
Summary
Synopsis
Ceftriaxolle possesses a broad spectrum of antimicrobial activity that indudes the Gram-positive and Gra-Negative aerobes commonly associated with serious infections. lts therapeutic efficacy is comparable to that of other third-generation cephalosporins and aminoglycoside-combinalion regimens. The most commonly reported adverse events with ceftriaxone are similar in incidence and severity to those reported with other third-generation cephalosporins. Notably, the drug has a favourable pharcokinetic profile which allows once-daily administration.
In comparative studies with other parenteral regimens requiring 3 10 6 daily doses, treatment with once,daily ceftrioxone reduced total antimicrobial drug costs (i.e. acquisition, preparation and administration costs) by 17 to 52%. Ceftriaxone was also more cost effective than ceftazidime and a variety of other antimicrobial treatment regimem (penicillins, cephaosporins, combination regimens) in the treatment a patients with community-acquired pneumonia or bronchopneumonia. This reflected lower drug and hospitalisation costs associated with a reduced length of hospital stay in ceftriaxone recipients.
In noncomparative studies, ceftriaxone achieved considerable hospitalisation cost savings in patients with serious infections (mostly bone, joint, skin/skin structure infections), who were able to receive all or part of their antimicrobial therapy as patients. In one analysis which evaluated all direct and indirect costs (such as training programmes, transportation, time for visits and supplies) and benefits (such as hospitalisation cost savings, return to work or school, increased productivity) of outpatient ceftriaxone therapy, the overall benefit-cost ratio was approximately 5 : 1.
The studies to date confirm that ceftriaxone is effective, well tolerated, convenient a administer and, when utilised appropriately, offers the potenial for cost avoidance in patients with serious infections. Although additional well designed pharmacoeonomic analyses are needed to further evaluate its cost effectiveness, ceftriaxone should be considered an essential third-generaion cephalolporin formulary, represetative in most clinical settings.
Diseose and Treatment Considerations
Treatment of serious infections traditionally requires hospitalisation and administration of intravenous antimicrobial agents. Besides hospitalisation costs, the major factors contributing toward the total direct costs of treatment include antimicrobial drug acquisition and administration costs, monitoring costs and costs arising from adverse effects or treatment failure. For some infections (e.g. osteomyelitis, skin/skin structure infections, bacterial endocarditis), clinically stable patients usually remain in hospital for extended periods of time solely to receive parenteral antimicrobials.
Ceftriaxone is a third-generation cephalosporin with a broad spectrum of activity in vitro which includes Gram-positive and Gram-negative aerobic and some anaerobic bacteria. Following parenteral administration of therapeutic dosages. ceftriaxone allains concentrations suffic ient to inhibit growth of the majority of bacteria in most body tissues and nuids. and has a plasma elimination half-life of around 8 hours. allowing once-daily administration.
Clinical trials havc shown that ceftriaxone is effective and well tolerated in eradicating susceptible bacteria in a wide range of serious infections, including those of the respiratory tract. blood. urinary tract, skin/skin structure. CSF, bone and joints. and infections in neutropenic patients. Data from comparative trials indicate that ceftriaxone is as effective as other third-generation cephalosporins and aminoglycoside/β-lactam combinations in treating serious infections in hospitalised patients. Like most other third-generation cephalosporins, ceftriaxone shou ld not be administered empirically in severe hospital-acquired infections of unknown aetiology if Pseudomonas aeruginosa is the suspected pathogen. Ceftriaxone has also demonstrated efficacy in treating adults and children with ostcomye litis, skin/skin structure infections. lower respiratory tract infections, urinary tract infections. infections in immunocompromised patients, bacteraemia and bacterial endocarditis in an outpatient setting (administered either entirely in the outpatient setting or after an initial period of hospitalisation).
Phormocoeconomic Benefits and Costs
The potential of ceftriaxone to save costs in hospitalised patients depends upon its comparable efficacy with other third-generation cephalosporins or combination regimens, and lower overall treatment costs as a result of its once-daily admi nistrat ion schedule. Preparation and administration costs and nursing time associated with once-daily administration of ceftriaxone are generally lower than those of antimicrobials which require mulliplc daily administrations.
