
Abstract
Any drug administered in the peri-operative period has the potential to produce life-threatening immune-mediated anaphylaxis. The incidence of anaphylaxis has been estimated at between 1 in 10 000 and 1 in 20 000 anaesthesias in Australia and 1 in 13 000 anaesthesias in France. In the most recent French epidemiological survey, the compounds most frequently involved in anaphylaxis were muscle relaxants (60%), followed by latex (16%).
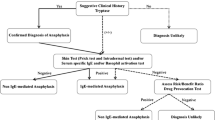
Activation of humoral and cellular pathways resulting from immunoglobulin E-mediated adverse reactions usually produces characteristic respiratory, cardiovascular and skin responses, but effects can be seen in virtually any system. These responses may occur as isolated clinical events. As a result, an anaphylacticreaction restricted to a single clinical symptom (e.g. bronchospasm, tachycardia) can easily be misdiagnosed. Intra- and postoperative investigations must be performed to confirm the nature of the adverse reaction, the role of the suspected drugs, and to define precise recommendations for future anaesthesias. The patient must be fully informed, and given a detailed written account of the anaphylactic episode, the results of the allergological assessment performed and the resulting recommendations. Furthermore, the patient should be strongly advise to wear a warning bracelet or carry a warning card.
Since no specific treatment has been proven to reliably prevent the onset of anaphylactic reactions, allergological assessment must be performed in all highrisk patients. The only possible strategy is to avoid the drug tested positively during the allergy work-up. Nevertheless, in cases where muscle relaxants are incriminated, patients allergic to one muscle relaxant can be administered another agent, the choice of which is based on skin test results. However, it should be borne in mind that rare cases of adverse reactions in spite of such screening procedures have been reported. On the contrary, there is no indication for allergological assessment in atopic patients who do not have additional anaesthetic agent risk factors or those allergic only to non-anaesthetic substances.
The treatment of anaphylaxis is aimed at interrupting contact with the responsible antigen, modulating the effects of released mediators, and inhibiting mediator production and release. Treatment must be initiated as quickly as possible, and relies on generally accepted principles.






Similar content being viewed by others

References
Portier P, Richet C. De l’action anaphylactique de certains venins. CR Soc Biol 1902; 6: 170–2
Paton WDM. Histamine release by compounds of simple chemical structure. Pharmacol Rev 1957; 9: 269–328
Watkins J, Ward AM, Thornton JA. Adverse reactions to intravenous induction agents [letter]. BMJ 1978; 2(6149): 1431
Lorenz W, Doenicke A, Feifel G, et al. Histamine release in man by propanidid (Epontol), gelatin (Haemaccel), histalog, pentagastrin and insulin. Naunyn Schmiedebergs Arch Pharmacol 1970; 266(4): 396–7
Lorenz W, Doenicke A, Schoning B, et al. Definition and classification of the histamine-release response to drugs in anaesthesia and surgery: studies in the conscious human subject. Klin Wochenschr 1982; 60(17): 896–913
Jerums G, Whittingham S, Wilson P. Anaphylaxis to suxamethonium: a case report. Br J Anaesth 1967; 39(1): 73–7
Fisher MM. Intradermal testing after severe histamine reactions to intravenous drugs used in anaesthesia. Anaesth Intensive Care 1976; 4(2): 97–104
Sigiel M, Laxenaire MC, Moneret-Vautrin DA, et al. Trois cas de choc anaphylactique à la Célocurine. Anesth Analg (Paris) 1975; 32: 447–62
Vervloet D, Arnaud A, Vellieux P, et al. Anaphylactic type of accidents due to myorelaxing agents during general anesthesia: clinical and biological study [in French]. Nouv Presse Med 1977; 6(9): 725–8
Galletly DC, Treuren BC. Anaphylactoid reactions during anaesthesia: seven years’ experience of intradermal testing. Anaesthesia 1985; 40(4): 329–33
Leynadier F, Sansarricq M, Didier JM, et al. Prick tests in the diagnosis of anaphylaxis to general anaesthetics. Br J Anaesth 1987; 59(6): 683–9
