
Abstract
An association between hypercholesterolaemia and ischaemic stroke has not yet been clearly defined by observational studies. In clinical trials, however, cholesterol-lowering treatments appear to consistently reduce stroke risk. Data are now available from various primary prevention studies — ALLHAT-LLT (Antihypertensive and Lipid-Lowering treatment to prevent Heart Attack, Lipid-Lowering Therapy), ASCOT-LLA (Anglo-Scandinavian Cardiac Outcomes Trial, Lipid-Lowering Arm), CARDS (Collaborative Atorvastatin Diabetes Study, WOSCOPS (West of Scotland COronary Prevention Study) — and secondary prevention studies — 4S (Scandinavian Simvastatin Survival Study), CARE (Cholesterol and Recurrent Events), GREACE (GREek Atorvastatin and Coronary-heart-disease Evaluation), HPS (Heart Protection Study), LIPID (Long-term Intervention with Pravastatin in Ischaemic Disease), MIRACL (Myocardial Ischemia Reduction with Aggressive Cholesterol Lowering), SPARCL (Stroke Prevention by Aggressive Reduction in Cholesterol Levels), TNT (Treating to New Targets) — confirming the ability of statins to reduce stroke risk.
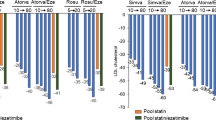
Regarding primary prevention, post hoc analyses showed pravastatin reduced the relative risk of stroke by 9–11 % (not statistically significant) in the ALLHAT-LLT and WOSCOPS trials, whereas atorvastatin reduced this risk by 27–48% in the ASCOT-LLA (p = 0.024) and CARDS trials. It remains to be established in prospective studies whether cholesterol-lowering is effective in the primary prevention of stroke. Regarding secondary prevention, in five placebo-controlled studies (4S, CARE, HPS, LIPID, MIRACL) involving a total of >40 000 patients with coronary heart disease (CHD), statin therapy reduced the relative risk of fatal or nonfatal stroke by 19–50% (p ≤ 0.048); the largest decrease was produced by atorvastatin in the MIRACL study (−50%, p = 0.045). In addition, high-dosage atorvastatin reduced stroke risk by 25% (p = 0.02) relative to lower-dosage therapy in the TNT trial, and by 47% (p = 0.034) relative to ‘usual’ care in the GREACE study. A post hoc analysis of data for 3280 HPS study participants who had had a previous stroke revealed that simvastatin reduced major vascular events by 20% (p = 0.001).
The SPARCL study assessed the secondary preventive efficacy of atorvastatin versus placebo in 4731 patients with a history of stroke or transient ischaemic attack (TLA), but without CHD. Atorvastatin reduced the adjusted relative risk of fatal or nonfatal stroke by 16% (p = 0.03), and that of fatal stroke alone by 43% (p = 0.03). Among secondary study endpoints, atorvastatin reduced the relative risks of stroke and TIA (−23%; p < 0.001), TIA alone (−26%; p = 0.004), and ischaemic stroke (−22%; p = 0.01). Overall, SPARCL study findings suggest that intensive atorvastatin therapy should be started immediately after a stroke or TIA.
In summary, atorvastatin has developed a well defined role in the primary and secondary prevention of cerebrovascular disease, and appears to have a particularly prominent place in preventing such disease in CHD patients, and in the post-stroke and post-TIA setting in patients without CHD.



Similar content being viewed by others


References
Cholesterol, diastolic blood pressure, and stroke: 13,000 strokes in 450,000 people in 45 prospective cohorts. Prospective studies collaboration. Lancet 1995; 346: 1647–53
Bots ML, Elwood PC, Nikitin Y, et al. Total and HDL cholesterol and risk of stroke: EUROSTROKE, a collaborative study among research centres in Europe. J Epidemiol Community Health 2002; 56 Suppl. I: 19–25
Patel A, Woodward M, Campbell DJ, et al. Plasma lipids predict myocardial infarction, but not stroke, in patients with established cerebrovascular disease. Eur Heart J 2005; 26: 1910–5
Sacco RL, Benson RT, Kargman DE, et al. High-density lipoprotein cholesterol and ischemic stroke in the elderly: the Northern Manhattan Stroke Study. JAMA 2001; 285: 2729–35
Tirschwell DL, Smith NL, Heckbert SR, et al. Association of cholesterol with stroke risk varies in stroke subtypes and patient subgroups. Neurology 2004; 63: 1868–75
Di Mascio R, Marchioli R, Tognoni G. Cholesterol reduction and stroke occurrence: an overview of randomized clinical trials. Cerebrovasc Dis 2000; 10: 85–92
Amarenco P, Labrueche J, Lavallée P, et al. Statins in stroke prevention and carotid atherosclerosis: systematic review and up-to-date meta-analysis. Stroke 2004; 35: 2902–9
Corvol JC, Bouzamondo A, Sirol M, et al. Differential effects of lipid-lowering therapies on stroke prevention: a meta-analysis of randomized trials. Arch Intern Med 2003; 163: 669–76
Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005; 366: 1267–78
Shepherd J, Blauw GJ, Murphy MJ, et al. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): a randomised controlled trial. Lancet 2002; 360: 1623–30
Bernick C, Katz R, Smith NL. Statins and cognitive function in the elderly: the Cardiovascular Health Study. Neurology 2005; 65: 1388–94
Etminan M, Gill S, Samii A. The role of lipid-lowering drugs in cognitive function: a meta-analysis of observational studies. Pharmacotherapy 2003; 23: 726–30
