
Summary
Synopsis
Omeprazole, a gastric acid pump inhibitor, dose-dependently controls gastric acid secretion; the drug has greater antisecretory activity than histamine H2-receptor antagonists.
Omeprazole 20 to 40 mg/day is more effective than histamine H2-receptor antagonists in the short term treatment of duodenal ulcer, gastric ulcer and reflux oesophagitis. Available data suggest that omeprazole 10 to 40 mg/day is also more effective than ranitidine in the maintenance therapy of duodenal ulcer and reflux oesophagitis. The drug is also effective in patients with duodenal ulcer, gastric ulcer or reflux oesophagitis poorly responsive to histamine H2-receptor antagonists.
The efficacy of omeprazole 20 mg/day appears to be similar to that of lansoprazole 30 mg/day in the short term treatment of duodenal ulcer, gastric ulcer and reflux oesophagitis. However, most available studies have been reported in abstract form only, and 2 of 3 studies in patients with duodenal ulcer have shown greater healing rates at 2 (but not 4) weeks with lansoprazole.
Helicobacter pylori eradication decreases duodenal ulcer relapse rates and appears to be associated with improved duodenal ulcer healing rates. Evidence also suggests that H. pylori eradication is associated with reduced gastric ulcer relapse rates. Omeprazole monotherapy may suppress but does not eradicate H. pylori infection. Eradication rates with omeprazole 20 or 40mg twice daily plus amoxicillin usually up to 2 g/day (3 g/day in a few studies) for 2 weeks appear to be similar to those of standard triple therapy (bismuth salt plus metronidazole, plus tetracycline or amoxicillin) or omeprazole plus clarithromycin, although eradication rates vary widely. Omeprazole plus amoxicillin appears to be better tolerated than triple therapy and represents a first-line treatment alternative in patients with H. pylori-associated peptic ulcer disease. Omeprazole plus amoxicillin plus metronidazole appears to be more effective than omeprazole plus amoxicillin in patients with metronidazole-sensitive H. pylori infection.
Omeprazole remains a treatment of choice in patients with Zollinger-Ellison syndrome. The dosage should be adjusted according to individual response. However, relatively low dosages of 10 to 40 mg/day may be sufficient in some patients. The drug has also shown promise in the treatment of children with severe reflux oesophagitis, in patients with reflux oesophagitis and coexisting systemic sclerosis, and in the prevention of aspiration pneumonia. Evidence suggests that omeprazole is more effective than ranitidine in patients with nonsteroidal anti-inflammatory drug (NSAID)-induced gastric damage who continue to take NSAIDs, especially in patients with large gastric ulcers; however, completion of ongoing studies is required to verify this.
Omeprazole is generally well tolerated during short (<12 weeks) and long (up to 10 years or more) term treatment. The most common, albeit infrequent, adverse effects are gastrointestinal in nature and are similar to those with histamine H2-receptor antagonists.
Thus, omeprazole is a first-line agent in the short and long term treatment of reflux oesophagitis, Zollinger-Ellison syndrome, and the short and long term treatment of peptic ulcer disease. Omeprazole plus amoxicillin appears to be of similar efficacy to, and better tolerated than, bismuth-containing triple therapy in eradicating H. pylori infection. Simultaneous ulcer healing, symptom resolution and H. pylori eradication is likely to become the management strategy of choice in H. pylori-positive duodenal ulcer disease, with omeprazole poised to play a substantial role in such therapy.
Pharmacological Properties
Omeprazole inhibits H+, K+-ATPase (the gastric acid pump), dose-dependently suppressing basal and stimulated gastric acid secretion. The drug has a prolonged duration of action and is more effective than histamine H2-receptor antagonists in suppressing gastric acid secretion. The short term acid-suppressing effects of omeprazole are maintained in the long term (6 to 12 months).
Acid inhibition following omeprazole therapy results in moderate increases in plasma gastrin levels in most patients which are greater than those with histamine H2-receptor antagonists and, in animals, are similar to those with lansoprazole.
The pharmacokinetic profile of omeprazole is well established. Since the last review of omeprazole in Drugs the pharmacokinetic parameters of omeprazole in patients with Zollinger-Ellison syndrome have been shown to be similar to those in healthy volunteers and patients with peptic ulcer disease except for elimination half-life which is increased approximately 2-fold. The metabolism of omeprazole to its hydroxy derivative is reduced in patients who are poor hydroxylators of S-mephenytoin.
Dosage adjustments do not appear to be necessary in patients with renal impairment or in the elderly amd are not considered to be necessary in patients with hepatic impairment, despite a reduction in the hepatic clearance of omeprazole. Pharmacokinetic data in children remain scarce.
Effects on Helicobacter pylori
Most cases of peptic ulcer disease are causally associated with Helicobacter pylori gastritis, but the exact pathogenetic mechanism of H. pylori-induced gastroduodenal damage is unknown. Omeprazole monotherapy may suppress but does not eradicate H. pylori. Although eradication rates vary between studies, omeprazole plus amoxicillin appears to eradicate H. pylori in a similar number of patients as standard triple therapy (bismuth salt plus metronidazole plus amoxicillin) or omeprazole plus clarithromycin. Omeprazole 20mg twice daily plus amoxicillin up to 2 g/day for 2 weeks is the currently recommended regimen of these agents, although preliminary evidence suggests that higher dosages of amoxicillin (up to 3 g/day) in combination with omeprazole 20mg twice daily for 2 weeks may be more effective. Evidence suggests that omeprazole plus amoxicillin plus metronidazole is more effective than omeprazole plus amoxicillin in patients with metronidazole-sensitive H. pylori. However, the search for the optimal treatment regimen for the eradication of H. pylori continues.
Therapeutic Use
Data published since the last review of omeprazole in Drugs confirm the significantly superior efficacy of 2 to 4 weeks’ treatment with omeprazole 20 mg/day, in terms of both healing rates and symptom resolution, compared with ranitidine 300 mg/day, cimetidine 800 mg/day or famotidine 40 mg/day in the short term treatment of duodenal ulcer. A meta-analysis of nearly 45 000 patients with duodenal ulcer found that healing rates with omeprazole were significantly greater than those with histamine H2-receptor antagonists, prostaglandin analogues, site-protective agents or placebo. Recent data also confirm that omeprazole is more effective than high dose ranitidine in patients with duodenal ulcers poorly responsive to standard dosages of histamine H2-receptor antagonists, and confirm the superior efficacy of omeprazole 10 to 20 mg/day in the maintenance treatment of duodenal ulcer.
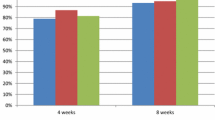
Duodenal ulcer healing rates at 4 weeks appear to be similar with omeprazole 20 mg/day or lansoprazole 30 mg/day. However, healing rates at 2 weeks were greater with lansoprazole in 2 of the 3 published studies.
