
Abstract
The category of common sleep disorders known as parasomnias includes disorders of arousal, rapid eye movement (REM) sleep behaviour disorder (RBD), nocturnal seizures, rhythmic movement disorder, and tooth grinding or ‘bruxism’. Parasomnias are all characterised as undesirable physical or behavioural phenomena occurring during the sleep period. Although these conditions can be distressing and, in some cases, hazardous to the sleeper and his or her bed partner, it is important to recognise that parasomnias are diagnosable and treatable in the vast majority of patients.
Evaluation begins with a careful clinical interview with the sleeper and a family member to elucidate the frequency, duration, description and timing after sleep onset of these behavioural events.
Disorders of arousal are the most common type of parasomnia and cover a spectrum from calm sleepwalking to emotionally agitated or complex behaviours, such as dressing or driving, for which the patient usually has no memory upon awaking. ‘Sleep terrors’ are quite common in young children and are often outgrown. Disorders of arousal represent a partial, as opposed to a full, awakening from deep non-REM sleep, typically occurring within the first 60 to 90 minutes after sleep onset.
RBD is characterised clinically by a history of dream-enacting behaviour, and the patient may recall dream content. REM sleep periods typically occur in the latter half of the night. Physiologically, RBD results from a lack of the normal muscle atonia that is associated with REM sleep. RBD has been linked to a number of other neurological conditions; thus, a careful review of systems and a physical examination are crucial.
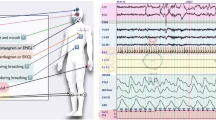
A formal laboratory sleep study or polysomnogram with an expanded electroencephalographic montage can help distinguish among non-REM and REM parasomnias and nocturnal seizures. The latter may manifest clinically as arousals from sleep associated with vocalisation and/or complex behaviours.
Rhythmic movement disorder can include head banging or body rocking at sleep onset or during the night. Tooth grinding is a common sleep-related behaviour that, when severe, can result in dental injury. Hypnagogic hallucinations (experience of dream imagery at sleep onset) and sleep-onset paralysis (experience of muscle/body paralysis as one is falling asleep) are symptoms rather than diagnostic categories. These phenomena classically occur in many individuals with narcolepsy, but also may occur in healthy sleep-deprived individuals.
Safety precautions and good general sleep hygiene measures are recommended for individuals with a parasomnia, as the disorder can be exacerbated by sleep deprivation and various other factors. When the events are frequent or particularly dramatic, medication with a long- or medium-acting benzodiazepine, such as clonazepam, at bedtime is effective therapy in most cases of non-REM disorders of arousal and RBD. A dental guard may be helpful in tooth grinders. Relaxation training and guided imagery may be helpful strategies for some patients, especially those with disorders of arousal or rhythm movement disorders. There is no evidence of any association between parasomnias and psychiatric illness. Demystification of these conditions and reassurance, particularly for parents of paediatric patients, is an important aspect of clinical intervention.




Similar content being viewed by others


References
Thorpy M, editor. Disorders of arousal. In: Handbook of sleepdisorders. New York: Marcel Dekker, 1990: 531–49
Mahowald M, Schenck C. Diagnosis and management of parasomnias. Postgrad Med 2000; 107(3): 145–56
Kryger M, Roth T, Dement W. Principles and practice of sleep medicine. 3rd ed. Philadelphia (PA): W.B. Saunders Company, 2000
Ohayon M, Guilleminault C, Priest R. Night terrors, sleepwalking,and confusional arousals in the general population: their frequency and relationship to other sleep and mental disorders. J Clin Psychiatry 1999; 60(4): 268–76