Fisher M. Intradermal testing after anaphylactoid reaction to anaesthetic drugs: practical aspects of performance and interpretation. Anaesth Intensive Care 1984; 12(2): 115–20
Baldo BA, Fisher MM. Substituted ammonium ions as allergenic determinants in drug allergy. Nature 1983; 306(5940): 262–4
Assem ESK. Anaphylactoid reactions to neuromuscular blockers: major role of IgE antibodies and possible contribution of IgE-independent mechanisms. In: Assem ESK, editor. Allergic reactions to anaesthetics: clinical and basic aspects. Basel: Karger, 1992: 24–53
Baldo BA, Fisher MM, Harle DG. Allergy to thiopentone. Clin Rev Allergy 1991; 9(3–4): 295–308
Laxenaire MC, Mata-Bermejo E, Moneret-Vautrin DA, et al. Life-threatening anaphylactoid reactions to propofol (diprivan) [see comments]. Anesthesiology 1992; 77(2): 275–80
Laxenaire MC. Encore et toujours l’allergie. Ann Fr Anesth Reanim 1999; 18: 831–3
Fisher MM, Baldo BA. The incidence and clinical features of anaphylactic reactions during anesthesia in Australia. Ann Fr Anesth Reanim 1993; 12(2): 97–104
Laxenaire MC. Epidémiologie des réactions anaphylactoïdes peranesthésiques. Quatrième enquête multicentrique (juillet 1994-décembre 1996). Ann Fr Anesth Reanim 1999; 18: 796–809
Sage D, Guarino R, Sage DD. Intradermal drug testing following anaphylactoid reactions during anaesthesia. Anaesth Intensive Care 1981; 9(4): 381–6
Pepys J, Pepys EO, Baldo BA, et al. Anaphylactic/anaphylactoid reactions to anaesthetic and associated agents: skin prick tests in aetiological diagnosis. Anaesthesia 1994; 49(6): 470–5
Moscicki RA, Sockin SM, Corsello BF, et al. Anaphylaxis during induction of general anesthesia: subsequent evaluation and management [see comments]. J Allergy Clin Immunol 1990; 86 (3 Pt 1): 325–32
Knowles SR, Weber E, Shear NH. Allergic reactions during general anesthesia (GA) [abstract]. J Allergy Clin Immunol 1996; 97: 344
Keith PK, Dolovich J. Anaphylactic and anaphylactoid reactions in the perioperative period. Immunol Allergy Clin North Am 1992; 12(3): 671–90
Watkins J. Adverse reaction to neuromuscular blockers: frequency, investigation, and epidemiology. Acta Anaesthesiol Scand Suppl 1994; 102: 6–10
Laxenaire MC, Moneret-Vautrin DA. Allergy and anaesthesia. Curr Opin Anaesthesiol 1992; 5: 436–41
Moneret-Vautrin DA, Laxenaire MC. The risk of allergy related to general anaesthesia. Clin Exp Allergy 1993; 23(8): 629–33
Gold M, Swartz JS, Braude BM, et al. Intraoperative anaphylaxis: an association with latex sensitivity. J Allergy Clin Immunol 1991; 87(3): 662–6
Warpinski JR, Folgert J, Cohen M, et al. Allergic reaction to latex: a risk factor for unsuspected anaphylaxis. Allergy Proc 1991; 12(2): 95–102
Moneret-Vautrin DA, Laxenaire MC, Gueant JL. Anaphylactic reactions to muscle relaxants. In: Pichler WJ, Stadler BM, Dahinden C, et al., editors. Progress in allergy and clinical immunology. Proceedings of the 13th International Congress of Allergology and Clinical Immunology: 1988 Oct 16–22; Montreux. Bern: Hogrefe & Huber, 1989: 450–4
Baird MB, Futter M. Anaphylaxis to mivacurium. Anaesth Intensive Care 1996; 24(4): 486–8
Yee R, Fernandez JA. Anaphylactic reaction to rocuronium bromide. Anaesth Intensive Care 1996; 24(5): 601–4
Barthelet Y, Ryckwaert Y, Plasse C, et al. Severe anaphylactic reactions to rocuronium bromide. Ann Fr Anesth Reanim 1999; 18: 896–900
Toh KW, Deacock SJ, Fawcett WJ. Severe anaphylactic reaction to cisatracurium. Anesth Analg 1999; 88(2): 462–4
Laxenaire MC. Drugs and other agents involved in anaphylactic shock occurring during anaesthesia: a French multicenter epidemiological inquiry. Ann Fr Anesth Reanim 1993; 12(2): 91–6
Laxenaire MC. Substances responsible for peranesthetic anaphylactic shock: a third French multicenter study (1992–94) [in French]. Ann Fr Anesth Reanim 1996; 15(8): 1211–8
Fisher MM, Baldo BA. Mast cell tryptase in anaesthetic anaphylactoid reactions. Br J Anaesth 1998; 80(1): 26–9
Fisher M, Baldo BA. Anaphylaxis during anaesthesia: current aspects of diagnosis and prevention. Eur J Anaesthesiol 1994; 11(4): 263–84
Porri F, Lemiere C, Birnbaum J, et al. Prevalence of muscle relaxant sensitivity in a general population: implications for a preoperative screening. Clin Exp Allergy 1999; 29(1): 72–5
