
Summary
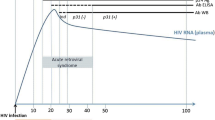
Patients are asymptomatic during the majority of HIV infection. The virus, however, is actively replicating, producing over 1 billion particles per day during this steady-state of the disease. Management of asymptomatic HIV infection involves initial recognition of infection and counselling to prevent its further spread.
When HIV infection has been confirmed, assessment consists of a careful history, physical examination and laboratory studies. The latter include serological tests for past exposure to infectious agents such as syphilis, hepatitis viruses, cytomegalovirus and toxoplasmosis. A purified protein derivative (PPD) skin test should also be performed. The immunological and virological status of the patient is assessed by quantifying CD4+ count and plasma HIV RNA levels. With the aid of these data, a decision can be made on the use of antiretroviral therapy.
Didanosine (ddI) is the only currently acceptable monotherapy. Combinations of antiretroviral drugs which have undergone evaluation include zidovudine (AZT) plus didanosine, zidovudine plus zalcitabine (ddC), zidovudine plus lamivudine (3TC), didanosine plus lamivudine, zidovudine plus didanosine plus nevirapine, zidovudine plus saquinavir, zidovudine plus zalcitabine plus saquinavir (D4T), zidovudine plus ritonavir, zidovudine plus lamivudine plus indinavir, and ritonavir plus saquinavir.
The optimum combination treatment has not been defined, but many appear promising. In addition, treatment for subclinical infections and prophylaxis should be administered. These include treatment of all PPD-positive patients with isoniazid 300 mg/day orally for 1 year; prophylaxis against Pneumocystis carinii pneumonia for all patients with CD4+ counts <200/mm3 with cotrimoxazole (trimethoprim plus sulfamethoxazole) one double-strength tablet daily, dapsone or dapsone plus trimethoprim; prophylaxis against toxoplasmosis in patients with CD4+ counts <100/mm3 with cotrimoxazole or with dapsone plus pyrimethamine; prophylaxis against disseminated Mycobacterium avium complex disease in patients with CD4+ counts <75/mm3 with azithromycin 1200mg orally once weekly, clarithromycin 500mg orally twice daily, or rifabutin 300 mg/day orally; and prophylaxis against Streptococcus pneumoniae pneumonia and bacteraemia by administration of the 23-valent pneumococcal vaccine.
Although cytomegalovirus disease occurs in most patients with advanced HIV disease (CD4+ <50/mm3), primary prophylaxis is not recommended because of conflicting data concerning the efficacy of oral ganciclovir. Primary prophylaxis against cryptococcosis is not recommended because of the low incidence of this infection.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Quinn TC. Global burden of the HIV pandemic. Lancet 1996; 348: 99–106
Wei X, Gosh SK, Taylor ME, et al. Viral dynamics in human immunodeficiency virus type 1 infection. Nature 1995; 373: 117–22
Ho DD, Neuman AU, Perelson AS, et al. Rapid turnover of plama virions and CD4 lymphocytes in HIV-1 infection. Nature 1995; 373: 123–6
Fahey JL, Taylor JMG, Detels R, et al. The prognostic value of cellular and serologic markers in infection with human immunodeficiency virus type 1. N Engl J Med 1990; 322: 166–72
Kaplan JE, Masur H, Holmes KK, et al. USPHS/IDSA guidelines for the prevention of opportunistic infections in persons infected with human immunodeficiency virus: an overview. Clin Infect Dis 1995; 21 Suppl. 1: S12–31
Saag MS, Holodoniy M, Kuritzkes DR, et al. HIV viral load markers in clinical practice. Nature Med 1996; 2: 625–9
Mellors JW, Kingsley LA, Rinaldo CR, et al. Quantitation of HIV-1 RNA in plasma predicts outcome after seroconversion. Ann Intern Med 1995; 122: 573–9
Mellors JW, Rinaldo CR, Gupta P, et al. Prognosis in HIV-1 infection predicted by the quantity of virus in plasma. Science 1996; 272: 1167–70
O’Brien TR, Blattner WA, Waters D, et al. Serum HIV-1 RNA levels and time to development of AIDS in the multicenter hemophilia cohort study. JAMA 1996; 276: 106–10