H. pylori eradication is associated with decreased relapse rates of duodenal and gastric ulcer. Eradication of H. pylori also appears to be associated with higher duodenal ulcer healing rates than persistent H. pylori infection, although further study is needed to confirm this.
Recent data confirm that omeprazole 20 mg/day is more effective than ranitidine 300 mg/day or cimetidine 800 mg/day, and is similar to that of lansoprazole 30 mg/day, in the short term treatment of gastric ulcer. The efficacy of omeprazole appears to be superior to that of ranitidine in patients with nonsteroidal anti-inflammatory drug (NSAID)-induced gastric damage who continue to take NSAIDs, especially in patients with large (>2cm in diameter) ulcers.
The superior efficacy of omeprazole 20 or 40 mg/day in terms of healing and symptom resolution compared with ranitidine 150mg twice daily in the short term treatment of all grades of reflux oesophagitis, including histamine H2-receptor antagonist-refractory disease, has also been confirmed in recent studies. Available data suggest that the efficacy of omeprazole is superior to that of ranitidine in combination with cisapride or metoclopramide, and similar to that of lansoprazole in the short term treatment of reflux oesophagitis. Recent data confirm the superiority of omeprazole over ranitidine in the prevention of recurrence of reflux oesophagitis. Further study with a low omeprazole dosage of 10 mg/day in the prevention of reflux oesophagitis recurrence is underway. Omeprazole has also shown promise in the treatment of patients with reflux oesophagitis and coexisting systemic sclerosis or peptic oesophageal strictures, and in children with severe gastro-oesophageal reflux. Although omeprazole has been shown to improve oesophagitis in patients with Barrett’s oesophagus, data on regression of the metaplasia are inconclusive.
The efficacy of omeprazole in the treatment of patients with Zollinger-Ellison syndrome is well established. Relatively low omeprazole dosages of 10 to 40 mg/day may be sufficient in some patients although dosage titration is advised.
Oral omeprazole 40mg on the evening before surgery plus oral omeprazole 40mg on the morning before surgery, or intravenous omeprazole 40mg 1 hour before induction of anaesthesia reduces the risk of aspiration pneumonitis during general anaesthesia.
Tolerability
The favourable tolerability profile of short term (<12 weeks) omeprazole therapy is well established, and is similar to that of short term ranitidine or cimetidine therapy. The most commonly reported adverse effects with short term omeprazole therapy are diarrhoea (1 to 3% of patients), headache (0.5 to 2.4%), nausea (0.9 to 2%), abdominal pain (0.4 to 2%), flatulence (1.5%) and dizziness/vertigo (0.5 to 1%). These adverse effects are generally mild, self-limiting and unrelated to dosage.
The adverse event profile of long term omeprazole therapy is similar to that seen in the short term; however, there is a trend towards a lower incidence of diarrhoea and headache. There have been no reports of serious adverse effects with long term omeprazole therapy. Mucosal cell hyperplasia and atrophic gastritis may occur in some patients receiving long term omeprazole therapy.
Omeprazole plus amoxicillin and omeprazole plus amoxicillin plus metronidazole appear to be better tolerated and associated with greater compliance than conventional bismuth-based triple therapy in patients with H. pylori infection.
Dosage and Administration
The recommended dosage of omeprazole in patients with reflux oesophagitis, or duodenal or gastric ulcer is 20 mg/day for 2 to 8 weeks. A dosage of 40 mg/day may be required in patients with conditions poorly responsive to histamine H2-receptor antagonists or in patients unhealed after 8 weeks’ omeprazole 20 mg/day therapy.
An omeprazole dosage of 10 to 20 mg/day has been shown to prevent recurrence of duodenal ulcer, and omeprazole 10 to 40 mg/day is also effective in the prevention of reflux oesophagitis relapse. Omeprazole 20mg twice daily plus amoxicillin up to 2 g/day is the currently recommended dosage regimen of these agents for the eradication of H. pylori infection.
The recommended dosage of omeprazole in patients with Zollinger-Ellison syndrome is 60 mg/day, although lower dosages (10 to 40 mg/day) are effective in some patients. Oral omeprazole 40mg in the evening before surgery plus oral omeprazole 40mg on the morning of surgery, or intravenous omeprazole 40mg 1 hour before induction of anaesthesia have shown promise in the prevention of aspiration pneumonia during general anaesthesia.
Dosage reductions are not necessary in patients with hepatic or renal impairment, or in the elderly.
Similar content being viewed by others


References
McTavish D, Buckley MM-T, Heel RC. Omeprazole. An updated review of its pharmacology and therapeutic use in acid-related disorders. Drugs 1991; 42: 138–70
Clissold SP, Campoli-Richards DM. Omeprazole: a preliminary review of its pharmacodynamic and pharmacokinetic properties, and therapeutic potential in peptic ulcer disease and Zollinger-Ellison syndrome. Drugs 1986; 32: 15–47
Sachs G, Shin JM, Besancon M, et al. The continuing development of gastric acid pump inhibitors. Aliment Pharmacol Ther 1993; 7 Suppl. 1: 4012
Simon A, Besancon M, Shin JM, et al. The H, H ATPase sites that react selectively with the benzimidazole class of anti-ulcer drugs [abstract]. Gastroenterology 1993; 104: A192
Burget DW, Chiverton SG, Hunt RH. Is there an optimal degree of acid suppression for healing of duodenal ulcers? A model of the relationship between ulcer healing and acid suppression. Gastroenterology 1990; 99: 345–51
Marks IN, Young GO, Winter T, et al. Duration of acid inhibition after withdrawal of omeprazole treatment in DU patients in remission [abstract]. Gastroenterology 1993; 104: A140
