
Abstract
Stroke and its consequences are of global concern. Although stroke can affect individuals of any age, it primarily affects the elderly. It is among the leading causes of severe disability and mortality. In recent years, acute stroke has become a medical emergency requiring urgent evaluation and treatment. Effective management of patients with acute stroke starts with organisation of the entire stroke care chain, from the community and prehospital scene, through the emergency department, to a dedicated stroke unit and then to comprehensive rehabilitation.
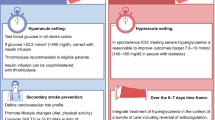
Intravenous thrombolysis with alteplase (recombinant tissue plasminogen activator; rt-PA) 0.9 mg/kg (maximum dose 90mg) was shown to significantly improve outcome of acute ischaemic stroke, despite an increased rate of symptomatic intracerebral haemorrhage, if treatment is initiated within 3 hours after the onset of symptoms to patients who meet strict eligibility criteria. Post-marketing studies have demonstrated that intravenous alteplase can be administered appropriately in a wide variety of hospital settings. However, strict adherence to the published protocol is mandatory, as failure to comply may be associated with an increased risk of symptomatic intracerebral haemorrhage. Intra-arterial revascularisation may provide more complete restitution of flow than intravenous thrombolytic therapy and improve the clinical outcome if it can be undertaken in patients with occlusion of the middle cerebral artery, and possibly the basilar artery, within the first hours from stroke onset. However, further data are needed.
Although intravenous alteplase is recommended for any age beyond 18 years, elderly patients, in particular patients aged ≥80 years, were often excluded or under-represented in randomised clinical trials of thrombolysis, so that available data on risk/benefit ratio for the very elderly are limited. Small post-marketing series suggest that despite elderly patients over 80 years having greater pre-stroke disability, the use of intravenous alteplase in this patient group does not significantly differ in effectiveness and complications compared with the same treatment in patients aged under age 80 years. Further studies are necessary and elderly patients with acute stroke should be included in future trials of the merits of thrombolytic therapy.




Similar content being viewed by others


References
Bonita R. Epidemiology of stroke. Lancet 1992; 339: 342–4
Bamford J, Sandercock P, Dennis M, et al. A prospective study of acute cerebrovascular disease in the community: the Oxfordshire Community Stroke Project 1981–86.
Methodology, demography and incident cases of first-ever stroke. J Neurol Neurosurg Psychiatry 1988; 51: 1373–80
Wolf PA, D’Agostino RB, Belanger AJ, et al. Probability of stroke: a risk profile from the Framingham Study. Stroke 1991; 22: 312–8
Tanne D, Yaari S, Goldbourt U. Risk profile and prediction of long-term ischemic stroke mortality: a 21-year follow-up in the Israeli Ischemic Heart Disease (IIHD) Project. Circulation 1998; 98: 1365–71
Williams GR, Jiang JG, Matchar DB, et al. Incidence and occurrence of total (first-ever and recurrent) stroke. Stroke 1999; 30: 2523–8
Brown RD, Whisnant JP, Sicks JD, et al. Stroke incidence, prevalence, and survival: secular trends in Rochester, Minnesota, through 1989. Stroke 1996; 27: 373–80
Bamford J, Dennis M, Sandercock P, et al. The frequency, causes and timing of death within 30 days of a first stroke: the Oxfordshire Community Stroke Project. J Neurol Neurosurg Psychiatry 1990; 53: 824–9
Al Rajeh S. Stroke in the elderly aged 75 years and above. Cerebrovasc Dis 1994; 4: 402–6
Sharma JC, Fletcher S, Vassallo M. Strokes in the elderly -higher acute and 3-month mortality —an explanation. Cerebrovasc Dis 1999; 9: 2–9