Wolozin B, Kellman W, Ruosseau P, et al. Decreased prevalence of Alzheimer disease associated with 3-hydroxyl-3-methylglutaryl coenzyme A resuctase inhibitors. Arch Neurol 2000; 57: 1439–43
ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major outcomes in moderately hypercholesterolemic, hypertensive patients randomized to pravastatin vs usual care: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT-LLT). JAMA 2002; 288: 2998–3007
Colhoun HM, Betteridge DJ, Durrington PN, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet 2004; 364: 685–96
Sever PS, Dahlöf B, Poulter NR, et al. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial, Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet 2003; 361: 1149–58
Shepherd J, Cobbe SM, Ford I, et al. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West of Scotland Coronary Prevention Study Group. N Engl J Med 1995; 333: 1301–7
Athyros VG, Papageorgiou AA, Mercouris BR, et al. Treatment with atorvastatin to the National Cholesterol Educational Program goal versus ‘usual’ care in secondary coronary heart disease prevention: the GREek Atorvastatin and Coronary-heart-disease Evaluation (GREACE) study. Curr Med Res Opin 2002; 18: 215–9
Collins R, Armitage J, Parish S, et al. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20 536 high-risk individuals: a randomised placebo-controlled trial. Lancet 2002; 360: 7–22
LaRosa JC, Grundy SM, Waters DD, et al. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med 2005; 352: 1425–35
Long-term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med 1998; 339: 1349–57
Pedersen TR, Kjekshus J, Berg K, et al. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994; 344: 1383–9
Sacks FM, Pfeffer MA, Moye LA, et al. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. N Engl J Med 1996; 335: 1001–9
Schwartz GG, Olsson AG, Ezekowitz MD, et al. Effects of atorvastatin on early recurrent ischrmic events in acute coronary syndromes: the MIRACL study, a randomized controlled trial. JAMA 2001; 285: 1711–8
Amarenco P, Bogousslavsky J, Callahan A, et al. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med 2006; 355: 549–59
Collins R, Armitage J, Parish S, et al. Effects of cholesterol-lowering with simvastatin on stroke and other major vascular events in 20 536 people with cerebrovascular disease or other high-risk conditions. Lancet 2004; 363: 757–67
Iso H, Jacobs DR, Wentworth D, et al. Serum cholesterol levels and six-year mortality from stroke in 350,977 men screened for the multiple risk factor intervention trial. N Engl J Med 1989; 320: 904–10
Lee SH, Bae HJ, Yoon BW, et al. Low concentration of serum total cholesterol is associated with multifocal signal loss lesions on gradient-echo magnetic resonance imaging: analysis of risk factors for multifocal signal loss lesions. Stroke 2002; 33: 2845–9
Yano K, Reed DM, MacLean CJ. Serum cholesterol and hemorrhagic stroke in the Honolulu Heart Program. Stroke 1989; 20: 1460–5
Waters DD, Schwartz GG, Olsson AG, et al. Effects of atorvastatin on stroke in patients with unstable angina or non-Q-wave myocardial infarction: a Myocardial Ischemia Reduction with Aggressive Cholesterol Lowering (MIRACL) substudy. Circulation 2002; 106: 1690–5
Waters DD, LaRosa JC, Barter P, et al. Effects of high-dose atorvastatin on cerebrovascular events in patients with stable coronary disease in the TNT (treating to new targets) study. J Am Coll Cardiol 2006; 48: 1793–9
Law MR, Wald NJ, Rudnicka AR. Quantifying effect of statins on low density lipoprotein cholesterol, ischaemic heart disease, and stroke: systematic review and meta-analysis. BMJ 2003; 326: 1407–8
Amarenco P. The Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) study. Presentation no. 130 at the World Congress of Cardiology; 2006 Sep 2–6; Barcelona, Spain
Goldstein LB, Amarenco P, Szarek M, et al. Secondary analysis of hemorrhagic stroke in the Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) study [abstract no. 16]. Stroke 2007; 38: 457
Acknowledgements
The preparation of this manuscript has been sponsored by Pfizer Italia, who proposed the initial idea of the review. Dr Achille Gaspardone has the responsibility of reported data as well as of their interpretation. The sponsor had no role in the approval of the final manuscript. Dr Achille Gaspardone served as consultant and/or received speaker honoraria from Pfizer Italia. Prof. Marcello Arca served as consultant and/or received speaker honoraria from Merck Sharp & Dhome, AstraZeneca, Simesa, Sanofi Aventis, Pfizer, Guidotti and Neopharmed. The authors wish to thank Dr Michelangelo Barone from the Medical Department of Pfizer Italia for his technical support in collecting part of the material used for this paper. Editorial support for the preparation of the manuscript was provided by Wolters Kluwer Health Medical Communications.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gaspardone, A., Area, M. Atorvastatin. Drugs 67 (Suppl 1), 55–62 (2007). https://doi.org/10.2165/00003495-200767001-00006
Published:
Issue Date:
DOI: https://doi.org/10.2165/00003495-200767001-00006