug utilization patterns as indicators. Pharmacoepidemol Drug Saf 1998; 7: 131–3
Willison DJ, Gaebel KA, Borden EK, et al. Experience in the development of a postmarketing surveillance network: the pharmacy medication monitoring program. Ann Pharmacother 1995; 29: 1208–13
Ungar WJ, Coyte PC, Chapman KR, et al, PMMP Advisory Board. The patient level cost of asthma in adults in south central Ontario. Can Respir J 1998; 5: 463–71
Ungar WJ, Coyte PC and the PMMP Advisory Board. Health services utilization reporting in respiratory patients. J Clin Epidemiol 1998; 51: 1335–42
Wang ECY, Gaebel KA. The burden of symptoms in patients with asthma [abstract 165]. Pharmacoepidemol Drug Saf 1998; 7(2 Suppl.):S148
Dales RE, Kerr PE, Schweitzer I, et al. Asthma management preceding an emergency department visit. Arch Intern Med 1992; 152: 2041–4
Speight AN, Lee DA, Hey EN. Underdiagnosis and undertreatment of asthma in childhood. BMJ (Clin Res Ed) 1983; 286: 1253–6
Bauman A, Young L, Peat JK, et al. Asthma under-recognition and under-treatment in an Australian community. Aust NZ J Med 1992; 22: 36–40
Wever AMJ, Wever-Hess J, Britton MG. Screening, diagnostic and outcome tools for asthma. Dis Manage Health Outcomes 1998; 3: 229–38
Cochrane GM. Impact of education on treatment compliance in patients with asthma. Monaldi Arch Chest Dis 1993 Aug; 48(4): 369–71
Cowan S, Cartier A, Boulet L-P, et al. The impact of an asthma education program on improving the quality of prescribing [abstract 253]. Pharmacoepidemiol Drug Saf 1998; 7(2 Suppl.): S186
Devine EC. Meta-analysis of the effects of psychoeducational care in adults with asthma. Res Nurs Health 1996 Oct; 19(5): 367–76
Volmer T. Economic considerations of patient education. Pneumologie 1997; 51: 850–7
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wang, E.C.Y., Gaebel, K.A. The Burden of Asthma Symptoms and the Positive Role of Patient Management. Dis-Manage-Health-Outcomes 6, 83–91 (1999). https://doi.org/10.2165/00115677-199906020-00004
Published:
Issue Date:
DOI: https://doi.org/10.2165/00115677-199906020-00004