Lind T, Cederberg C, Olausson M, et al. Omeprazole in elderly duodenal ulcer patients: relationship between reduction in gastric acid secretion and fasting plasma gastrin. Eur J Clin Pharmacol 1991; 40: 557–60
Lazzaroni M, Sangaletti O, Bianchi Porro G. Gastric acid secretion and plasma gastrin during short-term treatment with omeprazole and ranitidine in duodenal ulcer patients. Hepatogastroenterology 1992; 39: 366–70
Walker S, Klotz U, Sarem-Aslani A, et al. Effect of omeprazole on nocturnal intragastric pH in cirrhotics with inadequate antisecretory response to ranitidine. Digestion 1991; 48: 179–84
Savarino V, Mela GS, Zentilin P, et al. Antisecretory effect of three premeal doses of cimetidine 400 mg versus a single morning dose of omeprazole 20 mg: pathophysiological implications for duodenal ulcer treatment. Am J Gastroenterol 1993; 88: 1088–92
Corinaldesi R, De Giorgio R, Stanghellini V, et al. Comparison of the antisecretory effects of omeprazole and famotidine on peptone-meal-stimulated gastric acid secretion in patients with duodenal ulcer. Curr Ther Res 1991; 49: 560–5
Verdu EF, Armstrong D, Fraser R, et al. Interaction between Helicobacter pylori infection and acid inhibition by omeprazole. Hepatogastroenterology 1994; 41: 94
Cederberg C, Lind T, Rohss K, et al. Comparison of once-daily intravenous and oral omeprazole on pentagastrin-stimulated acid secretion in duodenal ulcer patients. Digestion 1992; 53: 171–8
Cederberg C, Rohss K, Lundborg P, et al. Effect of once daily intravenous and oral omeprazole on 24-hour intragastric acidity in healthy subjects. Scand J Gastroenterol 1993; 28: 179–84
Cederberg C, Thomson ABR, Mahachai V, et al. Effect of intravenous and oral omeprazole on 24-hour intragastric acidity in duodenal ulcer patients. Gastroenterology 1992; 103: 913–8
Cederberg C, Thompson ABR, Kirdeikis P, et al. Effect of continuous intravenous infusion of omeprazole on 24-hour intragastric pH in fasting DU-patients: comparison to repeated bolus doses of omeprazole or ranitidine [abstract]. Gastroenterology 1992; 102: A48
Sackier JM, Halliday K, Sprott P, et al. The effects of intravenous omeprazole on 24h gastric secretion in healthy subjects. Comparisons of continuous and intermittent infusions: a pilot study. Eur J Gastroenterol 1991; 3: 679–84
Chiverton SG, Howden CW, Burget DW, et al. Omeprazole (20 mg) daily given in the morning or evening: a comparison of effects on gastric acidity, and plasma gastrin omeprazole concentration. Aliment Pharmacol Ther 1992; 6: 103–11
Vigneri S, Savarino V, Mela GS, et al. The effects of omeprazole long-term treatment for duodenal ulcer on circadian gastric acidity [abstract]. Ital J Gastroenterol 1991; 23 Suppl. 2: 551
Banerjee S, Ardill JES, Beattie AD, et al. Omeprazole does not alter plasma gastrin in patients with achlorhydria [abstract F224]. Gut 1993; 34: S57
Holt S. Proton-pump inhibition for acid-related disease. South MedJ 1991; 84: 1078–87
Lysy J, Karmeli F, Wengrower D, et al. Effect of duodenal ulcer healing induced by omeprazole and ranitidine on the generation of gastroduodenal eicosanoids, platelet-activating factor, pepsinogen A, and gastrin in duodenal ulcer patients. Scand J Gastroenterol 1992; 27: 13–9
Pedersen SA, Rasmussen L, Øster-Jørgensen E, et al. A double-blind placebo-controlled study on the effects of omeprazole on fasting and early postprandial levels of gastrin and secretin [abstract 148]. Eur J Gastroenterol Hepatol 1991; 3 Suppl. 1: S37
Rasmussen L, Øster-Jørgensen E, Qvist N, et al. The effects of omeprazole on interdigestive motility and early postprandial levels of gastrin and secretin. Scand J Gastroenterol 1992; 27: 119–23
Thompson C, Sandier R, Isaacs K, et al. Comparison of the effects of omeprazole, cimetidine and ranitidine on hypergas-trinaemia in humans and rats [abstract]. Gastroenterology 1992; 102:A178
Lee H, Håkanson R, Karlsson A, et al. Lansoprazole and omeprazole have similar effects on plasma gastrin levels, enterochromaffin-like cells, gastric cells and somatostatin cells in the rat stomach. Digestion 1992; 51: 125–32
Baak LC, Biemond I, Jansen JBMJ, et al. Repeated intravenous bolus injections of omeprazole: effects on 24-hour intragastric pH, serum gastrin, and serum pepsinogen A and C. Scand J Gastroenterol 1991; 26: 737–46
Baak LC, Jansen JBMJ, Biemond I, et al. Weekend treatment with 20 and 40 mg omeprazole: effect on intragastric pH, fasting and postprandial serum gastrin, and serum pepsinogens. Gut 1991; 32: 977–82
Biemond I, Klinkenberg-Knol EC, Lamers CBHW, et al. Serum pepsinogens after interruption of long-term maintenance therapy with omeprazole in patients with reflux esophagitis. Dig Dis Sci 1993; 38: 932–6
De Boni M, De Bona M, Bellumat A, et al. Omeprazole and duodenal ulcer healing: effect on gastrin and pepsinogen A and C basal serum levels [abstract]. Gut 1993; 34: S13
Nemeth J, Varro A, Bridson J, et al. Increased tissue concentrations of the gastrin precursor in patients treated with omeprazole. Eur J Clin Invest 1992; 22: 638–44
Varro A, Nemeth J, Bridson J, et al. Antral progastrin concentrations after omeprazole. Gut 1991; 32: A594–5
Rogers M, Primrose JN, Carroll N, et al. Omeprazole but not cimetidine markedly inhibits pepsin secretion in patients with refractory duodenal ulcer [abstract]. Gut 1990; 31: A1200
Bigard MA, Isal JP. Complete prevention by omeprazole of aspirin-induced gastric lesions in healthy subjects. Gut 1988; 29:A712
Daneshmend TK, Stein AG, Bhaskar NK, et al. Abolition by omeprazole of aspirin-induced gastric mucosal injury in man. Gut 1990; 31: 514–7
Scheiman JM, Behler EM, Loeffler KM, et al. Prophylaxis of aspirin induced gastroduodenal injury by omeprazole [abstract]. Gastroenterology 1992; 102: A160