The potential for the greatest cost avoidance may occur in patients who must remain hospitalised solely 10 receive parenteral antimicrobial treatment. With its convenient administration schedule, ceftriaxone offers the potential for significant cost avoid.mce in patients who are able to complete all or part of their antimicrobial regimen in an outpatient selling. The largest cost savi ngs will be realised in countries wi th national health insurance schemes or. in the US. in those institutions with a high proportion of prospective payment status patients. However, the lack of adequate insurance coverage or government restrictions related to outpatient administration of antimicrobials may be a deterrent for some patients.
Since ceftriaxone is generally well tolerated, the costs associated with adverse events are not expected to be significant, although studies which include these costs in their pharmacoeconomic analysis are needed to confirm this, Ceftriaxone monotherapy eliminates the costs associated with plasma drug concentration monitoring as well as the risk of additional costs incurred as a result of aminoglycoside toxicity.
Pharmocoeconomic Analyses
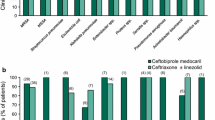
Cost-minimisation analyses in hospitali sed patients showed that once-daily ceftriaxone, when compared with antimicrobial regimens requiring 3 to 6 daily doses, reduced total antimicrobial drug COStS by 17 to 52% and saved approximately 40 min/day of nursing lime associated with parenteral therapy administration. In 3 comparisons in palients with community-acquired pneumonia, ceftriaxone was more cost effective than ceftazidime and a variety of other antimicrobial treatment regimens (penicillins, cephalosporins, combination regimens) as a result of lower drug and hospitalisation costs associated with a reduced length of hospital stay. However, the reliability of 2 of these studies was compromised by use of comparator agents which may not have provided adequate antibacterial activity for the treatment of community-acquired pneumonia: the refore more studies are needed before any definitive conclusions can be drawn about the effect of ceftriaxone treatment on the length of stay hospital.
Ceftriaxone offers a convenient administration schedule for parenteral therapy in outpatient settings. Charges associated with ceftriaxone outpatient treatment (emergency room visits, laboratory tests and hospitalisation) in febrile children with sickle cell disease were SUS 1195 lower per febrile episode than those associated with inpatient treatment. In noncomparative retrospective studies, significant hospitalisation cost savings (range $US4354 to $US7800 per patient) were realised when patients received some or all of their treatment with ccftriaxone as outpatients. A benefit-cost ratio of 5:1 was calculated for outpatient ceftriaxone treatment when costs associated with transponation, training programmes, supplies, time for outpatient visits. hospitalisation and increased productivity were evaluated.
In the outpatient studies discussed above, it was unclear how hospitalisation costs were determined and none of these analyses included costs of adverse effects or treatment failure. Thus, well designed comparative studies with other antimicrobials are needed 10 further facilitate the pharmacocconomic positioning of ceftriaxone in the outpatient setting.
Ceftriaxone is effective and well tolerated, and possesses a favourable pharmacokinetic profile which allows once-daily administration. Although the decision to grant formulary status to a particular third-generation cephalosporin should be based on institution-specific data regarding acquisition, administration and hospitalisation costs and antimicrobial susceptibilities, the available data suggests that ceflriaxone offers the potential for cost savings in the treatment of hospitalised patients and outpatients with serious infections.