Welles SL, Jackson JB, Yen-Lieberman B, et al. Prognostic value of plasma human immunodeficiency virus type 1 (HIV-1) RNA levels in patients with advanced HIV-1 disease and with little or no prior zidovudine therapy. J Infect Dis 1996; 174: 696–703
O’Brien WA, Hartigan PM, Martin D, et al. Changes in plasma HIV-1 RNA and CD4+ lymphocyte count relative to treatment and progression to AIDS. N Engl J Med 1996; 334: 426–31
Katzenstein DA, Hammer SM, Hughes MD, et al. The relation of virologic and immunologic markers to clinical outcomes after nucleoside therapy in HIV-infected adults with 200 to 500 CD4 cells per cubic millimeter. N Engl J Med 1996; 336: 1091–8
Carpenter CJ, Fischl MA, Hammer SM, et al. Consensus statement: antiretroviral therapy for HIV infection in 1996. Recommendations of an international panel. JAMA 1996; 276: 146–54
Volberding PA, Lagakos SW, Grimes JM, et al. A comparison of immediate with deferred zidovudine therapy for asymptomatic HIV-infected adults with CD4 cell counts of 500 or more per cubic millimeter. N Engl J Med 1995; 333: 401–7
Hamilton JD, Hartigan PM, Simberkoff MS, et al. A controlled trial of early versus later zidovudine in symptomatic human immunodeficiency virus infection: results of a Veterans Affairs Cooperative Study. N Engl J Med 1992; 326; 437–43
Volberding PA, Lagakos SW, Koch MA, et al. Zidovudine in asymptomatic human immunodeficiency virus infection: a controlled trial in persons with fewer than 500 CD4-positive cells per cubic millimeter. N Engl J Med 1990; 322: 941–9
Volberding PA, Lagakos SW, Grimes JM, et al. The duration of zidovudine benefit in persons with asymptomatic HIV infection: prolonged evaluation of protocol 019 of the AIDS Clinical Trials Group. JAMA 1994; 272: 437–42
Concorde Coordinating Committee. Concorde MRC/ANRS randomized double-blind controlled trail of immediate and deferred zidovudine in symptom-free HIV infection. Lancet 1994; 343: 871–81
Dolin R, Amato DA, Fischl MA, et al. Zidovudine compared with didanosine in patients with advanced HIV type 1 infection and little or no previous experience with zidovudine. Arch Intern Med 1995; 155: 961–74
Kahn JO, Lagakos SW, Richman DD, et al. A controlled trial comparing continued zidovudine with didanosine in human immunodeficiency virus infection. N Engl J Med 1992; 327: 581–7
Montaner JSG, Schechter MT, Rachlis A, et al. Didanosine compared with continued zidovudine therapy for HIV-infected patients with 200 to 500 CD4 cells/mm3: a double-blind, randomized, controlled trial. Ann Intern Med 1995; 123: 561–71
Spruance SL, Pavia AT, Peterson D, et al. Didanosine compared with continuation of zidovudine in HIV-infected patients with signs of clinical deterioration while receiving zidovudine: a randomized, double-blind clinical trial. Ann Intern Med 1994; 120: 360–8
Fischl MA, Olson RM, Follansbee SE, et al. Zalcitabine compared with zidovudine in patients with advanced HIV-1 infection who received previous zidovudine therapy. Ann Intern Med 1993; 118: 762–9
Abrams DI, Goldman AI, Launer C, et al. A comparative trial of didanosine or zalcitabine after treatment with zidovuine in patients with human immunodeficiency virus infection. N Engl J Med 1994; 330: 657–62
Fischl MA, Stanley K, Arduino JM, et al. Combination and monotherapy with zidovudine and zalcitabine in patients with advanced HIV disease. Ann Intern Med 1995; 122: 24–32
Cao Y, Ho DD, Todd JJ, et al. Clinical evaluation of branched DNA signal amplification for quantifying HIV type 1 in human plasma. AIDS Res Hum Retroviruses 1995; 11: 353–61
Larder BA, Darby G, Richmann DD. HIV with reduced sensitivity to zidvudine (AZT) isolated during prolonged therapy. Science 1989; 243: 1731–4
Johnson VA. Nucleoside reverse transcriptase inhibitors and resistance of human immunodeficiency virus type 1. J Infect Dis 1995; 171 Suppl. 2: S140–9
Markowitz M, Mo H, Kempf DJ, et al. Selection and analysis of human immunodeficiency virus type 1 variants with increased resistance to ABT-538, a novel protease inhibitor. J Virol 1995; 69: 701–6
Hammer SM, Katzenstein DA, Hughes MD, et al. A trial comparing nucleoside montherapy with combination therapy in HIV infected adults with CD4 cell counts from 200 to 500 per cubic millimeter. N Engl J Med 1996; 335: 1081–90