Nakayama H, Jorgensen HS, Raaschou HO, et al. The influence of age on stroke outcome. The Copenhagen Stroke Study. Stroke 1994; 25: 808–13
Pohjasvaara T, Erkinjuntti T, Vataja R, et al. Comparison of stroke features and disability in daily life in patients with ischemic stroke aged 55 to 70 and 71 to 85 years. Stroke 1997; 28: 729–35
Lin HJ, Wolf PA, Kelly-Hayes M, et al. Stroke severity in atrial fibrillation. The Framingham Study. Stroke 1996; 27: 1760–4
Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation: a major contributor to stroke in the elderly. The Framingham Study. Arch Intern Med 1987; 147: 1561–4
Tilley BC, Lyden PD, Brott TG, et al. Total quality improvement method for reduction of delays between emergency department admission and treatment of acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Arch Neurol 1997; 54: 1466–74
Katzan IL, Furlan AJ, Lloyd LE, et al. Use of tissue-type plas-minogen activator for acute ischemic stroke: the Cleveland area experience. JAMA 2000; 283: 1151–8
Kothari R, Sauerbeck L, Jauch E, et al. Patients’ awareness of stroke signs, symptoms, and risk factors. Stroke 1997; 28: 1871–5
Pancioli AM, Broderick J, Kothari R, et al. Public perception of stroke warning signs and knowledge of potential risk factors. JAMA 1998; 279: 1288–92
Kidwell CS, Starkman S, Eckstein M, et al. Identifying stroke in the field. Prospective validation of the Los Angeles prehospital stroke screen (LAPSS). Stroke 2000; 31: 71–6
Kothari RU, Pancioli A, Liu T, et al. Cincinnati Prehospital Stroke Scale: reproducibility and validity. Ann Emerg Med 1999; 33: 373–8
von Kummer R, Allen KL, Holle R, et al. Acute stroke: usefulness of early CT findings before thrombolytic therapy. Radiology 1997; 205: 327–33
Grotta JC, Chiu D, Lu M, et al. Agreement and variability in the interpretation of early CT changes in stroke patients qualifying for intravenous rtPA therapy. Stroke 1999; 30: 1528–33
Wardlaw JM, Dorman PJ, Lewis SC, et al. Can stroke physicians and neuroradiologists identify signs of early cerebral infarction on CT? J Neurol Neurosurg Psychiatry 1999; 67: 651–3
Barber PA, Demchuk AM, Zhang J, et al. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet 2000; 355: 1670–4
Kalra L, Evans A, Perez I, et al. Alternative strategies for stroke care: a prospective randomised controlled trial. Lancet 2000; 356: 894–9
Kaste M, Skyhoj Olsen T, Orgogozo J, et al. Organization of stroke care: education, stroke units and rehabilitation. European Stroke Initiative (EUSI). Cerebrovasc Dis 2000; 10 Suppl. 3: 1–11
Organised inpatient (stroke unit) care for stroke. Stroke Unit Trialists’ Collaboration. Cochrane Database Syst Rev 2000: CD000197
Kaste M, Palomaki H, Sarna S. Where and how should elderly stroke patients be treated? A randomized trial. Stroke 1995; 26: 249–53
Fagerberg B, Claesson L, Gosman-Hedstrom G, et al. Effect of acute stroke unit care integrated with care continuum versus conventional treatment: a randomized 1-year study of elderly patients: the Goteborg 70+ stroke study. Stroke 2000; 31: 2578–84
Hankey GJ, Warlow CP. Treatment and secondary prevention of stroke: evidence, costs, and effects on individuals and populations. Lancet 1999; 354: 1457–63
Alberts MJ, Hademenos G, Latchaw RE, et al. Recommendations for the establishment of primary stroke centers. Brain Attack Coalition. JAMA 2000; 283: 3102–9
Fieschi C, Argentino C, Lenzi GL, et al. Clinical and instrumental evaluation of patients with ischemic stroke within the first six hours. J Neurol Sci 1989; 91: 311–21
del Zoppo GJ, Poeck K, Pessin MS, et al. Recombinant tissue plasminogen activator in acute thrombotic and embolic stroke. Ann Neurol 1992; 32: 78–86
Astrup J, Siesjo BK, Symon L. Thresholds in cerebral ischemia —the ischemic penumbra. Stroke 1981; 12: 723–5
Zivin JA, Fisher M, DeGirolami U, et al. Tissue plasminogen activator reduces neurological damage after cerebral embolism. Science 1985; 230: 1289–92
