
Abstract
Objective: Numerous studies support the benefit of β-blockers and angiotensin-converting enzyme inhibition (ACE-I) in the management of heart failure. However, the real-world cost of heart failure in patients who take these medications is not well documented; furthermore, it is unclear if heart failure costs remain significant when current, appropriately aggressive care is delivered.
Design: This study describes 1-year medical costs in patients hospitalised for heart failure who received these therapies, alone or in combination.
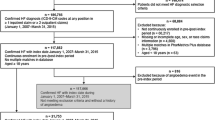
Methods: The study population was derived from 2.5 million patients with at least 3 years’ continuous eligibility in Pharmetrics®, an integrated claims and pharmacy database on approximately 25 million covered lives from 40 US health plans. The enrolment period was from 1 January 1996 to 31 December 2000. Costs included all recorded payments over a 1-year period. A total of 3073 patients (age >18 years) hospitalised with heart failure were identified (mean [± SD] age 72 ± 13 years; 46% female).
Results: The 1-year cost was $US16 786 in patients who received neither ACE inhibitors nor β-blockers as compared with $US19 567, $US22 785 and $US27 078 in patients who received ACE inhibitors, β-blockers or both drugs at maximum dosage, respectively (p < 0.001) [year of costing 2000]. Follow-up costs were substantial, representing almost twice the initial hospitalisation cost. Adjusted for age, sex, diabetes mellitus, coronary disease, hypertension and renal failure, costs remained significant in heart failure patients who received ACE inhibitors and/or β-blockers.
Conclusions: The 1-year cost of therapy for patients with heart failure is substantial, and there remains considerable need for more effective therapy to reduce the societal economic burden.








Similar content being viewed by others


References
American Heart Association. 2002 Heart and Stroke Statistical Update. Dallas (TX): American Heart Association, 2001
Rich MW, Nease RF. Cost-effectiveness analysis in clinical practice: the case of heart failure. Arch Intern Med 1999; 159: 1690–700
Weintraub WS, Cole J, Tooley J. Cost and cost-effectiveness studies in heart failure research. Am Heart J 2002; 143: 565–76
Garg R, Yusuf S, for the Collaborative Group on ACE Inhibitor Trials. Overview of randomized trials of angiotensin-converting-enzyme inhibitors on mortality and morbidity in patients with heart failure. JAMA 1995; 273: 1450–6
LeJemtel TH, Sonnenblick EH, Frishman WH. Diagnosis and management of heart failure. In: Fuster V, Alexander RA, O’Rourke RA, et al., editors. Hurst’s the heart. New York: McGraw-Hill, 2001: 692–700
Weintraub WS, Krumholz H. Cost-effective strategies in cardiology. In: Fuster V, Alexander RW, O’Rourke RA, et al., editors. Hurst’s the heart. New York: McGraw-Hill, 2001: 2487–512
Eisenberg SS. Benchmarking in understanding resource utilization and disease management: are we ready? Mining a large national database for supporting healthplan programs and activities using diabetes as a prototype. Dis Manag Health Outcomes 2001; 9 Suppl. 1: 29–38
Xuan J, Duong PT, Russo PA, et al. The economic burden of congestive heart failure in a managed care population. Am J Manag Care 2000; 6: 693–700
Weintraub WS, Kawabata H, Tran M, et al. Influence of co-morbidity on cost of care for heart failure. Am J Cardiol 2003; 91: 1011–5
SAS Institute Inc., Cary, NC, USA
http/www.cms.gov [Accessed 2002 Aug 19]
Rich MW, Beckham V, Wittenberg C, et al. A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure. N Engl J Med 1995; 333: 1190–5
West JA, Miller NH, Parker KM, et al. A comprehensive management system for heart failure improves clinical outcomes and reduces medical resource utilization. Am J Cardiol 1997; 79: 58–63
The Antiarrhythmics Versus Implantable Defibrillators (AVID) Investigators. A comparison of antiarrhythmic drug therapy with implatable defibrillators in patients resuscitated from near-fatal ventricular arrhythmicas. N Engl J Med 1997; 337: 1576–83
Moss AJ, Hall WJ, Cannom DS, et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. N Engl J Med 1996; 335: 1933–40
Auricchio A, Ding J, Spinelli JC, et al. Cardiac resynchronization therapy restores optimal atrioventricular mechanical timing in heart failure patients with ventricular conduction delay. J Am Coll Cardiol 2002; 39: 1163–9
Abraham WT, Fisher WG, Smith AL, et al. Cardiac resynchronization in chronic heart failure. N Engl J Med 2002; 346: 1845–53
Hannan EL, Kilburn Jr H, Lindsey ML, et al. Clinical versus administrative data bases for CABG Surgery: does it matter? Med Care 1992; 30: 892–907
Weintraub WS, Deaton C, Shaw L, et al. Can cardiovascular clinical characteristics be identified and outcome models be developed from an in-patient claims database? Am J Cardiol 1999; 84: 166–9
Acknowledgements
Dr Weintraub is a consultant to Bristol-Myers Squibb; Mr Kawabata, Ms Tran, Dr l’italien and Dr Chen are employees of Bristol-Myers Squibb.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Weintraub, W.S., Kawabata, H., Tran, M. et al. Cost of Heart Failure in Patients Receiving β-Blockers and Angiotensin-Converting Enzyme Inhibitors. Clin. Drug Investig. 24, 255–264 (2004). https://doi.org/10.2165/00044011-200424050-00002
Published:
Issue Date:
DOI: https://doi.org/10.2165/00044011-200424050-00002