Delta Coordinating Committee. Delta: a randomized double-blind controlled trial comparing combinations of zidovudine plus didansosine or zalcitabine with zidovudine alone in HIV-infected individuals. Lancet 1996; 348: 283–91
Saravolatz LD, Winslow DL, Collins G, et al. Zidovudine alone or in combination with didanosine or zalcitabine in HIV infected patients with the acquired immunodeficiency syndrome or fewer than 100 CD4 cells per cubic millimeter. N Engl J Med 1996; 335: 1099–106
Boucher CA, Cammack N, Schipper P, et al. High level resistance to () enantiomeric 2-deoxy-3-thiacytidine in vitro is due to one amino acid substitution in the catalytic site of human immunodeficiency virus type 1 reverse transcriptase. Anti-microb Agents Chemother 1993; 37: 2231–4
Schinazi RF, Lloyd RM, Nguyen MH, et al. Characterization of human immunodeficiency viruses resistant to oxanthiolane-cytosine nucleosides. Antimicrob Agents Chemother 1993; 37: 875–81
Eron JJ, Benoit SI, Jemsek J, et al. Treatment with lamivudine, zidovudine, or both in HIV-positive patients with 200 to 500 CD4+ cells per cubic millimeter. N Engl J Med 1995; 333: 1662–9
Eron JJ, Quinn JB, Hill-Price S, et al. 52 week follow-up of NUCA 3001: 3TC, zidovudine or both in the treatment of HIV-positive patients with CD4 cell counts of 200–500 cells/mm3. Presented at the 3rd Conference on Retroviruses and Opportunistic Infections; 1996 Jan 29–Feb 1; Washington, DC: The American Society for Microbiology, 1996
Bartlett JA, Benoit SL, Johnson VA, et al. Lamivudine plus zidovudine compared with zalcitabine plus zidovudine in patients with HIV infection: a randomized, double-blind, placebo-controlled trial. Ann Intern Med 1996; 125: 161–72
Havlir D, McLaughlin MM, Richman DD. A pilot study to evaluate the development of resistance to nevirapine in asymptomatic human immunodeficiency virus-infected patients with CD4 cell counts of >500/mm3: AIDS Clinical Trials Group Protocol 208. J Infect Dis 1995; 172: 1379–83
D’Aquila RT, Hughes MD, Johnson VA, et al. Nevirapine, zidovudine, and didanosine compared with zidovudine and didanosine in patients with HIV-1 infection: a randomized, double-blind, placebo-controlled trial. Ann Intern Med 1996; 124: 1019–30
Collier AC, Coombs RW, Schoenfeld DA, et al. Treatment of human immunodeficiency virus infection with saquinavir, zidovudine, and zalcitabine. N Engl J Med 1996; 334: 1011–7
Cameron B, Heath-Chiozzi M, Kravcik S, et al. Prolongation of life and prevention of AIDS in advanced HIV immunodeficiency with ritonavir. Presented at the 3rd Conference on Retroviruses and Opportunistic Infections; 1996 Jan 29–Feb 1; Washington, DC: The American Society for Microbiology, 1996
Gulick R, Mellors J, Havlir D, et al. Potent and sustained antiretroviral activity of indinavir in combination with zidovudine and lamivudine. Presented at the 3rd Conference on Retroviruses and Opportunistic Infections; 1996 Jan 29–Feb 1; Washington, DC: The American Society for Microbiology, 1996
Cohen C, Sun E, Cameron D, et al. Ritonavir-saquinavir combination treatment in HIV-infected patients [abstract no. LB7b]. Presented at the 36th Interscience Conference on Antimicrobial Agents and Chemotherapy; 1996 Sep 15–18; New Orleans. Washington, DC: The American Society for Microbiology, 1996
Selwyn PA, Hartel D, Lewis VA, et al. A prospective study of the risk of tuberculosis among intravenous drug users with human immunodeficiency virus infection. N Engl J Med 1989; 320: 545–50
Whalen C, Horsburgh CR, Hom D, et al. Accelerated course of human immunodeficiency virus infection after tuberculosis. Am J Respir Crit Care 1995; 151: 129–35
Castro KG. Tuberculosis as an opportunistic disease in persons infected with human immunodeficiency virus. Clin Infect Dis 1995; 21 Suppl. 1: S66–71
Phair J, Muñoz A, Detels R, et al. The risk of Pneumocystis carinii pneumonia among men infected with human immunodeficiency virus type 1. N Engl J Med 1990; 322: 161–5
Schneider MME, Hoepelman AIM, Schattenkerk JKME, et al. A controlled trial of aerosolized pentamidine or trimethoprim-sulfamethoxazole as primary prophylaxis against Pneumocystis carinii pneumonia in patients with human immunodeficiency virus infection. N Engl J Med 1992; 327: 1836–41