Moneret-Vautrin DA, Renaudin JM, Kanny G, et al. Prospective study of the latent sensitization to muscle relaxants. In: Dehling AK, Huerat-Lopez JG, editors. Progress in allergy and clinical immunology. Cancun: Hogrefe and Huber, 1997: 361–76
Albrech C, Widmer S, Beaudoin E, et al. Prospective study of sensitization to muscle relaxants [abstract]. J Allergy Clin Immunol 1995; 95: 289
Laroche D, Lefrancois C, Gerard JL, et al. Early diagnosis of anaphylactic reactions to neuromuscular blocking drugs. Br J Anaesth 1992; 69(6): 611–4
Laroche D, Dubois F, Lefrancois C, et al. Early biological markers of anaphylactoid reactions occurring during anesthesia [in French]. Ann Fr Anesth Reanim 1992; 11(6): 613–8
Laroche D, Vergnaud MC, Sillard B, et al. Biochemical markers of anaphylactoid reactions to drugs: comparison of plasma histamine and tryptase. Anesthesiology 1991; 75(6): 945–9
Aimone-Gastin I, Gueant JL, Laxenaire MC, et al. Pathogenesis of allergic reactions to anaesthetic drugs. Int J Immunopathol Pharmacol 1997; 10(2): 193–6
de Weck AL. Immunochemical particularities of anaphylactic reactions to compounds used in anesthesia. Ann Fr Anesth Reanim 1993; 12(2): 126–30
Falk K, Rotzschke O, Stevanovic S, et al. Allele-specific motifs revealed by sequencing of self-peptides eluted from MHC molecules. Nature 1991; 351(6324): 290–6
Romagnoli P, Labhardt AM, Sinigaglia F. Selective interaction of Ni with an MHC-bound peptide. EMBO J 1991; 10(6): 1303–6
van den Broeke LT, Heffler LC, Tengvall-Linder M, et al. Direct Ni2+ antigen formation on cultured human dendritic cells. Immunology 1999; 96: 578–85
Fisher MM. Anaphylaxis to muscle relaxants: cross sensitivity between relaxants. Anaesth Intensive Care 1980; 8(2): 211–3
Vervloet D, Arnaud A, Vellieux P, et al. Anaphylactic reactions to muscle relaxants under general anesthesia. J Allergy Clin Immunol 1979; 63(5): 348–53
Baldo BA, Harle DG. Drug allergenic determinants. In: Baldo BA, editor. Molecular approaches to the study of allergens. Monographs in allergy. Basel: Karger, 1990: 11–51
Birnbaum J, Vervloet D. Allergy to muscle relaxants. Clin Rev Allergy 1991; 9(3–4): 281–93
Leynadier F, Dry J. Anaphylaxis to muscle-relaxant drugs: study of cross-reactivity by skin tests. Int Arch Allergy Appl Immunol 1991; 94(1–4): 349–53
Fisher MM, Harle DG, Baldo BA. Anaphylactoid reactions to narcotic analgesics. Clin Rev Allergy 1991; 9(3–4): 309–18
Fisher MM, Baldo BA. The diagnosis of fatal anaphylactic reactions during anaesthesia: employment of immunoassays for mast cell tryptase and drug-reactive IgE antibodies. Anaesth Intensive Care 1993; 21(3): 353–7
Levy JH. Allergic reactions during anesthesia [clinical conference]. J Clin Anesth 1988; 1(1): 39–46
Stellato C, de Paulis A, Cirillo R, et al. Heterogeneity of human mast cells and basophils in response to muscle relaxants. Anesthesiology 1991; 74(6): 1078–86
Fisher MM. Clinical observations on the pathophysiology and treatment of anaphylactic cardiovascular collapse. Anaesth Intensive Care 1986; 14(1): 17–21
Fisher M. Treatment of acute anaphylaxis [(see comments) published erratum appears in BMJ 1995 Oct 7; 311(7010): 937]. BMJ 1995; 311(7007): 731–3
Ring J, Messmer K. Incidence and severity of anaphylactoid reactions to colloid volume substitutes. Lancet 1977; I(8009): 466–9
Douglas DM, Sukenick E, Andrade WP, et al. Biphasic systemic anaphylaxis: an inpatient and outpatient study. J Allergy Clin Immunol 1994; 93(6): 977–85
Leynadier F, Pecquet C, Dry J. Anaphylaxis to latex during surgery. Anaesthesia 1989; 44(7): 547–50
Moneret-Vautrin DA, Laxenaire MC. Anaphylactic and anaphylactoid reactions: clinical presentation. Clin Rev Allergy 1991; 9(3–4): 249–58
Laxenaire MC, Charpentier C, Feldman L. Anaphylactoid reactions to colloid plasma substitutes: incidence, risk factors, mechanisms: aFrench multicenter prospective study [(see comments) in French]. Ann Fr Anesth Reanim 1994; 13(3): 301–10
Steiner DJ, Schwager RG. Epidemiology, diagnosis, precautions, and policies of intraoperative anaphylaxis to latex [see comments]. J Am Coll Surg 1995; 180(6): 754–61