Oddsson E, Gudjónsson H, Thjódleifsson B. Comparison between ranitidine and omeprazole for protection against gastroduodenal damage caused by naproxen. Scand J Gastroenterol 1992; 27: 1045–8
Lamers CBHW, Teunissen L, Jansen JBMJ. Absorption of omeprazole in Zollinger-Ellison syndrome is accelerated by alkali [abstract]. Gut 1985; 26: A1134–5
Andersson T, Cederberg C, Regårdh CG, et al. Pharmacokinetics of various single intravenous and oral doses of omeprazole. Eur J Clin Pharmacol 1990; 39: 195–7
Andersson T, Andren K, Cederberg C, et al. Pharmacokinetics and bioavailability of omeprazole after single and repeated oral administration in healthy subjects. Br J Clin Pharmacol 1990; 29: 557–63
Andersson T, Cederberg C, Heggelund A, et al. The pharmacokinetics of single and repeated once-daily doses of 10, 20 and 40mg omeprazole as enteric-coated granules. Drug Invest 1991; 3: 45–52
Andersson T, Bergstrand R, Cederberg C. Influence of acid secretory status on absorption of omeprazole from enteric coated granules. Br J Clin Pharmacol 1991; 31: 275–8
Andersson T, Regårdh C-G. Pharmacokinetics of omeprazole and metabolites following single intravenous and oral doses of 40 and 80mg. Drug Invest 1990; 2: 255–63
Vinayek R, Amantea MA, Maton PN, et al. Pharmacokinetics of oral and intravenous omeprazole in patients with the Zollinger-Ellison syndrome. Gastroenterology 1991; 101: 138–47
Andersson T, Regårdh C-G, Dahl-Puustinen M-L, et al. Slow omeprazole metabolisers are also poor S-mephenytoin hydroxylators [correspondence]. Ther Drug Monit 1990; 12: 415–6
Chiba K, Kobayashi K, Manabe K, et al. Oxidative metabolism of omeprazole in human liver microsomes: cosegregation with S-mephenytoin 4′-hydroxylation. J Pharmacol Exp Ther 1993; 266: 52–9
Andersson T, Cederberg C, Edvardsson G, et al. Effect of omeprazole treatment on diazepam plasma levels in slow versus normal rapid metabolisers of omeprazole. Clin Pharmacol Ther 1990; 47: 79–85
Sohn D-R, Kobayashi K, Chiba K, et al. Disposition kinetics and metabolism of omeprazole in extensive and poor metabolizers of S-mephenytoin 4′-hydroxylation recruited from an Oriental population. J Pharmacol Exp Ther 1992; 262: 1195–202
Burgess E, Muruve D. Renal effects of peptic ulcer therapy. Drug Saf 1992; 7: 282–91
Landahl S, Andersson T, Larsson M, et al. Pharmacokinetic study of omeprazole in elderly healthy volunteers. Clin Pharmacokinet 1992; 23: 469–76
Andersson T, Olsson R, Regårdh C-G, et al. Pharmacokinetics of [14C]omeprazole in patients with liver cirrhosis. Clin Pharmacokinet 1993; 24: 71–8
Kato S, Shibuya H, Hayashi Y, et al. Effectiveness and pharmacokinetics of omeprazole in children with refractory duodenal ulcer. J Pediatr Gastroenterol Nutr 1992; 15: 184–8
Sipponen P, Hyvarinen H. Role of Helicobacter pylori in the pathogenesis of gastritis, peptic ulcer and gastric cancer. Scand J Gastroenterol 1993; 28 Suppl. 196: 3–6
Vigneri S, Termini R, Di Mario F, et al. Effects of short-term omeprazole therapy for duodenal ulcer on Helicobacter pylori and related gastritis [abstract]. Ital J Gastroenterol 1991; 23 Suppl. 2: 115–6
Dixon MF. Pathophysiology of Helicobacter pylori infection. Scand J Gastroenterol. In press
Lee A. The microbiology and epidemiology of Helicobacter pylori infection. Scand J Gastroenterol. In press
o’Connor HJ. Role of Helicobacter pylori in peptic ulcer disease. Scand J Gastroenterol 1994; Suppl. 201: 11–5
Tytgat GNJ, Lee A, Graham DY, et al. The role of infectious agents in peptic ulcer disease. Gastroenterol Int 1993; 6: 76–89
Bell GD, Powell KU. Eradication of Helicobacter pylori and its effect in peptic ulcer disease. Scand J Gastroenterol 1993; 28 Suppl. 196:7–11
Rauws EAJ, Langenberg W, Houthoff HJ, et al. Campylobacter pyloritis-associated chronic active antral gastritis. A prospective study of its prevalence and the effects of antibacterial and antiulcer treatment. Gastroenterology 1988; 94: 33–40
Solcia E, Villani L, Fiocca R, et al. Effects of eradication of Helicobacter pylori on gastritis in duodenal ulcer patients. Scand J Gastroenterol 1994; 29 Suppl. 201: 28–37
Sipponen P. Gastric cancer — a long term consequence of Helicobacter pylori infection? Scand J Gastroenterol. In press
Bell GD, Powell KU, Burridge SM, et al. Reinfection or recrudescence after apparently successful eradication of Helicobacter pylori infection: implications for treatment of patients with duodenal ulcer disease. Q J Med 1993; 86: 375–82
Borody T, Andrews P, Mancuso N, et al. Helicobacter pylori reinfection 4 years post-eradication. Lancet 1992; 339: 1295
Parsonnet J, Blaser MJ, Perez-Perez GI, et al. Symptoms and risk factors of Helicobacter pylori infection in a cohort of epidemiologists. Gastroenterology 1992; 102: 41–6
Cariani G, Vandelli A, Santini D. Antral and body Helicobacter pylori status after short- and long-term omeprazole monotherapy. Eur J Gastroenterol Hepatol 1992; 4: 867–8
Axon ATR. The role of acid inhibition in the treatment of Helicobacter pylori infection. Scand J Gastroenterol 1994; 29 Suppl. 201: 16–23
Chiba N, Rao BV, Rademaker JW, et al. Meta-analysis of the efficacy of antibiotic therapy in eradicating Helicobacter pylori. Am J Gastroenterol 1992; 87: 1716–27
Pajares JM, Carballo F, Blanco M. Treatment of peptic ulcer disease: is Helicobacter pylori a consideration? Hepatogastroenterology 1992; 39 Suppl. 1: 40–4
Adamek RJ, Wegner M, Birkholz S, et al. Modified combined omeprazole/amoxicillin therapy regimen for eradication of H. pylori — a pilot study [abstract T]. Ir J Med Sci 1992; 161 Suppl. 10: 90
Adamek RJ, Wegner M, Ricken D, et al. Successful Helicobacter pylori eradication: a systemic or topica effect of antibiotics? [abstract]. Gastroenterology 1993; 104: A29
Bayerdorffer E, Mannes GA, Sommer A, et al. High dose omeprazole treatment combined with amoxicillin eradicates Helicobacter pylori. Eur J Gastroenterol Hepatol 1992; 4: 697–702