Overgaard K, Sereghy T, Boysen G, et al. Reduction of infarct volume and mortality by thrombolysis in a rat embolie stroke model. Stroke 1992; 23: 1167–73
Chopp M, Zhang RL, Zhang ZG, et al. The clot thickens-thrombolysis and combination therapies. Acta Neurochir 1999; 73: 67–71
Randomised controlled trial of streptokinase, aspirin, and combination in treatment of acute ischaemic stroke. Multicentre Acute Stroke Trial-Italy (MAST-I) Group. Lancet 1995; 346: 1509–14
Thrombolytic therapy with streptokinase in acute ischemic stroke. The Multicenter Acute Stroke Trial —Europe Study Group. N Engl J Med 1996; 335: 145–50
Donnan GA, Davis SM, Chambers BR, et al. Streptokinase for acute ischemic stroke with relationship to time of administration: Australian Streptokinase (ASK) Trial Study Group. JAMA 1996; 276: 961–6
Hacke W, Kaste M, Fieschi C, et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The European Cooperative Acute Stroke Study (ECASS). JAMA 1995; 274: 1017–25
Hacke W, Kaste M, Fieschi C, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet 1998; 352: 1245–51
The NINDS rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995; 333: 1581–7
Clark WM, Wissman S, Albers GW, et al. Recombinant tissue-type plasminogen activator (alteplase) for ischemic stroke 3 to 5 hours after symptom onset. The ATLANTIS Study: a randomized controlled trial. Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic Stroke. JAMA 1999; 282: 2019–26
Furlan A, Higashida R, Wechsler L, et al. Intra-arterial prourokinase for acute ischemic stroke. The PROACT II study: a randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism. JAMA 1999; 282: 2003–11
Tanne D, Bates VE, Verro P, et al. Initial clinical experience with IV tissue plasminogen activator for acute ischemic stroke: a multicenter survey. The t-PA Stroke Survey Group. Neurology 1999; 53: 424–7
Hanson SK, Brauer DJ, Brown RD, et al. Should use of t-PA for ischemic stroke be restricted to specialized stroke centers [abstract]. Stroke 2000; 31: 313
Grond M, Stenzel C, Schmulling S, et al. Early intravenous thrombolysis for acute ischemic stroke in a community-based approach. Stroke 1998; 29: 1544–9
Grotta JC, Alexandrov AV, Burgin WS, et al. Intravenous TPA for ischemic stroke patients: Houston experience 1996–2000. Stroke 2001; 32: 323-b
Albers GW, Bates VE, Clark WM, et al. Intravenous tissue-type plasminogen activator for treatment of acute stroke: the Standard Treatment with Alteplase to Reverse Stroke (STARS) study. JAMA 2000; 283: 1145–50
Hill MD, Woolfendeu A, Teal PA, et al. Intravenous Alteplase for stroke: the Canadian experience. Stroke Intervention 2000; 2: 3–8
Cornu C, Boutitie F, Candelise L, et al. Streptokinase in acute ischemic stroke: an individual patient data meta-analysis: the Thrombolysis in Acute Stroke Pooling Project. Stroke 2000; 31: 1555–60
Brott T, Bogousslavsky J. Treatment of acute ischemic stroke. N Engl J Med 2000; 343: 710–22
Albers GW, Amarenco P, Easton JD, et al. Antithrombotic and thrombolytic therapy for ischemic stroke. Chest 2001; 119: 300S–20S
Kwiatkowski TG, Libman RB, Frankel M, et al. Effects of tissue plasminogen activator for acute ischemic stroke at one year. National Institute of Neurological Disorders and Stroke Recombinant Tissue Plasminogen Activator Stroke Study Group. N Engl J Med 1999; 340: 1781–7
Marier JR, Tilley BC, Lu M, et al. Early stroke treatment associated with better outcome: the NINDS rt-PA stroke study. Neurology 2000; 55: 1649–55
The NINDS rt-PA Stroke Study Group. Generalized efficacy of t-PA for acute stroke. Subgroup analysis of the NINDS t-PA Stroke Trial. Stroke 1997; 28: 2119–25
A systems approach to immediate evaluation and management of hyperacute stroke. Experience at eight centers and implications for community practice and patient care. The National Institute of Neurological Disorders and Stroke (NINDS) rt-PA Stroke Study Group. Stroke 1997; 28: 1530–40