Cardot E, Tillie-Leblond I, Jeannin P, et al. Anaphylactic reaction to local administration of rifamycin SV. J Allergy Clin Immunol 1995; 95 (1 Pt 1): 1–7
Laxenaire MC, Mouton C, Frederic A, et al. Anaphylactic shock after tourniquet removal in orthopedic surgery [abstract]. Ann Fr Anesth Reanim 1996; 15(2): 179–84
Watkins J. Immediate hypersensitivity-type reactions in anaesthesia: allergy or otherwise, a problem or an overstatement. Theor Surg 1991; 6: 229–35
Lorenz W, Neugebauer E, Uvnas B, et al. Munich consensus development conference on histamine determination. In: Uvnas B, editor. Handbook of experimental pharmacology, histamine and histamine antagonists. Berlin: Springer-Verlag, 1991: 81–92
Matsson P, Enander I, Andersson AS, et al. Evaluation of mast cell activation (tryptase) in two patients suffering from druginduced hypotensoid reactions. Agents Actions 1991; 33(1–2): 218–20
Veien M, Szlam F, Holden JT, et al. Mechanisms of nonimmunological histamine and tryptase release from human cutaneous mast cells. Anesthesiology 2000; 92: 1074–81
Moneret-Vautrin DA, Laxenaire MC. Anaphylaxis to muscle relaxants: predictive tests [letter]. Anaesthesia 1990; 45(3): 246–7
Fisher MM, Baldo BA. Persistence of allergy to anaesthetic drugs. Anaesth Intensive Care 1992; 20(2): 143–6
Laxenaire MC, Moneret-Vautrin DA. Le risque allergique en anesthésie-réanimation. In: Lemaire F, Desmonts JM, editors. Collection d’Anesthésiologie et de Réanimation. Paris: Masson, 1990:1–154
Fisher MM, Bowey CJ. Intradermal compared with prick testing in the diagnosis of anaesthetic allergy. Br J Anaesth 1997; 79(1): 59–63
Moneret-Vautrin DA, Laxenaire MC. Skin tests in diagnosis of allergy to muscle relaxants and other anaesthetic drugs. In: Assem ES, editor. Allergic reactions to anaesthetics: clinical and basic aspects. Basel: Karger, 1992: 145–55
Galletly DC. Comparative cutaneous histamine release by neuromuscular blocking agents. Anaesth Intensive Care 1986; 14(4): 365–9
Laxenaire MC, Gastin I, Moneret-Vautrin DA, et al. Cross-reactivity of rocuronium with other neuromuscular blocking agents. Eur J Anaesthesiol Suppl 1995; 11: 55–64
Moneret-Vautrin DA, Gueant JL, Kamel L, et al. Anaphylaxis to muscle relaxants: cross-sensitivity studied by radioimmunoassays compared to intradermal tests in 34 cases. J Allergy Clin Immunol 1988; 82 (5 Pt 1): 745–52
McKinnon RP, Wildsmith JA. Histaminoid reactions in anaesthesia. Br J Anaesth 1995; 74(2): 217–28
Assem ES. Anaphylactic anaesthetic reactions: the value of paper radioallergosorbent tests for IgE antibodies to muscle relaxants and thiopentone. Anaesthesia 1990; 45(12): 1032–8
Gueant JL, Mata E, Monin B, et al. Evaluation of a new reactive solid phase for radioimmunoassay of serum specific IgE against muscle relaxant drugs. Allergy 1991; 46(6): 452–8
Gueant JL, Masson C, Laxenaire MC. Biological tests for diagnosing the IgE-mediate allergy to anaesthetic drugs. In: Assem K, editor. Monographs in allergy. Basel: Karger, 1992: 94–107
Guilloux L, Ricard-Blum S, Ville G, et al. A new radioimmunoassay using a commercially available solid support for the detection of IgE antibodies against muscle relaxants. J Allergy Clin Immunol 1992; 90(2): 153–9
Guilloux L, Richard-Blum S, Ville G, et al. Histamine release assay and radioimmunoassay for the detection of IgE antibodies against neuromuscular blocking drugs. Ann Fr Anesth Reanim 1993; 12(2): 182–6
Gueant JL, Mata E, Monin B. Evaluation clinique et biologique d’un test radio-immunologique de détection des IgE sériques spécifiques des curarisants. In: Galteau M, Siest G, Henny J, editors. Biologic prospective. Paris: Libbey Eurotext, 1989: 737–40
Moneret-Vautrin DA, Widmer S, Gueant JL, et al. Simultaneous anaphylaxis to thiopentone and a neuromuscular blocker: a study of two cases. Br J Anaesth 1990; 64(6): 743–5
Gueant JL, Mata E, Masson C, et al. Non-specific cross-reactivity of hydrophobic serum IgE to hydrophobic drugs. Mol Immunol 1995; 32(4): 259–66
Moneret-Vautrin DA, Finet JF, Maria Y. L’allergie au latex. Revue Française d’Allergologie 1988; 183: 235–6
Mata E, Gueant JL, Moneret-Vautrin DA, et al. Clinical evaluation of in vitro leukocyte histamine release in allergy to muscle relaxant drugs. Allergy 1992; 47(5): 471–6