Hardy WD, Feinberg J, Finkelstein DM, et al. A controlled trial of aerosolized pentamidine or trimethoprim-sulfamethoxazole as secondary prophylaxis against Pneumocystis carinii pneumonia in patients with human immunodeficiency virus infection. N Engl J Med 1992; 327: 1842–8
Simonds RJ, Hughes WT, Feinberg J, et al. Preventing Pneumocystis carinii pneumonia in persons infected with human immunodeficiency virus. Clin Infect Dis 1995; 21 Suppl. 1: S44–8
Luft BJ, Remington JS. Toxoplasmic encephalitis in AIDS. Clin Infect Dis 1992; 15: 211–22
Richards FO, Kovacs JA, Luft BJ. Preventing toxplasmic encephalitis in persons infected with human immunodeficiency virus. Clin Infect Dis 1995; 21 Suppl. 1: S49–56
Nightingale SD, Byrd LT, Southern PM, et al. Incidence of Mycobacterium avium-intracellulare complex bacteremia in human immunodeficiency virus-positive patients. J Infect Dis 1992; 1082–5
Nightingale SD, Cameron DW, Gordin FM, et al. Two controlled trials of rifabutin prophylaxis against Mycobacterium avium complex infection in AIDS. N Engl J Med 1993; 329: 828–33
Pierce M, Crampton S, Henry D, et al. A randomized trial of clarithromycin as prophylaxis against disseminated Mycobacterium avium complex infection in patients with advance acquired immunodeficiency syndrome. N Engl J Med 1996; 335: 384–91
Havlir DV, Dube MP, Sattler FR, et al. Prophylaxis against disseminated Mycobacterium avium complex with weekly azithromycin, daily rifabutin, or both. N Engl J Med 1996; 335: 392–8
Ostroff SM, Spiegel RA, Feinberg J, et al. Preventing disseminated Mycobacterium avium complex disease in patients infected with human immunodeficiency virus. Clin Infect Dis 1995; 21 Suppl. 1: S72–6
Spector SA, McKinley GF, Lalezari JP, et al. Oral ganciclovir for the prevention of cytomegalovirus disease in persons with AIDS. N Engl J Med 1996; 34: 1491–7
Brosgart CL, Craig C, Hillman D, et al. A randomized, placebo-controlled trial of the safety and efficacy of oral ganciclovir for prophylaxis of CMV retinitis and gastrointestinal mucosal disease in HIV-infected individuals with severe immunosuppression [abstract no. LB-10]. Presented at the 35th Interscience Conference on Antimicrobial Agents and Chemotherapy; 1995 Sep 17–20; San Francisco. Washington, DC: The American Society for Microbiology, 1995
Rose DN, Sacks HS, Lan V. Cost-effectiveness analysis of oral ganciclovir to prevent cytomegalovirus disease in patients with AIDS. Presented at the 3rd Conference on Retroviruses and Opportunistic Infections; 1996 Jan 29–Feb 1; Washington, DC: The American Society for Microbiology, 1996
Powderly WG, Finkelstein DM, Feinberg J, et al. A randomized trial comparing fluconazole with clotrimazole troches for the prevention of fungals infection in patients with advanced human immunodeficiency syndrome. N Engl J Med 1995; 332: 700–5
Polsky B, Gold JWM, Whimbey E, et al. Bacterial pneumonia in patients with the acquired immunodeficiency syndrome. Ann Intern Med 1985; 104: 38–41
Redd SC, Rutherford GW, Sande MA, et al. The role of human immunodeficiency virus infection in pneumococcal bacteremia in San Francisco residents. J Infect Dis 1990; 162: 1012–7
Simberkoff MS, El-Sadr W, Schiffman G, et al. Streptococcus pneumoniae infection in patients with acquired immune deficiency syndrome, with report of a pneumococcal vaccine failure. Am Rev Resp Dis 1984; 130: 1174–6
Huang KL, Ruben FL, Rinaldo CR, et al. Antibody responses after influenza and pneumococcal immunization in HIV-infected homosexual men. JAMA 1987; 257: 2047–50
Centers for Disease Control. Update on adult immunization: recommendations of the Immunization Practices Advisory Committee (ACIP). Pneumococcal disease. MMWR Morb Mortal Wkly Rep 1991; 40(RR-12): 42–4
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Simberkoff, M.S. Management of Asymptomatic HIV Infection. Dis Manage Health Outcomes 1, 105–117 (1997). https://doi.org/10.2165/00115677-199701020-00005
Published:
Issue Date:
DOI: https://doi.org/10.2165/00115677-199701020-00005