Practice advisory: thrombolytic therapy for acute ischemic stroke-summary statement. Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 1996; 47: 835–9
Adams HPJ, Brott TG, Furlan AJ, et al. Guidelines for thrombolytic therapy for acute stroke: a supplement to the guidelines for the management of patients with acute ischemic stroke. A statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Stroke 1996; 27: 1711–8
European Stroke Initiative recommendations for stroke management. European Stroke Council, European Neurological Society and European Federation of Neurological Societies. Cerebrovasc Dis 2000; 10: 335–51
Fagan SC, Morgenstern LB, Petitta A, et al. Cost-effectiveness of tissue plasminogen activator for acute ischemic stroke. NINDS rt-PA Stroke Study Group. Neurology 1998; 50: 883–90
Hacke W, Brott T, Caplan L, et al. Thrombolysis in acute ischemic stroke: controlled trials and clinical experience. Neurology 1999; 53: S3–14
Schmulling S, Grond M, Rudolf J, et al. One-year follow-up in acute stroke patients treated with rtPA in clinical routine. Stroke 2000; 31: 1552–4
Buchan AM, Barber PA, Newcommon N, et al. Effectiveness of t-PA in acute ischemic stroke: outcome relates to appropriateness. Neurology 2000; 54: 679–84
Lopez-Yunez AM, Bruno A, Williams LS, et al. Protocol violations in community-based rTPA stroke treatment are associated with symptomatic intracerebral hemorrhage. Stroke 2001; 32: 12–6
Demchuk AM, Morgenstern LB, Krieger DW, et al. Serum glucose level and diabetes predict tissue plasminogen activator-related intracerebral hemorrhage in acute ischemic stroke. Stroke 1999; 30: 34–9
Tanne D, Kasner SE, Demchuk AM, et al. Prediction of intracerebral hemorrhage after intravenous rt-PA therapy for acute ischemic stroke in clinical practice: the multicenter acute stroke survey. Neurology. In press
Kasner SE, Villar-Cordova CE, Tong D, et al. Hemopericardium and cardiac tamponade after thrombolysis for acute ischemic stroke. Neurology 1998; 50: 1857–9
Hill MD, Barber PA, Takahashi J, et al. Anaphylactoid reactions and angioedema during alteplase treatment of acute ischemic stroke. CMAJ 2000; 162: 1281–4
Rudolf J, Grond M, Schmulling S, et al. Orolingual angioneurotic edema following therapy of acute ischemic stroke with alteplase. Neurology 2000; 55: 599–600
Rudolf J, Grond M, Prince WS, et al. Evidence of anaphylaxy after alteplase infusion. Stroke 1999; 30: 1142–3
Abou-Chebl A, Furlan AJ. Intra-arterial thrombolysis in acute stroke. Curr Opin Neurol 2000; 13: 51–5
Lewandowski CA, Frankel M, Tomsick TA, et al. Combined intravenous and intra-arterial r-TPA versus intra-arterial therapy of acute ischemic stroke. Emergency Management of Stroke (EMS) bridging trial. Stroke 1999; 30: 2598–605
The NINDS rt-PA Stroke Study Group. Intracerebral hemorrhage after intravenous t-PA therapy for ischemic stroke. The NINDS t-PA Stroke Study Group. Stroke 1997; 28: 2109–18
Larrue V, von Kummer R, del Zoppo G, et al. Hemorrhagic transformation in acute ischemic stroke. Potential contributing factors in the European Cooperative Acute Stroke Study. Stroke 1997; 28: 957–60
Larrue V, von Kummer R, Muller A, et al. Risk factors for severe hemorrhagic transformation in ischemic stroke patients treated with recombinant tissue plasminogen activator: a secondary analysis of the European-Australasian Acute Stroke Study (ECASS II). Stroke 2001; 32: 438–41
Tanne D, Gorman MJ, Bates VE, et al. Intravenous tissue plasminogen activator for acute ischemic stroke in patients aged 80 years and older: the tPA stroke survey experience. Stroke 2000; 31: 370–5
Demaerschalk B, Merino JG, Silver B, et al. Intravenous tissue plasminogen activator for acute ischemic stroke in patients 80 years old: the London, Canada experience [abstract]. Stroke 2001;32: 358–d