Sainte-Laudy J, Vallon C, Guerin JC. Analysis of membrane expression of the CD63 human basophil activation marker: applications to allergologic diagnosis [in French]. Allerg Immunol (Paris) 1994; 26(6): 211–4
Abuaf N, Rajoely B, Ghazouani E, et al. Validation of a flow cytometric assay detecting in vitro basophil activation for the diagnosis of muscle relaxant allergy. J Allergy Clin Immunol 1999; 104 (2 Pt 1): 411–8
Laroche D, Bricard H, Laxenaire MC. Allergo-anesthesia consultation: not enough patients are tested after an anaphylactoid anesthetic incident [(letter; comment) in French]. Ann Fr Anesth Reanim 1998; 17(1): 89–90
Fisher MM. The prevention of second anaphylactoid reactions to anaesthetic drugs. Anaesth Intensive Care 1981; 9(3): 242–6
Charpin D, Benzarti M, Hemon Y, et al. Atopy and anaphylactic reactions to suxamethonium. J Allergy Clin Immunol 1988; 82 (3 Pt 1): 356–60
Guldager H, Sondergaard I. Histamine release from basophil leukocytes in asthma patients after in vitro provocation with various neuromuscular blocking drugs and intravenous anaesthetic agents. Acta Anaesthesiol Scand 1987; 31(8): 728–9
Akagi K, Townley RG. Spontaneous histamine release and histamine content in normal subjects and subjects with asthma. J Allergy Clin Immunol 1989; 83(4): 742–9
Laxenaire M, Mata E, Guéant J, et al. Basophil histamine release in atopic patients after in vitro provocation with thiopental, diprivan and chlormethiazole. Acta Anaesthesiol Scand 1991; 35: 706–10
Naguib M, Samarkandi AH, Bakhamees HS, et al. Histaminerelease haemodynamic changes produced by rocuronium, vecuronium, mivacurium, atracurium and tubocurarine [see comments]. Br J Anaesth 1995; 75(5): 588–92
Fuchs T, Spitzauer S, Vente C, et al. Natural latex, grass pollen, and weed pollen share IgE epitopes. J Allergy Clin Immunol 1997; 100(3): 356–64
Moneret-Vautrin DA, Beaudouin E, Widmer S, et al. Prospective study of risk factors in natural rubber latex hypersensitivity. J Allergy Clin Immunol 1993; 92(5): 668–77
Kelly KJ, Pearson ML, Kurup VP, et al. Acluster of anaphylactic reactions in children with spina bifida during general anesthesia: epidemiologic features, risk factors, and latex hypersensitivity. J Allergy Clin Immunol 1994; 94(1): 53–61
Konrad C, Fieber T, Gerber H, et al. The prevalence of latex sensitivity among anesthesiology staff. Anesth Analg 1997; 84(3): 629–33
Lebenbom-Mansour MH, Oesterle JR, Ownby DR, et al. The incidence of latex sensitivity in ambulatory surgical patients: a correlation of historical factors with positive serum immunoglobin E levels [see comments]. Anesth Analg 1997; 85(1): 44–9
Cuesta-Herranz J, de las Heras M, Fernandez M, et al. Allergic reaction caused by local anesthetic agents belonging to the amide group [see comments]. J Allergy Clin Immunol 1997; 99(3): 427–8
Ismail K, Simpson PJ. Anaphylactic shock following intravenous administration of lignocaine. Acta Anaesthesiol Scand 1997; 41(8): 1071–2
Fisher MM, Bowey CJ. Alleged allergy to local anaesthetics. Anaesth Intensive Care 1997; 25(6): 611–4
Clendenen SR, Harper JV, Wharen Jr RE, et al. Anaphylactic reaction after cisatracurium. Anesthesiology 1997; 87(3): 690–2
Leynadier F, Calinaux C, Dry J. Predictive value of intradermal tests using muscle-relaxing drugs [in French]. Ann Fr Anesth Reanim 1989; 8(2): 98–101
Thacker MA, Davis FM. Subsequent general anaesthesia in patients with a history of previous anaphylactoid/anaphylactic reaction to muscle relaxant. Anaesth Intensive Care 1999; 27(2): 190–3
Fisher MM. Anaphylactoid reactions during anaesthesia. In: Prys-Roberts C, editor. International practice of anaesthesia. Oxford: Butterworth-Heinemann, 1996: 1–13
Fisher MM, Merefield D, Baldo B. Failure to prevent an anaphylactic reaction to a second neuromuscular blocking drug during anaesthesia. Br J Anaesth 1999; 82(5): 770–3
Shenot P, Rivas DA, Kaiman DD, et al. Latex allergy manifested in urological surgery and care of adult spinal cord injured patients. Arch Phys Med Rehabil 1994; 75(11): 1263–5