Bell GD, Powell KU, Burridge SM, et al. Short report: omeprazole plus antibiotic combinations for the eradication of metronidazole-resistant Helicobacter pylori. Aliment Pharmacol 1992; 6: 751–8
Bell GD, Powell KU, Burridge SM, et al. Helicobacter pylori eradication: efficacy and side effect profile of a combination of omeprazole, amoxycillin and metronidazole compared with four alternative regimens. Q J Med 1993; 86: 743–50
Cottrill MRB. The detection of Helicobacter pylori (H. pylori) in patients on long term H2 antagonist treatment and the evaluation of eradication using standard ‘triple’ therapy compared with omeprazole and amoxycillin: a study in a single general practice [abstract]. Gut 1993; 34 Suppl: S37
Labenz J, Gyenes E, Rühl GH, et al. Two weeks treatment with amoxicillin/omeprazole for eradication of Helicobacter pylori. Z Gastroenterol 1992; 30: 776–8
Labenz J, Gyenes E, Riihl GH, et al. Amoxicillin plus omeprazole versus triple therapy for eradication of Helicobacter pylori in duodenal ulcer disease: a prospective, randomized, and controlled study. Gut 1993; 34: 1167–70
Labenz J, Gyenes E, Rühl GH, et al. Omeprazole plus amoxicillin: efficacy of various treatment regimens to eradicate Helicobacter pylori. Am J Gastroenterol 1993; 88: 491–5
Labenz J, Stolte M, Domian C, et al. Omeprazole plus amoxicillin or clarithromycin for eradication of H. pylori in DU disease. Am J Gastroenterol 1993; 88: 1511
Labenz J, Rühl GH, Bertrams J, et al. Efficacy of medium- and high-dose omeprazole plus amoxicillin for eradication of H. pylori in GU disease. Am J Gastroenterol 1993; 88: 1511
Mannes GA, Bayerdorffer E, Hela C, et al. An increasing dose of omeprazole combined with amoxicillin increases the eradication rate of Helicobacter pylori [abstract]. Gastroenterology 1993; 104: A140
Unge P, Ekstrom P. Effects of combination therapy with omeprazole and an antibiotic on Helicobacter pylori and duodenal ulcer disease. Scand J Gastroenterol 1993; 28 Suppl. 196: 17–8
Burette A, Glupczynski Y, DePrez C, et al. Omeprazole alone or in combination with clarithromycin for eradication of H. pylori: results of a randomized double-blind study. Gastroenterology 1993; 194: A49
Di Napoli A, Petrino R, Bellis D, et al. Antral gastritis improvement after therapy of Helicobacter pylori infection with omeprazole and clarithromicin. Ital J Gastroenterol 1991; 23 Suppl. 2: 86
Logan RPH, Gummett PA, Schaufelberger HD, et al. Eradication of Helicobacter pylori with clarithromycin and omeprazole. Gut 1994; 35: 323–6
Cellini L, Marzio L, Di Girolamo A, et al. Enhanced clearing of Helicobacter pylori after omeprazole plus roxithromycin treatment. FEMS Microbiol Lett 1991; 84: 255–8
Marzio L, Cellini L, Grossi L, et al. Treatment of Helicobacter pylori (HP) infection with an association of omeprazole and roxydromicine: a study in vivo and in vitro. Abstract p306. Ital J Gastroenterology 1991; 23 Suppl. 2: 111
Bazzoli F, Zagari RM, Fossi S, et al. Efficacy and tolerability of a short term, low dose triple therapy for eradication of Helicobacter pylori [abstract]. Gastroenterology 1993; 104: A40
Coelho LGV, Passos MCF, Chausson Y, et al. One-week $12.00 therapy heals duodenal ulcer and eradicates H. pylori [abstract]. Gastroenterology 1992; 102: A51
Lamouliatte H, Bernard PH, Cayla R, et al. Controlled study of omeprazole-amoxicillin-tinidazole vs ranitidine-amoxicillin-tinidazole in helicobacter pylori associated duodenal ulcers (DU). Abstract. Final and long term results. Gastroenterology 1992; 102: A106
McCarthy CJ, Collins R, Beattie S, et al. Long term study of omeprazole triple therapy in Helicobacter pylori associated duodenal ulcer disease [abstract]. Gastroenterology 1992; 102: A123
Borody TJ, Brandl S, Andrews P, et al. H. pylori eradication failure (EF) — further treatment possibilities [abstract]. Gastroenterology 1992; 102 Suppl: A43
De Koster E, Burette A, Nyst JF, et al. HP treatment: bismuth, omeprazole, antibiotics [abstract]. Gastroenterology 1991; 100: A52
Forte GB, Bottiglieri ME, Durasco R, et al. Effect of combined therapy on duodenal ulcer associated with Helicobacter pylori infection [abstract T29]. Ir J Med Sci 1992; 161 Suppl. 10:95
Hosking SW, Ling TKW, Yung MY, et al. Randomised controlled trial of short term treatment to eradicate Helicobacter pylori in patients with duodenal ulcer. BMJ 1992; 305: 502–4
Logan RPH, Gummett PA, Misiewicz JJ, et al. Two-week eradication regimen for metronidazole-resistant Helicobacter pylori. Aliment Pharmacol Ther 1993; 7: 149–53
Wagner S, Varrentrapp M, Haruma K, et al. The role of omeprazole (40 mg) in the treatment of gastric Helicobacter pylori infection. Z Gastroenterol 1991; 29: 595–8
Greig MA, Neithercut WD, Hossack M, et al. Suicidal destruction of H pylori mediated by its urease activity [abstract]. Gut 1990; 31: A600
Bode G, Malfertheiner P, Lettner I, et al. The influence of omeprazole on growth, morphology and viability of H. pylori in vitro [abstract]. Ital J Gastroenterol 1991; 23 Suppl: 35
Iwahi T, Satoh H, Nakao M, et al. Lansoprazole, a novel benzimidazole proton pump inhibitor, and its related compounds have selective activity against Helicobacter pylori. Antimicrob Agents Chemother 1991; 35: 490–6
Loo VG, Sherman P, Matlow AG. Helicobacter pylori infection in a pediatric population; in vitro susceptibilities to omeprazole and eight antimicrobial agents. Antimicrob Agents Chemother 1992; 36: 1133–5
Megraud F, Bouchard S, Lamouliatte H. Proton pump inhibitors have an antimicrobial activity against Helicobacter pylori [abstract]. Gastroenterology 1991; 100 Suppl: A123
Sherman P, Shames B, Loo V, et al. Omeprazole therapy for Helicobacter pylori infection. Scand J Gastroenterol 1992; 27: 1018–22