Yamada M. Cerebral amyloid angiopathy: an overview. Neuropathology 2000; 20: 8–22
Greenberg SM, Vonsattel JP Diagnosis of cerebral amyloid angiopathy. Sensitivity and specificity of cortical biopsy. Stroke 1997; 28: 1418–22
Sloan MA, Price TR, Petito CK, et al. Clinical features and pathogenesis of intracerebral hemorrhage after rt-PA and heparin therapy for acute myocardial infarction: the Thrombolysis in Myocardial Infarction (TIMI) II Pilot and Randomized Clinical Trial combined experience. Neurology 1995; 45: 649–58
Henon H, Godefroy O, Lucas C, et al. Risk factors and leukoaraiosis in stroke patients. Acta Neurol Scand 1996; 94: 137–44
Wardlaw JM, del Zoppo G, Yamaguchi T. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev 2000: CD000213
Leys D, Englund E, Del Ser T, et al. White matter changes in stroke patients. Relationship with stroke subtype and outcome. Eur Neurol 1999; 42: 67–75
Gorter JW. Major bleeding during anticoagulation after cerebral ischemia: patterns and risk factors. Stroke Prevention in Reversible Ischemia Trial (SPIRIT). European Atrial Fibrillation Trial (EAFT) study groups. Neurology 1999; 53: 1319–27
de Boer A, Kluft C, Kroon JM, et al. Liver blood flow as a major determinant of the clearance of recombinant human tissue-type plasminogen activator. Thromb Haemost 1992; 67: 83–7
Cohen AF, Burggraaf K, de Boer A, et al. Clearance of plasminogen activator —a major determinant of plasma concentration: therapeutic and diagnostic implications. Ann NY Acad Sci 1992; 667: 443–9
Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomized trials of more than 1000 patients. Fibrinolytic Therapy Trialists’ (FTT) Collaborative Group. Lancet 1994; 343: 311–22
Ramanathan K, Ellis CJ, White HD. Thrombolytic therapy in the elderly. Pharmacoeconomic considerations. Drugs Aging 1996; 8: 237–44
Woods KL, Ketley D. Utilisation of thrombolytic therapy in older patients with myocardial infarction. Drugs Aging 1998; 13: 435–41
Thiemann DR, Coresh J, Schulman SP, et al. Lack of benefit for intravenous thrombolysis in patients with myocardial infarction who are older than 75 years. Circulation 2000; 101: 2239–46
Brass LM, Lichtman JH, Wang Y, et al. Intracranial hemorrhage associated with thrombolytic therapy for elderly patients with acute myocardial infarction: results from the Cooperative Cardiovascular Project. Stroke 2000; 31: 1802–11
Gurwitz JH, Gore JM, Goldberg RJ, et al. Risk for intracranial hemorrhage after tissue plasminogen activator treatment for acute myocardial infarction. Participants in the National Registry of Myocardial Infarction 2. Ann Intern Med 1998; 129: 597–604
Simoons ML, Maggioni AP, Knatternd G, et al. Individual risk assessment for intracranial haemorrhage during thrombolytic therapy. Lancet 1993; 342: 1523–8
Berger AK, Schulman KA, Gersh BJ, et al. Primary coronary angioplasty vs thrombolysis for the management of acute myocardial infarction in elderly patients. JAMA 1999; 282: 341–8
Ayanian JZ, Braunwald E. Thrombolytic therapy for patients with myocardial infarction who are older than 75 years. Do the risks outweigh the benefits? Circulation 2000; 101: 2224–6
McMechan SR, Adgey AA. Age related outcome in acute myocardial infarction. Elderly people benefit from thrombolysis and should be included in trials. BMJ 1998; 317: 1334–5
Acknowledgements
The authors greatly thank Dr Steven R. Levine from Wayne State University/Detroit Medical Center Stroke Center, Detroit, MI, USA for his insightful comments and revision of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tanne, D., Turgeman, D. & Adler, Y. Management of Acute Ischaemic Stroke in the Elderly. Drugs 61, 1439–1453 (2001). https://doi.org/10.2165/00003495-200161100-00007
Published:
Issue Date:
DOI: https://doi.org/10.2165/00003495-200161100-00007