
Abstract
Background: Early switch to oral antibacterials is recommended for the treatment of hospitalized patients with community-acquired pneumonia (CAP). However, its efficacy and safety in patients with more severe forms of CAP have not been well established.
Objective: To evaluate early switch to oral treatment in hospitalized patients with moderate to severe CAP.
Methods: Two reviewers independently extracted data from relevant randomized controlled trials (RCTs) with the same total duration of antibacterial treatment in the compared groups (early switch from intravenous to oral and conventional intravenous treatment for the whole duration of therapy).
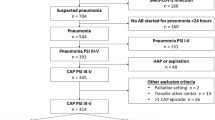
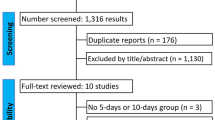
Results: Six RCTs including 1219 patients fulfilled the criteria for inclusion in the meta-analysis. Treatment success was not different between early switch to oral treatment and intravenous only treatment groups in both intention to treat (odds ratio [OR] 0.76; 95% CI 0.36, 1.59) and clinically evaluable patients (OR 0.92; 95% CI 0.61, 1.39). Mortality and recurrence of CAP were not different (OR 0.81; 95% CI 0.49, 1.33 and OR 1.81; 95% CI 0.70, 4.72, respectively), while duration of hospitalization was shorter (weight mean difference −3.34; 95% CI −4.42, −2.25) and drug-related adverse events were fewer in the early switch group (OR 0.65; 95% CI 0.48, 0.89). Findings were similar in patients with severe CAP.
Conclusions: Early conversion to oral antibacterials seems to be as effective as continuous intravenous treatment in patients with moderate to severe CAP and results in substantial reduction in duration of hospitalization.








Similar content being viewed by others

References
Marston BJ, Plouffe JF, File Jr TM, et al. Incidence of community-acquired pneumonia requiring hospitalization: results of a population-based active surveillance study in Ohio. The Community-Based Pneumonia Incidence Study Group. Arch Intern Med 1997; 157: 1709–18
Guest JF, Morris A. Community-acquired pneumonia: the annual cost to the National Health Service in the United Kingdom. Eur Respir J 1997; 10: 1530–4
Niederman MS, McCombs JS, Unger AN, et al. The cost of treating community-acquired pneumonia. Clin Ther 1998; 20: 820–37
Rello J, Catalan M, Diaz E, et al. Associations between empirical antimicrobial therapy at the hospital and mortality in patients with severe community-acquired pneumonia. Intensive Care Med 2002; 28: 1030–5
Feikin DR, Schuchat A, Kokzak M, et al. Mortality from invasive pneumococcal pneumonia in the era of antibiotic resistance, 1995–1997. Am J Public Health 2000; 90: 223–9
Mandell LA, Wunderink RG, Anzueto A, et al., for the Infectious Diseases Society of America-American Thoracic Society. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007; 44: S27–72
Woodhead M, Blasi F, Ewig S, et al. ERS task force in collaboration with ESCMID. Guidelines for the management of adult lower respiratory tract infections. Eur Respir J 2005; 26: 1138–80
Castro-Guardiola A, Viejo-Rodriguez AL, Soler-Simon S, et al. Efficacy and safety of oral and early-switch therapy for community-acquired pneumonia: a randomized controlled trial. Am J Med 2001; 111: 367–74
Siegel RE, Halpem NA, Almenoff PL, et al. A prospective randomized study of inpatient IV antibiotics for community-acquired pneumonia: the optimal duration of therapy. Chest 1996; 110: 965–71
Rhew DC, Tu GS, Ofman J, et al. Early switch and early discharge strategies in patients with community-acquired pneumonia: a meta-analysis. Arch Intern Med 2001; 161: 722–7
Halm EA, Switzer GE, Mittman BS, et al. What factors influence physicians' decision to switch from intravenous to oral antibiotics for community-acquired pneumonia? J Gen Intern Med 2001; 16: 599–605
Moher D, Pham B, Jones A, et al. Does quality of reports of randomized trials affects estimates of intervention efficacy reported in meta-analyses? Lancet 1998; 352: 609–13
Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med 1997; 336: 243–50
Lim WS, van der Eerden MM, Laing R, et al. Defining community-acquired pneumonia on presentation to hospital: an international derivation and validation study. Thorax 2003; 58: 377–82
Yaqub A, Khan Z. Comparison of early intravenous to oral switch amoxicillin/clavulanate with parenteral ceftriaxone in treatment of hospitalized patients with community acquired pneumonia. Pak J Med Sci 2005; 21: 259–66
Oosterheert JJ, Bonten MJM, Schneider MM, et al. Effectiveness of early switch from intravenous to oral antibiotics in severe community-acquired pneumonia: multicentre randomized trial. BMJ 2006; 333: 1193–8
Omidvari K, de Boisblanc BP, Karam G, et al. Early transition to oral antibiotic therapy for community-acquired pneumonia: duration of therapy, clinical outcomes, and cost analysis. Respir Med 1998; 92: 1032–9
Norrby SR, Petermann W, Willcox PA, et al. A comparative study of levofloxacin and ceftriaxone in the treatment of hospitalized patients with pneumonia. Scand J Infect Dis 1998; 30: 397–404
Lee RWW, Lindstrom ST. Early switch to oral antibiotics and early discharge guidelines in the management of patients with community-acquired pneumonia. Respirology 2007; 12: 111–6
Capelategui A, Espana PP, Quintana JM, et al. Improvement of process of care and outcomes after implementing a guideline for the management of community-acquired pneumonia: a controlled before and after design study. CID 2004; 39: 995–63
Marrie TJ, Lau CY, Wheeler SL, et al. A controlled trial of a critical pathway for treatment of community-acquired pneumonia. JAMA 2000; 283: 749–55
Halm EA, Fine MJ, Kapoor WN, et al. Instability on hospital discharge and the risk of adverse outcomes in patients with pneumonia. Arch Intern Med 2002; 162: 1278–84
Kothe H, Bauer T, Marre R, et al. Outcome of CAP: influence of age, residence status, and antimicrobial treatment. Eur Respir J 2008; 32: 139–46
Polic-Vizintin M, Lepee M, Stimac D, et al. Risk of pneumonia reccurence in patients previously hospitalized for pneumonia: a retrospective study. Coll Antropol 2005; 29: 213–9
Hedlund J, Ortqvist AB, Kalin M, et al. Risk of pneumonia in patients previously treated in hospital for pneumonia. Lancet 1992; 340: 396–7
Lanbeck P, Odenholt I, Riesbeck K. Dicloxacillin and erythromycin at high concentrations increase ICAM-1 expression by endothelial cells: a possible factor in the pathogenesis of infusion phlebitis. J Antimicrob Chemother 2004; 53: 174–9
Mortensen EM, Coley CM, Singer DE, et al. Causes of death for patients with community-acquired pneumonia: results from the pneumonia patient outcome research team cohort study. Arch Intern Med 2002; 162: 1059–64
Acknowledgements
No sources of funding were used to assist in the preparation of this meta-analysis. The authors have no conflicts of interest that are directly relevant to the content of this meta-analysis.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Athanassa, Z., Makris, G., Dimopoulos, G. et al. Early Switch to Oral Treatment in Patients with Moderate to Severe Community-Acquired Pneumonia. Drugs 68, 2469–2481 (2008). https://doi.org/10.2165/0003495-200868170-00005
Published:
Issue Date:
DOI: https://doi.org/10.2165/0003495-200868170-00005