Suerbaum S, Leying H, Klemm K, et al. Antibacterial activity of pantoprazole and omeprazole against Helicobacter pylori. Eur J Clin Microbiol Infect Dis 1991; 10: 92–3
Willems V, Janisch HD, Langmaack H, et al. Omeprazol and ursodeoxycholic-acid (UDCA) have selective activity against Helicobacter pylori [abstract]. Gastroenterology 1992; 102: A189
Ghelani AM, Hale S, Coleman H, et al. Lack of in vitro activity of omeprazole against Campylobacter pylori. J Clin Pathol 1990; 43: 171–2
Bugnoli M, Bayeli PF, Rappuoli R, et al. Inhibition of Helicobacter pylori urease by omeprazole. Eur J Gastroenterol Hepatol 1993; 5: 683–5
Deltenre M, De Koster E, Nyst JF, et al. Clinical results of proton pump inhibitors in the management of Helicobacter pylori related disease [abstract]. Ital J Gastroenterol 1991; 23 Suppl. 2: 2
Figura N, Bugnoli M, Armellini D, et al. Inhibition of Helicobacter pylori urease by omeprazole [abstract T134]. Gut 1993; 34 Suppl: S34
Logan RPH, Gummett PA, Misiewicz JJ, et al. The urease activity of H. pylori before, during & after treatment with omeprazole [abstract]. Gastroenterology 1991; 100 Suppl: A112
Louw JA, Lucke W, Jaskiewicz K, et al. Helicobacter pylori suppression by the proton pump inhibitors (PPI’s): a class effect [abstract]. S Afr Med J 1991; 83: 784
Archimandritis A, Tjivras M, Davaris P, et al. Effect of omeprazole on H. pylori after two weeks of treatment. Ital J Gastroenterol 1991; 23: 357–8
Cariani G, Vandelli A, Santini D, et al. Omeprazole in short-term treatment of Helicobacter pylori positive duodenal ulcer. Ital J Gastroenterol 1991; 23: 597–8
D’Adda T, Bordi C, Lazzaroni M, et al. Long term omeprazole monotherapy is ineffective against Helicobacter pylori infection. Am J Gastroenterol 1992; 87: 681
Daw MA, Deegan P, Leen E, et al. Short report: the effect of omeprazole on Helicobacter pylori and associated gastritis. Aliment Pharmacol Ther 1991; 5: 435–9
Goh KL, Parasakthi N, Peh SC, et al. Healing of duodenal ulcers with omeprazole is associated with clearance of Helicobacter pylori [abstract]. Gastroenterology 1991; 100 Suppl: A71
Goh KL, Tan KK, Anderson PE. Omeprazole may kill Helicobacter pylori. Am J Gastroenterol 1991; 86: 124
Jaskiewicz K, Louw JA, Marks IN. Local cellular and immune response by antral mucosa in patients undergoing treatment for eradication of Helicobacter pylori. Dig Dis Sci 1993; 38: 937–43
Rokkas T, Karameris A, Archavlis E, et al. Omeprazole effectiveness on Helicobacter pylori in duodenal ulcer patients [abstract]. Gastroenterology 1991; 100 Suppl.: A148
Weil J, Bell GD, Powell K, et al. Omeprazole and Helicobacter pylori: temporary suppression rather than true eradication. Aliment Pharmacol Ther 1991; 5: 309–13
Gusmaroli R, Milesi F, Mule P, et al. A comparison of treatment regimens for Helicobacter pylori (HP) associated duodenal ulcer (DU): preliminary results [abstract T46]. Ir J Med Sci 1992; 161 Suppl. 10: 100
Catalano F, Mangiameli A, Inserra G, et al. Omeprazole vs. ranitidine in short-term treatment of Helicobacter pylori positive duodenal ulcer patients. Ital J Gastroenterol 1991; 23: 9–11
Louw JA, Zak J, Jaskiewicz K, et al. Omeprazole may clear but does not eradicate H. pylori. Eur J Gastroenterol Hepatol 1992; 4: 481–5
Rauws EAJ, Langenberg W, Bosma A, et al. Lack of eradication of Helicobacter pylori after omeprazole. Lancet 1991; 337: 1093
Unge P, Gad A, Gnarpe H, et al. Does omeprazole improve antimicrobial therapy directed towards Campylobacter pylori in patients with antral gastritis?. A pilot study. Scand J Gastroenterol 1989; 24 Suppl. 167: 49–54
Vigneri S, Termini R, Scialabba A, et al. Omeprazole therapy modifies the gastric localization of Helicobacter pylori. Am J Gastroenterol 1991; 86: 1276
Vigneri S, Termini R, Di Mario F, et al. Changed distribution of H. pylori after omeprazole therapy for duodenal ulcer [abstract]. Ital J Gastroenterol 1992; 23: 550–1
Bayerdorffer E, Mannes GA, Sommer A, et al. Long-term follow-up after eradication of Helicobacter pylori with a combination of omeprazole and amoxycillin. Scand J Gastroenterol 1993; 28 Suppl: 19–25
Labenz J, Gyenes E, Rühl GH, et al. Helicobacter pylori re-infection and clinical course of peptic ulcer disease in the first year post-amoxicillin/omeprazole treatment. Eur J Gastroenterol Hepatol 1992; 4: 893–6
Labenz J, Borsch G, Gyenes E, et al. Amoxicillin plus omeprazole: a simple and effective therapeutic regimen to eradicate Helicobacter pylori. Eur J Gastroenterol Hepatol 1993; 5: 115–6
Unge P, Gad A, Eriksson K, et al. Amoxicillin added to omeprazole prevents relapse in the treatment of duodenal ulcer patients. Eur J Gastroenterol Hepatol 1993; 5: 325–31
Bell GD, Powell K, Weil J, et al. Experience with omeprazole in combination with either amoxicillin or colloidal bismuth subcitrate in patients with metronidazole-resistant Helicobacter pylori. Eur J Gastroenterol Hepatol 1991; 3: 923–6
Hunt RH. pH and Hp — gastric acid secretion and Helicobacter pylori: implications for ulcer healing and eradication of the organism. Am J Gastroenterol 1993; 88: 481–3
McNulty CAM, Dent JC, Ford GA, et al. Inhibitory antimicrobial concentrations against Campylobacter pylori in gastric mucosa. J Antimicrob Chemother 1988; 22: 729–38
Westblom TU, Duriex DE. Enhancement of antibiotic concentrations in gastric mucosa by H2- receptor antagonist. Implications for treatment of Helicobacter pylori infections. Dig Dis Sci 1991; 36: 25–8
Dotto P, Battaglia G, Franceschi M, et al. Comparison of three different therapeutic regimens for eradicating Helicobacter pylori. Curr Ther Res 1993; 53: 557–64
Moayyedi P, Axon ATR. Efficacy of a new one week triple therapy regime in eradicating Helicobacter pylori. Gut 1994; 35 Suppl. 2: F245
Bertschinger Ph, Brunner J, Flury R, et al. Vergleich der Wirksamkeit von Omeprazole/bismutsubcitrat oder Triple-therapie bei Helicobacter-pylori-gastritis. Schweiz Med Wochenschr 1992; 122: 1446–51