Similar content being viewed by others

References
Gladen HE. Evaluating the cost-effectiveness of treatment with third generation cephalosporins. Diagn Microbiol Infect Dis 1992; 15: 99–105
Guglielmo BJ. Brooks GF. Antimicrobial therapy. Cost-benefit considerations. Drugs 1989: 38: 473–80
Foran RM, Brett JL, Wulf PH. Evaluating the cost impact of intravenous antibiotic dosing frequencies. Drug Intell Clin Pharm 1991; 25; 546–51
Plumridge RJ. Cost comparison of intravenous antibiotic administration. Med J Aust 1990: 153: 516–8
Tanner DJ. Cost containment of reconstituted parenteral antibiotics: personnel and supply costs associated with preparation.dispensing, and administration. Rev Infect Dis 1984: 6 Suppl.4: 924–37
Tanner DJ. Nazarian MQ. Cost containment associated with decreased parenteral antibiotic administration frequencies.AmJ Med 1984: 148: 104–11
Balinsky W, Nesbitt S. Cost-effectiveness of out patient antibiotics: a review of the literature. Am J Med 1989: 87: 301–5
Finkler SA. The distinction between cost and charges. Ann Intern Med 1982: 96: 102–9
Chamberlain TM,Lechman ME, Groh MJ. et al. COSt analysis of a home intravenous antibiotic program. Am J Hosp Pharm 1988: 45: 2341–5
U.S. Bureau of tile Census. Statistical Abstract of the United States. 113th ed. Washington,DC: US Department of Commerce. 1993
Grizzard MB. Harris G. Karns H. Use of out patient parenteral antibiotic therapy in a health maintenance organization. Rev Infect Dis 1991: 13Suppl.2: 174–9
Tice AD. Once-daily ceftriaxone out patient therapy in adults with infections. Chemotherapy Basel 1990: 37 Suppl.3: 7–10
Jauregui LE. Martin M. Hageage G. Clinical evaluation of ceftriaxone therapy in an out patient setting.Insights into the treatment of Serious Infections 1988: 2: 186–94
Parker SE. Davey PG. Pharmacoeconomics of intravenous drug dministration. Pharmaco Economics 1992: 1 103–15
Garrelts JC. Smith DF. Ast D. et al. A comparison of the safety. timing and cost-effectiveness of administering antibiotics by intravenous bolus (push) versuS intrdvenous piggyback (slowinfusion) in surgical prophylaxis. Pharmaco Economics 1992:1 116–23
Kaplan JM. Gorebki SA, Keith S, et al. Cost of antibiotic therapy for infants and children. Pediatr Infect Dis J 1990: 9:722–8
Crane VS. Projected cost savings associated with cefmetazole. A new cephamycin for the hospitalized patient. Hosp Form 1991: 26: 302–10
Barriere SL. Eonomic impact of oral ciprofloxacin. Am J Med 1987: 82 Suppl.4A: 387–92
Cousins DH. Lee M. Stanaway M. et al. Implementation and evaluation of a centralised IV additive service for antibiotic injections. Pharm J 1989; 242 Suppl: 14–16
Huckleberry SD. Antibiotic cost-containment. Drug Intell Clin Pharm 1986; 20; 589–91
Dziebra SH. Reilly RT. Caselnova DA. Cost savings achieved through cephaloporin use review and restriction. Am J Hosp Pharm 1986: 43: 2194–7
Avron J. Soumerai SB. Taylor MD, et al. Reduction of incorrect antibiotic dosing through a structured educational order form. Arch Intern Med 1988: 148: 1720–4
Quintiliani R, Cooper BW, Briceland LL. et al. Economic impact of stream lining antibiotic administration. Am J Med 1987:82 Suppl 4A: 391–4
Bamberger OM. Dahl SL. Impact of voluntary vs enforced compliance of third-generation cephalosporin use in a teaching hospital. Arch Intern Med 1992; 152: 554–7
Karki SD, Holden JMC, Mariano E. A team approach to reduce antibiotic costs. Drug Intell Clin Pharm 1990: 24: 202–5
Coleman RW. Rodondi L. Kaubisch S. et al. Cost-effectiveness of prospective and continuous parenteral antibiotic control:experience at the Palo Alto Veterans Affairs Medical Center from 1987 to 1989. Am J Med 1991.90: 439–44
Schentag JJ. The results of 3 targeted pharmacy intervention program. Clin Ther 1993; 15 Suppl. A; 29–36
Meyer RD. Risk factors and comparisons of clinical nephroloxicity of aminoglycosides. Am J Med 1986; 80 Suppl.66: 119
