
Abstract
Objective: To monitor the safety and efficacy profile of long-term treatment with diclofenac, nabumetone, meloxicam and celecoxib in patients with rheumatoid arthritis.
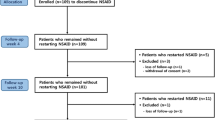
Design and methods: This randomised, prospective clinical trial included a total of 461 subjects (313 females and 148 males) with clinically diagnosed rheumatoid arthritis. Their average age was 46.9 ± 14.4 years (range 20–69 years), and the average disease duration was 1333.7 ± 992.85 days. Subjects were randomly assigned daily administration of one of the following: diclofenac 75–100mg, meloxicam 15mg, nabumetone l000mg or celecoxib 200mg. During the 6-month treatment period, a monthly patient interview was conducted to evaluate drug efficacy and safety.
Results: 407 subjects successfully completed the 6-month treatment. Sixteen patients (12.2%) withdrew from the diclofenac group, 16 (12.2%) from the nabumetone group, 17 (11.8%) from the meloxicam group and five (9.1%) from the celecoxib group. Most withdrawals occurred during the first 3 months of treatment. Reasons for withdrawals in the first three groups were lack of efficacy (44.9%) and adverse effects (38.8%). For the celecoxib group, high cost (80%) was the main reason for withdrawal. Adverse drug reactions to NSAIDs mostly occurred at an early stage of treatment, with an incidence rate of 31.9% for the diclofenac group, 19.9% for the nabumetone group, 25.2% for the meloxicam group, and 7.27% for the celecoxib group. Clinical efficacy rates for the four NSAIDs were positively related to the length of treatment. During the first 4 months, diclofenac, meloxicam and celecoxib showed better efficacy than nabumetone. There were no significant differences in efficacy during the fifth and sixth months. The overall 6-month effectiveness rates were 68.8% for diclofenac, 59.8% for nabumetone, 67.6% for meloxicam and 69.1% for celecoxib.
Conclusions: Adverse drug reactions and their related withdrawals occurred mostly at an early stage of NSAID treatment, so it is crucial to strengthen pharmacovigilance during this period. Among the investigated NSAIDs, celecoxib did not prove to be superior to diclofenac, nabumetone or meloxicam with respect to its efficacy in the treatment of rheumatoid arthritis; however, it did show good patient compliance and safety profiles.








Similar content being viewed by others


Notes
Shanghai’s general hospitals are ranked as A, B and C class according to their patient-bed volume and service quality. A is the highest hospital category, each usually equipped with more than 1000 patient beds.
References
Hawkey CJ. COX-1 and COX-2 inhibitors. Best Pract Res Clin Gastroenterol 2001; 15(5): 801–20
Marie R, Griffin MD. Epidemiology of non-steroidal anti-inflammatory drug-associated gastrointestinal injury. Am J Med 1998; 104(3A): 23–8
Arnet FC, Edworthy SM, Bloch DA. The American Rheumatoid Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 1998; 31: 315–7
Felson DT, Andersson JJ, Bores M, et al. American College of Rheumatology preliminary definition of improvement in rheumatoid arthritis. Arthritis Rheum 1995; 38: 727–35
Rovensky J, Micekova D. Six-month prospective study to monitor the treatment of rheumatic disease with sustained-release flubiprofen. Drugs Exp Clin Res 2000; 26(1): 19–24
Huskinsson EC, Ghozlan R, Kurthen R. A long-term study to evaluate the safety and efficacy of meloxicam therapy in the patients with rheumatoid arthritis. Br J Rheumatol 1996; 35Suppl. 1: 29–34
Jones CW. A post-marketing surveillance study of Voltarol 75mg SR in the primary case setting. Br J Clin Pract 1995; 50: 390–5
Tindall EA, Sharp JT, Burr A, et al. A 12-month, multicenter, prospective, open-label trial of radiographic analysis of disease progression in osteoarthritis of the knee or hip in patients receiving celecoxib. Clin Ther 2002; 24(12): 2051–63
Emery P, Zeidler H, Kvien TK, et al. Celecoxib versus diclofenac in long-term management of rheumatoid arthritis: randomised double-blind comparison. Lancet 1999; 354(9196): 2106–11
Shi W, Wang YM, Cheng NN, et al. Meta-analysis on the effect and adverse reaction of NS AIDs treating patients with osteoarthritis and rheumatoid arthritis. Chinese J Epidemiol 2003; 24(11): 1044–8
Shi W, Wang YM, Cheng NN, et al. Sample size determination in a cohort study on NSAID adverse reactions. Chinese J Clin Pharmacol 2002; 18(6): 455–7
Lister BJ, Poland M, DeLapp RE. Efficacy of nabumetone versus diclofenac, naproxen, ibuprofen, and piroxicam in osteoarthritis and rheumatoid arthritis. Am J Med 1993; 95(2A): 2S–9S
Wordsworth BP. Rheumatoid arthritis. In: Weatherall DJ, Ledingham JGG, Warrell DA, editors. Oxford textbook of medicine: rheumatoid arthritis. New York: Oxford University Press, 1996: 2964
Weinblatt ME. Treatment of rheumatoid arthritis. In: Willian JK, editor. Arthritis and allied conditions, a textbook of rheumatology: rheumatoid arthritis. Baltimore (MD): Williams & Wilkins, 1997: 1134
Ahmad SR, Kortepeter C, Brinker A, et al. Renal failure associated with the use of celecoxib and rofecoxib. Drug Saf 2002; 25(7): 537–44
Gurkirpal S. Recent considerations in nonsteroidal anti-inflammatory drug gastropathy. Am J Med 1998; 105: 31–38s
Huskinsson EC, Ghozlan R, Kurthen R. A long-term study to evaluate the safety and efficacy of meloxicam therapy in the patients with rheumatoid arthritis. Br J Rheumatol 1996; 35Suppl. 1: 29–34
Deeks JJ, Smith LA, Bradley MD. Efficacy, tolerability, and upper gastrointestinal safety of celecoxib for treatment of osteoarthritis and rheumatoid arthritis: systematic review of randomized controlled trials. BMJ 2002; 325(7365): 619–24
Lanas A. Clinical experience with cyclooxygenase-2 inhibitors. Rheumatology (Oxford) 2002; 41Suppl. 1: 16–22
Acknowledgements
We thank the participating rheumatologists for their invaluable cooperation. This survey was supported in part by a grant (BK-PJ-0301) from the State Food and Drug Administration of China. The authors have no conflicts of interest directly relevant to the content of this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shi, W., Wang, Y.M., Li, L.S. et al. Safety and Efficacy of Oral Nonsteroidal Anti-Inflammatory Drugs in Patients with Rheumatoid Arthritis. Clin. Drug Investig. 24, 89–101 (2004). https://doi.org/10.2165/00044011-200424020-00004
Published:
Issue Date:
DOI: https://doi.org/10.2165/00044011-200424020-00004