Logan RPH, Gummett PA, Karim NQ, et al. A two week eradication regime for metronidazole resistant Helicobacter pylori [abstract]. Gut 1991; 32: A1227–8
Tucci A, Corinaldesi R, Stanghellini V, et al. One-day therapy for treatment of Helicobacter pylori infection. Dig Dis Sci 1993; 38: 1670–3
Labenz J, Gyenes E, Peitz U, et al. Ciprofloxacin-omeprazole treatment for eradication of Helicobacter pylori [in German]. Z Gastroenterol 1991; 29: 143–5
Labenz J, Borsch G, Gyenes E, et al. Failure of combined cefixime/omeprazole treatment to eradicate Helicobacter pylori. Eur J Gastroenterol Hepatol 1992; 4: 592
Lauritsen K, Rutgersson K, Boiling E, et al. Omeprazole 20 or 40 mg daily for healing of duodenal ulcer? A double-blind comparative study. Eur J Gastroenterol 1992; 4: 995–1000
Marks IN, Danilewitz MD, Garisch JAM. A comparison of omeprazole and ranitidine for duodenal ulcer in South African patients. A multiracial study. Dig Dis Sci 1991; 36: 1395–400
Rubio D, Samitier S, de Rojas D, et al. Comparative multicentric study of omeprazole versus ranitidine in the treatment of duodenal ulcer [in Spanish]. Rev Esp Enferm Dig 1991; 80: 12–6
Wang C-Y, Wang T-H, Lai K-H, et al. Double-blind comparison of omeprazole 20 mg OM and ranitidine 300 mg nocte in duodenal ulcer: a Taiwan multi-centre study. J Gastroenterol Hepatol 1992; 7: 572–6
Zaterka S, Massuda H, Chinzon D, et al. Treatment of duodenal ulcer with omeprazole or ranitidine in a Brazilian population: a multicentre double-blind, parallel group study. Am J Gastroenterol 1993; 88: 397–401
Bamberg P, Caswell CM, Frame MH, et al. Alimentary tract and pancreas. A meta-analysis comparing the efficacy of omeprazole with H2-receptor antagonists for acute treatment of duodenal ulcer in Asian patients. J Gastroenterol Hepatol 1992; 7: 577–85
Delle Fave G, Annibale B, Franceschi M, et al. Omeprazole versus famotidine in the short-term treatment of duodenal ulcer disease. Aliment Pharmacol Ther 1992; 6: 469–78
Morgan DG, Burget DW, Howden CW, et al. Rates of duodenal ulcer (DU) healing by drug classes: a meta-analysis. Gastroenterology 1993; 104: A150
Petite JP, Slama J-L, Licht H, et al. Lansoprazole and omeprazole in the treatment of duodenal ulcer: a multicentric double-blind comparative trial. Gastroenterol Clin Biol 1993; 17: 334–40
Louw JA, van Rensburg C, Simjee AE, et al. Lansoprazole versus omeprazole in duodenal ulcer healing [abstract], S Afr Med J 1993; 83: 777
Ekström P, Unge P, Carling L, et al. Lansoprazole vs omeprazole in active duodenal ulcer — a healing study [abstract]. Gastroenterology 1993; 104: A74
Ekstrom P, Unge P, Ahlberg J, et al. Lansoprazole versus omeprazole in active duodenal ulcer — a healing study. Scand J Gastroenterol 1992; 27 Suppl. 190: 34
Beker JA, Bianchi Porro G, Delle Fave G, et al. Efficacy of pantoprazole, compared to omeprazole in duodenal ulcer: European multicentre study. Ital J Gastroenterol 1993; 25 Suppl. 1: 16
Tulassay Z, Szalay F, Acharya M. Omeprazole versus ranitidine in the treatment of resistant duodenal ulcer. Gut 1992; 33: 863
Bayerdorffer E, Mannes GA, Hochter W, et al. Antibacterial treatment of gastric ulcers — a German gastric ulcer study [abstract]. Gastroenterology 1993; 104: A40
Hosking SW, Ling TKW, Chung SCS, et al. Duodenal ulcer helaing by eradication of Helicobacter pylori without anti-acid treatment: randomised controlled trial. Lancet 1994; 343: 508–10
Graham DY, Colon-Pagan J, Morse RS, et al. Ulcer recurrence following duodenal ulcer healing with omeprazole, ranitidine, or placebo: a double-blind, multicenter, 6-month study. Gastroenterology 1992; 102: 1289–94
Kager L, Lindberg G, Nilsson LH, et al. The effect of omeprazole and ranitidine on ulcer healing, relief of symptoms, and incidence of adverse events in the treatment of duodenal ulcer patients. Hepatogastroenterology 1991; 38: 287–90
Boonyapisit S, Lai KH, Goh KL, et al. Prevention of duodenal ulcer relapse during maintenance treatment with omeprazole 20 mg o.m. for 12 months compared with placebo — an Asian multicentre trial [abstract 146]. IXth Asian Pacific Congress of Gastroenterology, Nov 29-Dec 3, Bangkok, Thailand, 1992
Del Piano M, Manfredda I, Montino F, et al. The maintenance treatment of duodenal ulcer with omeprazole [abstract]. Gastrointest Endosc 1993; 39: 273
Festen HPM. Prevention of duodenal ulcer relapse by long-term treatment with omeprazole. Scand J Gastroenterol 1994; 29 Suppl. 201:39–41
Interdisciplinary Group for Ulcer Study. Long-term study with different dosages of omeprazole for preventing relapses of duodenal ulcer disease. Ital J Gastroenterol 1993; 25 Suppl 1: 94
Bianchi Porro G, Boiling E, Barbara L, et al. Maintenance treatment with omeprazole in the prevention of duodenal ulcer relapse: a double-blind comparative trials [abstract]. Gastroenterology 1990; 98 Suppl. 5: A21
Lauritsen K, Andersen BN, Laursen LS, et al. Weekend administration of omeprazole in the prevention of duodenal ulcer relapse: A double-blind comparative trials. Gastroenterology 1989; 96: A289
Lauritsen K, Andersen BN, Laursen LS, et al. Omeprazole 20 mg three days a week and 10 mg daily in prevention of duo-denal ulcer relapse. Double-blind comparative trial. Gastroenterology 1991; 100: 663–9
Ferrara A, Prada A, Colombo E, et al. Maintenance treatment of duodenal ulcer with omeprazole: three different regimens. Ital J Gastroenterol 1993; 25 Suppl. 1: 77
Graham DY, Lew GM, Klein PD, et al. Effect of treatment of Helicobacter pylori infection on the long-term recurrence of gastric or duodenal ulcer. A randomized, controlled study. Ann Intern Med 1992; 116: 705–8