Gatell JM. Ferran F. Araujo V. eI al. Univariate and muilivariate analysis of risk factors predisposing to auditor toxictly in patients receiving aminoglycosides. Antimicrob Agents Chemother 1987: 31: 1383
Mathews A. Bailie GR. Clinical pharmacokinetics. toxicity and cost effectiviness analysis of aminoglycosides and aminoglycoside dosing services. J Clin Pharm Ther 1987: 12: 273–91
Eisenberg JM. Koffer B. Glick HA. et al. What is the cost of nepphroloxicity associated with aminoglycosides? Ann Intern Med 1987; 107: 900–9
Cunha BA. Third-genereration cephalosporins: a review. Clin Ther 1992: 14: 616–52
Chambers ST. Which cephalosporins: a review.Clin Ther 1992; 105: 498–500
Cano SB. Fujita NK. Formulaary evauluation or third-generation cephalosporins using decision analysis. Am J Hosp Pham.1988: 45: 566–9
Barriere SL. Flaherty JF. Third-generation cephulosporins: a critical evaluation. Am J Hosp Pharm 1984: 3: 351–73
Jones RN.Summation. Diagn Microbiol Infect Dis 1992: 15: 107–8
Eriksen NL. Blanca JD. Extended-spectrum (second-and third generation) cephalosporins. Obstet Gynerol Clin North Am 1992: 19:461–74
Meyers BR. Comprarative toxidlies of third generation cephalosporins. Am J Med 1985; 79 Suppl.2A: 96–103
Brogden RN. Ward A. Ceftriaxone. A reaappraisal of its antibacterial activity and pharmacokinetic, properties, and an update on its therapeutic use with particular reference to once-daily administration. Drugs 1988: 35: 604–45
National Committee for Clinical Laboratory Standards. Performance standards for antimacrobial suseplibility testing;Fourth Information Supplement. Villanova (PA): NCCLS.1992. NCCLS Document M100-S4
Dever LA. Dermody TS. Mechanisms of bacterial resistance to antibiotics. Arch Intern Med 1991: 151: 886–95
Gancia-Rodriguez JA. Gancia Sanchez JE. bellido JL. et al. Current status of bacterial resistance to third-generation cephalsporins. Diagn Microbiol Infect Dis 1992: 15: 67–72
Jenkins SG. Compparative suscepibility patterns of common clinical isolateS to cefoperazone: 1981 to 1987. Am J Med 1988: 85 Suppl.IA: 52–5
Weinstein RA, Occurence of cefolaxime-resistance Enterobacter during therapy of cardiac surgery patients. Chimioterapia 1985: 4: 110–2
Ballow CH, Schentag JJ. Trends in antibiotic utilization and bacterial resistance, Report of the National Nosocomial Resistance Surveillance Group. Diagn Microbiol Infect Dis1992; 15: 37–42
Conus P. Francioli P. Relationship between cefatriaxone use and resistance of Enterobacecr species. J Clin Pharm Ther 1992:17: 303–5
Yuk JH. Nightingale CH. tQuintiliani R. Clinical pharmacokinetics of ceftriaxone. Clin Pharmacokinet 1989; 17: 223–35
Patel IH. Chen S. Parsonnet M. et al. Pharmacokinetics of ceftriaxone in humans. Amimicrob Agents Chemother 1981;20: 634–41
Yuk-Choi JH, Nightingale CH. Williams TW. Consideations in dosage seletion for third generation cephalosporins. Clin Pharmacokinet 1992; 22: 132–43
Eron LJ. Parenteral antibiotic therapy in oulpatients: quality assurance: and other issues, in a protohospital. Chemotherapy 1991; 37 Suppl.2: 14–20
Childs SJ. Wells WG. Mirelman S. Ceftriaxone: for once-a-day therapy of urinary tract infection. Am J Med 1984: 77: 73–5
Rothwell DL. Bremmer DA. Taylor KM. Treatment of complicated urinary tract infections with the long acting cephalosporin, ceftriaxone. N Z Med J 1983; 96: 392–4
Westenfelder M. Pelz K. Klinische studie zur prufung der Wirbamkcil und Vertnrglichkeit von Cefotaxim. CCefotaximund Ceflriuooc bei Patienten mit kompplizicnen Harnweginfecklionen. Infection 1983; 11: 296–301
Bailey RR. Lynn KL. Peddie BA. et al. Comparison of netilmicin with ceftriaxone for the treatmnent of !severe or complicated urinary trackk infections. N Z Med J 1986: 99: 459–61
Lepage JY. Juge C. Cozian A. et al. Comparative study of ceftriaxone and amikacin as first line therapy for severe urinary tract infections in adults. Pathol Biol 1987: 35: 638–41