Ellsworth PI, Merguerian PA, Klein RB, et al. Evaluation and risk factors of latex allergy in spina bifida patients: is it preventable? J Urol 1993; 150 (2 Pt 2): 691–3
Slater JE. Rubber anaphylaxis [see comments]. N Engl J Med 1989; 320(17): 1126–30
Bouaziz H, Laxenaire MC. Anaesthesia for the allergic patient. Current Opinion in Anaesthesiology 1998; 11: 339–44
Tarlo SM, Sussman GL, Holness DL. Latex sensitivity in dental students and staff: a cross-sectional study. J Allergy Clin Immunol 1997; 99(3): 396–401
Mazon A, Nieto A, Estornell F, et al. Factors that influence the presence of symptoms caused by latex allergy in children with spina bifida. J Allergy Clin Immunol 1997; 99(5): 600–4
Porri F, Pradal M, Lemiere C, et al. Association between latex sensitization and repeated latex exposure in children. Anesthesiology 1997; 86(3): 599–602
Ylitalo L, Turjanmaa K, Palosuo T, et al. Natural rubber latex allergy in children who had not undergone surgery and children who had undergone multiple operations. J Allergy Clin Immunol 1997; 100(5): 606–12
Brehler R, Theissen U, Mohr C, et al. ‘Latex-fruit syndrome’: frequency of cross-reacting IgE antibodies. Allergy 1997; 52(4): 404–10
Youngman PR, Taylor KM, Wilson JD. Anaphylactoid reactions to neuromuscular blocking agents: a commonly undiagnosed condition? Lancet 1983; II(8350): 597–9
Assem ES, Ling YB. Fatal anaphylactic reaction to suxamethonium: new screening test suggests possible prevention [see comments]. Anaesthesia 1988; 43(11): 958–61
Brahams D. Fatal reaction to suxamethonium: case for screening by radioallergosorbent test? [see comments]. Lancet 1989; 1(8651): 1400–1
Porri F, Lemiere C, Birnbaum J, et al. Prevalence of latex sensitization in subjects attending health screening: implications for a perioperative screening. Clin Exp Allergy 1997; 27(4): 413–7
Ostergaard D, Engbaek J, Viby-Mogensen J. Adverse reactions and interactions of the neuromuscular blocking drugs. Med Toxicol Adverse Drug Exp 1989; 4(5): 351–68
Fisher MM, Brady PW. Adverse reactions to plasma volume expanders. Drug Saf 1990; 5(2): 86–93
Lorenz W, Röhrer HD, Doenicke A. Histamine release in anaesthetic and surgery: a new method to evaluate its clinical significance with several types of causal relationship. Clin Anaesthesiol 1984; 2: 403–26
Fisher M. Direct histamine release in anaesthesia and surgery: unanswered questions. Theor Surg 1988; 3: 145–7
Hobsley M, Moss J, Levi R, et al. Discussion forum about a protocol of a controlled clinical trial: induction of anaesthesia and perioperative risk. Theor Surg 1988; 3: 55–77
Lorenz W, Ennis M, Doenicke A, et al. Perioperative uses of histamine antagonists [published erratum appears in J Clin Anesth 1991 Mar-Apr; 3 (2): 170]. J Clin Anesth 1990; 2(5): 345–60
Schwartz A, Sutton SL, Askenase PW, et al. Histamine inhibition of concanavalin A-induced suppressor T-cell activation. Cell Immunol 1981; 60(2): 426–39
Lichtenstein LM, Gillespie E. Inhibition of histamine release by histamine controlled by H2 receptor. Nature 1973; 244(5414): 287–8
Hutchcroft BJ, Moore EG, Orange RP. The effects of H1- and H2-receptor antagonism on the response of monkey skin to intradermal histamine, reverse-type anaphylaxis, and passive cutaneous anaphylaxis. J Allergy Clin Immunol 1979; 63(6): 376–82
Meyrick Thomas RH, Browne PD, Kirby JDT. The effect of ranitidine, alone and in combination with clemastine, on allergen-induced cutaneous wheal-and-flare reaction in human skin. J Allergy Clin Immunol 1985; 76(6): 864–9
Koga Y, Iwatsuki N, Hashimoto Y. Direct effects of H2-receptor antagonists on airway smooth muscle and on responses mediated by H1- and H2-receptors. Anesthesiology 1987; 66: 181–5
Ring J, Behrendt H. H1- and H2-antagonists in allergic and pseudoallergic diseases. Clin Exp Allergy 1990; 20 Suppl. 2: 43–9
Lorenz W, Doenicke A. H1 and H2 blockade: a prophylactic principle in anaesthesia and surgery against histamine-release responses of any degree of severity: pt II. N Engl Reg Allergy Proc 1985; 6(2): 174–94
Dorsch W, Reimann HJ, Neuhauser J. Histamine l-histamine2 antagonism: effect of combined clemastine and cimetidine pretreatment on allergen and histamine-induced reactions of the guinea pig lung in vivo and in vitro. Agents Actions 1982; 12(1–2): 113–8