Mahowald M, Schenck C. Medical-legal aspects of sleep medicine. Neurol Clin 1999; 17: 215–34
Broughton RJ. Non-REM arousal parasomnias. In: Mahowald MW, editor. Principles and practice of sleep medicine. Philadelphia (PA): W.B. Saunders, 2000: 693–706
Eliseo T. The hypnotic treatment of sleepwalking in an adult. Am J Clin Hypn 1975; 17(4): 272–6
Reid W, Ahmed I, Levie C. Treatment of sleepwalking: a controlled study. Am J Psychother 1981; 35(1): 27–37
Schenck C, Mahowald M. Polysomnographic, neurologic, psychiatric and clinical outcome report on 70 consecutive cases with REM sleep behavior disorder (RBD): sustained clonazepam efficacy in 89.5% of 57 treated patients. Cleve Clin J Med 1990; 57: S9–23
Wright BA, Rosen JR, Buysse DJ, et al. Shy-Drager syndrome presenting as a REM behavioral disorder. J Geriatric Psychiatry Neurol 1990; 3: 110–3
Schenck CH, Mahowald MW. 5 cases of parkinsonism emerging after the onset of REM sleep behavior disorder (RBD) in men aged 58–79 years. Sleep Res 1993; 22: 261
Schenck CH, Mahowald MW. Motor dyscontrol in narcolepsy: rapid-eye-movement (REM) sleep without atonia and REM sleep behavior disorder. Ann Neurol 1992; 32: 3–10
Kimura K, Tachibana N, Kohyama J, et al. A discrete pontine ischemic lesion could cause REM sleep behavior disorder. Neurology 2000; 55(6): 894–5
Ferini-Strambi L, Zucconi M. REM sleep behavior disorder. Clin Neurophysiol 2000; 111 Suppl. 2: 136–40
Schutte S, Doghramji K. REM behavior disorder seen with venlafaxine (Effexor). Sleep Res 1996; 25: 365
Olson E, Boeve B, Silber M. Rapid eye movement sleep behaviour disorder: demographic, clinical and laboratory findings in 93 cases. Brain 2000; 123(2): 231–339
Schenck C, Hurwitz T, Mahowald M. REM sleep behavior disorder: an update on a series of 96 patients and a review of the world literature. J Sleep Res 1993; 2: 224–31
Bamford C. Carbamazepine in REM sleep behavior disorder. Sleep 1993; 16: 33–4
Schenck CH, Mahowald MW. REM sleep behavior disorder: clinical, developmental, and neuroscience perspectives 16 years after its formal identification in SLEEP. Sleep 2002; 25(2): 120–38
TinuperP, Piazzi G, Provini A, et al. The syndrome of nocturnal frontal lobe epilepsy. In: Lugaresi E, Parmeggiani PL, editors. Somatic and autonomic regulation in sleep. New York: Springer-Verlag, 1997: 125–35
Scheffer I, Bhatia KP, Lopes-Cendes I, et al. Autosomal dominant frontal epilepsy misdiagnosed as sleep disorder. Lancet 1994; 343: 515–7
Sheffer I, Bhatia KP, Lopes-Cendes I, et al. Autosomal dominant nocturnal frontal lobe epilepsy: a distinctive clinical disorder. Brain 1995; 118: 61–73
Oldani Z, Zicconi M, Renini-Strambi L, et al. Autosomal dominant nocturnal frontal lobe epilepsy. Epilepsia 1996;37:964–76
Ohayon M, Li KKD, Guilleminault CM. Risk factors for sleep bruxism in the general population. Chest 2001; 119(2): 53–61
Abe K, Shimakawa M. Genetic and developmental aspects of sleeptalking and teeth-grinding. Acta Paedopsychiatr 1966; 33: 339–44
Hartmann E. Bruxism. In: Kryeger M, Roth T, Dement W, editors. Principles and practice of sleep medicine. Philadelphia (PA): W.B. Saunders, 1989: 385–8
Wright E. Using soft splints in your dental practice. Gen Dent 1999; 47(5): 506–10
Garcia J, Rosen G, Mahowald M. Waterbeds in treatment of rhythmic movement disorders: experience with two cases. Sleep Res 1996; 25: 243
Ferber R, Kryger M. Principles and practices of sleep medicine. Philadelphia (PA): WB Saunders Co., 1995
Acknowledgements
The authors wish to express appreciation for the assistance of Drs Mark Mahowald and Carlos Schenck in the preparation of this manuscript. No sources of funding were used in its preparation. The authors have no conflicts of interest that are directly relevant to the content of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wills, L., Garcia, J. Parasomnias. CNS Drugs 16, 803–810 (2002). https://doi.org/10.2165/00023210-200216120-00002
Published:
Issue Date:
DOI: https://doi.org/10.2165/00023210-200216120-00002