Baumgartner JD. Glauser HP. Tolerance study of ceftriaxone compared wilh amoxicillin in patients with pneumonia. Am J Med 1984: 77: 54–9
McCabe R. Schlossberg D. Donowitz G. e t al. Cefonicid Versus ceftriaxone in the treatment of lower respiratory tract infectionsin patients with COPD. Proceedingsof 17th Conference of ICAAC. New York. 1987
Barradas P. Zamith M. Videira W. et al. Therapy of lower respiratory track infections: a comparison of ceftriaxone and cefotaxime. Chemotherapy Basel 1989: 35 Suppl.2: 33–40
Rascio N. Marseglia GL. Ugazio AG. The treatment of pneumonia in children: ceftriaxone vs amoxicillin plus.tobramycin.An open trial. Clin Trials J 1985: 22: 401–4
Fernez A. Prinz G. Szalka A. et al.Ceftriaxone versus cefotaxime in tlhe treatment of septicemia in adults. Chemotherapy Basel 1989: 35 Suppl. 2: 5–9
Ludwig E. Magyar T. Lanyl P. et al. Efficacy and safety of ceftriaxone + netilmicin once daily versus ceftazidime +netilmicin twice daily in Seveere nosocomial infections. Curr Ther Res 1993; 53: 687–93
Mandell LA. Bergeron MG. Ronald AR. et al. Once-daily therapy with ceftriaxone compared with daily multiple-dose therapy with cefataxime for serious baterial infections: a randomized, double-blind study. J Infect Dis 1989: 160:433–41
Smith CR. Petty BG. Hendrix CW et al. Ceftriaxone compared with cefotaxime for serious bacterial infections. J Infect Dis 1989; 160: 442–7
Bradsher R, Snow RM, Ceftriaxone treatment of skin and soft tissue infections in a once daily regimen. Am J Med 1984: 77:63–7
Gordin FM. Wofsy CB. Mills J. Once daily ceftriauxone for skin and soft tissue infections, Antimickrob Agents Chemother 1985: 27: 648–9
Bucaneve G. Mecnichetti F. Minitti V. et al. Ceftriaxone versus imipenem/cilastatin as empirical monotherapy for infections in cancer patients. Chemotherapy 1989; 35 Suppl. 2: 10–5
Gibson J. Johnson L. Snowdon L. et al. Single daily ceftriaxone and tobramycin in the empirical management of febrile neutropenic patients: a randomized trial. Int J Hematol 1993; 58:63–72
International Antimicrobial Therapy Cooperative of the European Organization for Research and Treatnent of Cancer.Efficacy and toxicity of single daily dOseS of amikacin and ceftriaxone versus multiple daily doses of amikacin and ceftazidime, for infection in patients with cancer and granulocytopenia. Ann Intern Med 1993: 19: 584-93
Maiche AG. Teerenhovi L. Empiric treatment of serious infections in patients; with cancer: a comparative study of two combinations of i.v and oral antibiotics. lnt J Exp Clin Chemother 1992; 5: 203–8
Oturai PS. Hollander NH. Hansen OP. et al. Ceftriaxone versus latamoxef in febrile neutropenic patients: empirica l mon-therapy in patients with solid tumours. Eur J Cancer 1993;29A: 1274–9
Ferrnex M. Havu L. Kissling M. Clinical trials with ceftriaxone: an analysis of 12803 publishing cases. Insights treat serious Infect 1988: 2: 207–27
Hughes WT, Armstrong D. Bodey GP. et al. Guidelines for the use of antimicrobial agents in neutropenic patienls with unexplained fever. J Infect Dis 1990; 161: 381–96
Eron LJ, Park CH. Hixon DH. e tal. Ceftriaxone therapy of bone and soft tissue infections in hospital and outpatient settings. Antimicrob Agents Chemother 1983: 23: 731–7
Stamboulian D, Bonvehi, P. Arevalo C, et al. Antibiotic management of out patients with endocarditis due to penicillin-susceptible streptococci. Rev Infect Dis 1991: 13 Suppl.2:I60–3
Francioli P. Etienne J. Hoigne R. et al. Treatment of Streptococcal endocarditis with a single daily dose of ceftriaxone sodium for 4 weeks. JAMA 1992; 267: 264–7
Karachalios GN, Georgiopoulos AN. Kanatakis S. Treatment of various infections in an outpatient practice by intramuscular ceftriaxone: home paRenteral thrapy. Chemotherapy 1989: 35: 389–92
Russo TA. Cook S. Gorbach SL Intralmascular ceftriaxone in home parenteral therapy. Antimicrob Agents Chemother1988; 32: 1439–40