Lieberman P. The use of antihistamines in the prevention and treatment of anaphylaxis and anaphylactoid reations. J Allergy Clin Immunol 1990; 86: 684–6
Lorenz W, Doenicke A, Schoning B, et al. H1 + H2-receptor antagonists for premedication in anaesthesia and surgery: a critical view based on randomized clinical trials with Haemaccel and various antiallergic drugs. Agents Actions 1980; 10 (1 Pt2): 114–24
Philbin DM, Moss J, Akins CW, et al. The use of H1 and H2 histamine antagonists with morphine anesthesia: a doubleblind study. Anesthesiology 1981; 55(3): 292–6
Hosking MP, Lennon RL, Gronert GA. Combined H1 and H2 receptor blockade attenuates the cardiovascular effects of highdose atracurium for rapid sequence endotracheal intubation. Anesth Analg 1988; 67(11): 1089–92
Doenicke A, Moss J, Lorenz W, et al. Effect of oral antihistamine premedication on mivacurium-induced histamine release and side effects. Br J Anaesth 1996; 77(3): 421–3
Renz CL, Laroche D, Thurn JD, et al. Tryptase levels are not increased during vancomycin-induced anaphylactoid reactions. Anesthesiology 1998; 89(3): 620–5
Renz CL, Thurn JD, Finn HA, et al. Antihistamine prophylaxis permits rapid vancomycin infusion [see comments]. Crit Care Med 1999; 27(9): 1732–7
Moss J, Roizen MF, Nordby EJ, et al. Decreased incidence and mortality of anaphylaxis to chymopapain. Anesth Analg 1985; 64(12): 1197–201
Lorenz W, Duda D, Dick W, et al. Incidence and clinical importance of perioperative histamine release: randomised study of volume loading and antihistamines after induction of anaesthesia. Trial Group Mainz/Marburg [see comments]. Lancet 1994; 343(8903): 933–40
Dahl JB. Antihistamine prophylaxis and general anaesthesia [see comments]. Lancet 1994; 343(8903): 929–30
Setlock MA, Cotter TP, Rosner D. Latex allergy: failure of prophylaxis to prevent severe reaction. Anesth Analg 1993; 76(3): 650–2
Kwittken PL, Sweinberg SK, Campbell DE, et al. Latex hypersensitivity in children: clinical presentation and detection of latex-specific immunoglobulin E. Pediatrics 1995; 95: 693–9
Powell JA, Maycock EJ. Anaphylactoid reaction to ranitidine in an obstetric patient. Anaesth Intensive Care 1993; 21(5): 702–3
Patterson LJ, Milne B. Latex anaphylaxis causing heart block: role of ranitidine. Can J Ansth 1999; 46(8): 776–8
McKinnon RP. Allergic reactions during anaesthesia. Curr Opin Anaesthesiol 1996; 9: 267–70
Birnbaum J, Porri F, Pradal M, et al. Allergy during anaesthesia. Clin Exp Allergy 1994; 24(10): 915–21
Ljungstrom KG, Willman B, Hedin H. Hapten inhibition of dextran anaphylaxis. Nine years of post-marketing surveillance of dextran 1. Ann Fr Anesth Reanim 1993; 12(2): 219–22
Ljungstrom KG, Renck H, Hedin H, et al. Hapten inhibition and dextran anaphylaxis. Anaesthesia 1988; 43(9): 729–32
Hedin H, Ljungstrom KG. Prevention of dextran anaphylaxis: ten years experience with hapten dextran. Int Arch Allergy Immunol 1997; 113 (1–3): 358–9
Berg EM, Fasting S, Sellevold OF. Serious complications with dextran-70 despite hapten prophylaxis: is it best avoided prior to delivery? Anaesthesia 1991; 46(12): 1033–5
Vervloet D, Arnaud A, Senft M, et al. Anaphylactic reactions to suxamethonium: prevention of mediator release by choline. J Allergy Clin Immunol 1985 (76): 222–5
Thomas H, Eledjam JJ, Macheboeuf M, et al. Rapid pre-operative immunotherapy in a patient allergic to muscle relaxants. Eur J Anaesthesiol 1988; 5(6): 385–9
Moneret-Vautrin DA, Kanny G, Gueant JL, et al. Prevention by monovalent haptens of IgE-dependent leucocyte histamine release to muscle relaxants. Int Arch Allergy Immunol 1995; 107(1–3): 172–5
Moneret-Vautrin DA, Laxenaire MC. Routine testing for latex allergy in patients with spina bifida [reply]. Anesthesiology 1991; 74: 391–2
Ebo DG, Stevens WJ, Bridts CH, et al. Latex-specific IgE, skin testing, and lymphocyte transformation to latex in latex allergy. J Allergy Clin Immunol 1997; 100(5): 618–23
Porri F, Pradal M, Rud C, et al. Is systematic preoperative screening for muscle relaxant and latex allergy advisable? Allergy 1995; 50(4): 374–7