Bass JW. Steele RW. Wittle RR. et al. Antimicrobial treatment of occult bacteremia: a mullicenter cooperative study. Pediatr Infect Dis J 1993; 12: 466–73
Baskin MN. O’Rourke EJ. Fleisher GR. outtpatient treatment of febrile infants 28 to 89 days of age with intramascular administration of ceftriaxons. J Pediatr 1992: 120: 22–7
Preis S. Jugens H. Friedland C, et al. Ceftriaxone alone or in combination with teicoplanin in the management of febrile episodes in neutropenic children and:adolescents with cancer on an outpatient basis.Klin Padiatr 1993: 205: 295–9
Leibovitz E. Tabachnik E. Fliedel O. et al.Once-daily intramuscular ceftriaxone in the: outpa!ient treatment of severe: community-acquired pneumonia in children, Clin Pediatr 1991;29: 634–9
Bradley JS, Ching DK. Phillips SE, Outpalient therapy of serious pediatric infections wilh ceftriaxone. Pediatr Infect Dis J 1988: 7: 160–4
Dagan R. Eihorn M. A program of outpatient parenteral antibiotic therapy for serious pediatric bacterial infections. Rev Infect Dis 1991. 13 Suppl. 2: 152–5
Moskovitz BL. Clinical adverse effects during ceftriaxone therapy. Am J Med 1984: 77: 84–8
Schaad VB, Wedgewood-Krucko J. Tschaeppeler H. Reversible ceftriaxone-associated biliary pseudolithiasis in children.Lancet 1988:2: 1411–3
Oakes M. Macdonald H. Wilson D. Abnormal laboratory test values during ceftriaxone therapy. Am J Med 1984: 77: 89–96
Norrby SR. Pharmacoeconomic studies on antibiotics. Current controversies. Pharmaco Economics 1994: 5: 274–7
Robinson R. Cost and cost-minimisation analysis. BMJ 1993: 307: 726–8
Capri S. Dellamano R. Cost-efTectiveness in the hospital use of antibiotics: introduction, considerations. J Chemother 1993:5: 348–51
Capri S. Carella E. Catena E. et al. Valutazione clinica ed economica della terapia delle infezioni acute delle basse vie respiratorie coo cdalosporine di lera generazione. Farmacie Terapia 1993: 10: 27–35
Hoepelman IM. Rozaberg-Arska M, Verhoef J. Comparison of once daily ceftriaxone with gentamicin plus cefuroxime for treatment of serious bacterial infections. Lancet 1988: 1: 1305–9
Mangi RJ. Peccerillo KM. Ryan I, et al. Cefoperazone versus ceftriaxone monotherapy of nosocomial pneumonia. Diagn Microbiol Infect Dis 1992: 15: 441–7
Poretz DM. Woolard D. Eron LJ, et al. Outpatient use of ceftriaxone: a Cost-benefit analysis. Am J Med 1984: 77: 77–83
Niebuhr H. Nahrstedh U. Ruckert K. et al. Empirical treatment of nosocomial or community-acquired bacterial pneumonia. Chemotherapie 1993: 12: 28–35
Rolston KVI. Jones PG. Fainstein V. et aL Single agent therapy for infection cancer patients: a prospective randomized comparing three extended-spectrum cephalosporins. Eur J Clin Microbiol Infect Dis 1991: 10: 139–45
Schaison GS. Decroly FC Prophylaxis, cost and effectiveness of therapy of infections caused by Gram-positive organism in neutropenic children. J Antimicrob Chemother 1991: 27Suppl. 8: 61–7
Wiliams JA. Flynn PM. Harris S, et al. A randomised study of outpatient treatment with ceftriaxone for selected febrile children wilth sickle cell disease. N Engl J Med 1993; 329: 472–6
Baumgartner J-D. Glauser MP. Single daily dose treatment of severe refractory infections with ceftriaxone. Arch Intern Med 1983: 143: 1868–73
Vichinsky EP. Comprehensive care in sickle cell disease: its impact onai morbidity and mortality. Semin Hematol 1991: 28: 220–6
Francioli PB. Ceftriaxone and outpatient treatment of infectiive endocarditis. Infect Dis Clin North Am 1993: 7: 97–115
Eisenberg JM. Kitz DS. Savings from outpatient antibiotic terapy for osteomyelitis. JAMA 1986; 255: 1584–11
Roche Products (New Zealand) Ltd. Ceftriaxone prescribing information. New Zealand. 1993
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Davis, R., Bryson, H.M. Ceftriaxone. Pharmacoeconomics 6, 249–269 (1994). https://doi.org/10.2165/00019053-199406030-00009
Published:
Issue Date:
DOI: https://doi.org/10.2165/00019053-199406030-00009