Theissen JL, Zahn P, Theissen U, et al. Allergic and pseudo-allergic reactions in anesthesia. I: pathogenesis, risk factors, substances [in French]. Anasthesiol Intensivmed Notfallmed Schmerzther 1995; 30(1): 3–12
SFAR. Indications de la curarisation en Anesthésie. Conférence de Consensus. Texte court. Société Française d’Anesthésie et de Réanimation; 1999 Jul 12; Saint-Mandé. Available from: URL: http://www.sfar.org/curarisationccons.html [Accessed 2000 May 16]
Birmingham PK, Dsida RM, Grayhack JJ, et al. Do latex precautions in children with myelodysplasia reduce intraoperative allergic reactions?J Pediatr Orthop 1996; 16(6): 799–802
Holzman RS. Clinical management of latex-allergic children. Anesth Analg 1997; 85(3): 529–33
Heilman DK, Jones RT, Swanson MC, et al. A prospective, controlled study showing that rubber gloves are the major contributor to latex aeroallergen levels in the operating room. J Allergy Clin Immunol 1996; 98(2): 325–30
Laxenaire MC. Choc anaphylactique peranesthésique: conduite à tenir. Ann Fr Anesth Reamin 1997; 16(7): 2–4
Laxenaire MC, Moneret-Vautrin DA. Immunology: allergy and anaesthesia. Oether 1994; I: 14–18
The use of epinephrine in the treatment of anaphylaxis: American Academy of Allergy and Immunology board of Directors. Clin Immunol 1994; 94: 666-8
Ewan PW. Anaphylaxis [published erratum appears in BMJ 1998 May 23; 316 (7144): 1507]. BMJ 1998; 316(7142): 1442–5
Heilborn H, Hjemdahl P, Daleskog M, et al. Comparison of subcutaneous injection and high-dose inhalation of epinephrine: implications for self-treatment to prevent anaphylaxis. J Allergy Clin Immunol 1986; 78(6): 1174–9
Simons FE, Roberts JR, Gu X, et al. Epinephrine absorption in children with a history of anaphylaxis. J Allergy Clin Immunol 1998; 101 (1 Pt 1): 33–7
Plomley RF, Czarny D. Inhaled adrenaline in the treatment of anaphylaxis [letter]. Med J Aust 1988; 149(10): 564
Powers RD, Donowitz LG. Endotracheal administration of emergency medications. South Med J 1984; 77(3): 340–1
Powers RD, Donowitz LG. Endotracheal administration of emergency medications. South Med J 1984; 77(3): 346 — afeter 178
Alexander R, Pappachan R, Smith GB, Taylor BL. Treatment of acute anaphylaxis: avoid subcutaneous or intramuscular adrenaline [letter; comment]. BMJ 1995; 311(7017): 1434–5
Campbell S. Treatment of acute anaphylaxis: expressing the dose of adrenaline in milligrams is easier [letter; comment]. BMJ 1995; 311(7017): 1435
Raper RF, Fisher MM. Profound reversible myocardial depression after anaphylaxis. Lancet 1988; I(8582): 386–8
Levy JH. New concepts in the treatment of anaphylactoid reactions in anesthesia. Ann Fr Anesth Reanim 1993; 12(2): 223–7
Mitsuhata H, Shimizu R, Yokoyama MM. Role of nitric oxide in anaphylactic shock. J Clin Immunol 1995; 15(6): 277–83
Compton J. Use of glucagon in intractable allergic reactions and as an alternative to epinephrine: an interesting case review. J Emerg Nurs 1997; 23(1): 45–7
Lee ML. Glucagon in anaphylaxis [letter]. J Allergy Clin Immunol 1982; 69(3): 331–2
Zaloga GP, DeLacey W, Holmboe E, et al. Glucagon reversal of hypotension in a case of anaphylactoid shock. Ann Intern Med 1986; 105(1): 65–6
Schleimer RP. The mechanisms of antiinflammatory steroid action in allergic diseases. Annu Rev Pharmacol Toxicol 1985; 25: 381–412
Runge JW, Martinez JC, Caravati EM, et al. Histamine antagonists in the treatment of acute allergic reactions. Ann Emerg Med 1992; 21(3): 237–42
De Soto H, Turk P. Cimetidine in anaphylactic shock refractory to standard therapy. Anesth Analg 1989; 69: 260–9
Kambam JR, Merrill WH, Smith BE. Histamine-2 receptor blocker in the treatment of protamine related anaphylactoid reactions: two case reports. Can J Anaesth 1989; 36(4): 463–5
Kelly JS, Prielipp RC. Is cimetidine indicated in the treatment of acute anaphylactic shock. Anesth Analg 1990; 71: 104–5
Acknowledgements
We thank Professor D. Longrois and Dr W. Canada for their help in reviewing this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mertes, P.M., Laxenaire, MC. Anaphylaxis During General Anaesthesia. Mol Diag Ther 14, 115–133 (2000). https://doi.org/10.2165/00023210-200014020-00003
Published:
Issue Date:
DOI: https://doi.org/10.2165/00023210-200014020-00003