Labenz J, Rühl GH, Bertrams J, et al. Clinical course of duodenal ulcer disease one year after omeprazole plus amoxicillin or triple therapy plus ranitidine for cure of Helicobacter pylori infection. Eur J Gastroenterol Hepatol 1994; 6: 293–7
Sobhani I, Chastang C, de Korwin JD, et al. Cure of duodenal ulcer: eradication of Helicobacter pylori versus maintenance of healing [abstract]. Results of a double blind randomized trial. Gastroenterology 1993; 104 Suppl: A195
Kawaguchi Y, Suko H, Matsuzaki H, et al. Clinical usefulness of omeprazole (Omeprazon Rm) in patients with gastric and duodenal ulcer [in Japanese]. Shinryo to Shinyaku 1993; 30: 319–30
Sollano JD, Espiritu AC, Alvarez SZ, et al. An open trial on short-term omeprazole therapy for gastric and duodenal ulcers. Gastroenterol Jpn 1991; 26: 271–4
Choi KW, Sun HS, Yoon CM, et al. A double-blind, randomized, parallel group study of omeprazole and ranitidine in Korean patients with gastric ulcer. J Gastroenterol Hepatol 1994; 9: 118–23
Italian Cooperative Group on Omeprazole. Omeprazole 20 mg uid and ranitidine 150 mg bid in the treatment of benign gastric ulcer. Hepatogastroenterology 1991; 38: 400–3
Niwa Y, Nakazawa S, Tsukamoto Y, et al. A new method for evaluating gastric ulcer healing by endoscopic ultrasonography. Scand J Gastroenterol 1991; 26: 457–64
Howden CW, Burget DW, Wilkinson J, et al. A comparison of different drug classes with respect to rapidity of healing of gastric ulcer. Gastroenterology 1993; 104: A105
Florent C, Forestier S, Joubert-Collin M. Lansoprazole versus omeprazole: efficacy and safety in acute gastric ulcer [abstract]. Gastroenterology 1993; 104 Suppl: A80
Steadman CJ. Prophylaxis against NSAID-induced ulcers. Med J Aust 1992; 157: 801–3
van Berge Henegouwen GP, Smout AJPM. The management of non-steroidal anti-inflammatory drug-induced gastroduodenal ulcers. Scand J Gastroenterol 1991; 26 Suppl. 188: 87–91
Agrawal NM. Anti-inflammatories and gastroduodenal damage: therapeutic options. Eur J Rheumatol Inflam 1993; 13: 17–24
Bianchi Porro G, Lazzaroni M. Prevention and treatment of non-steroidal gastroduodenal lesions. Eur J Gastroenterol Hepatol 1993; 5: 420–32
Yeomans ND, Skeljo MV, Giraud AS. The role of acid regulation in the treatment of NSAID-induced mucosal damage. Digestion 1992; 51 Suppl. 1: 3–10
Walan A, Bader J-P, Classen M, et al. Effect of omeprazole and ranitidine on ulcer healing and relapse rates in patients with benign gastric ulcer. N Engl J Med 1989; 320: 69–75
Bianchi Porro G, Santalucia F, Petrillo M. Omeprazole v sucralfate in the treatment of NSAID-induced gastric and duodenal ulcer [abstract]. Gut 1990; 31: A1175
Gubbins GP, Schubert TT, Attanasio F, et al. Helicobacter pylori seroprevalence in patients with rheumatoid arthritis: effect of nonsteroidal anti-inflammatory drugs and gold compounds. Am J Med 1992; 93: 412–8
Jones STM, Clague RB, Eldridge J, et al. Serological evidence of infection with Helicobacter pylori may predict gastrointestinal intolerance to non-steroidal anti-inflammatory drug (NSAID) treatment in rheumatoid arthritis. Br J Rheumatol 1991; 30: 16–20
Loeb DS, Talley NJ, Ahlquist DA, et al. Long-term nonsteroidal anti-inflammatory drug use and gastroduodenal injury: the role of Helicobacter pylori. Gastroenterology 1992; 102: 1899–905
Schubert TT, Bologna SD, Nensey Y, et al. Ulcer risk factors: interactions between Helicobacter pylori infection, nonsteroidal use, and age. Am J Med 1993; 94: 413–8
Weinbeck M, Barnert J. Epidemiology of reflux disease and reflux esophagitis. Scand J Gastroenterology 1989; 24 Suppl. 156:7–13
Hetzel DJ, Heddle R. Gastroesophageal reflux disease, pH monitoring, and treatment. Curr Opin Gastroenterology 1993; 9: 629–40
Bell NJV, Hunt RH. Role of gastric acid suppression in the treatment of gastro-oesophageal reflux disease. Gut 1992; 33: 118–24
Dent J. Roles of gastric acid and pH in the pathogenesis of gastro-oesophageal reflux disease. Scand J Gastroenterol 1994; 29 Suppl. 201:55–61
Bell NJV, Burget D, Howden CW, et al. Appropriate acid suppression for the management of gastro-oesophageal reflux disease. Digestion 1992; 51 Suppl. 1: 59–67
Sontag SJ, Hirschowitz BI, Holt S, et al. Two doses of omeprazole versus placebo in symptomatic erosive esophagitis: the U.S. multicentre study. Gastroenterology 1992; 102: 109–18
Bate CM, Crowe JP, Dickinson RJ, et al. Reflux oesophagitis resolves more quickly with omeprazole 20 mg once daily than with ranitidine 150 mg twice daily: omeprazole 40 mg once daily provides further benefit in unresponsive patients. Br J Clin Res 1991; 2: 133–48
Bianchi Porro G, Pace F, Peracchia A, et al. Short-term treatment of refractory reflux esophagitis with different doses of omeprazole or ranitidine. J Clin Gastroenterol 1992; 15: 192–8
Hazenburg BP, Geraedts AAM, de Groot GH. Omeprazole versus ranitidine in the treatment of symptomatic mild reflux oesophagitis: a Dutch multi-centre trial [abstract]. Gut 1994; 35 Suppl. 2: W26
Hungin APS, Gunn SD, Bate CM, et al. A comparison of the efficacy of omeprazole 20 mg once daily with ranitidine 150 mg bd in the relief of symptomatic gastro-oesophageal reflux disease in general practice. Br J Clin Res 1993; 4: 73–88
Italian Reflux Oesophagitis Study Group. Omeprazole produces significantly greater healing of erosive or ulcerative reflux oesophagitis than ranitidine. Eur J Gastroenterol Hepatol 1991; 3: 511–7
James OFW, Parry-Billings KS. Comparison of omeprazole and histamine H2-receptor antagonists in the treatment of elderly and young patients with reflux oesophagitis. Age Ageing 1994; 23: 121–6
Hill ADK, o’Donoghue DP. Omeprazole in refractory reflux oesophagitis. Gullet 1991; 1: 81–3
Koop H, Katschinski M, Arnold R. Medical therapy of stenotic reflux oesophagitis — complete healing by dilatation and omeprazole [in German]. Med Klin 1991; 86: 566–8
Laursen LS, Bondesen S, Hansen J, et al. Omeprazole 20 mg or 40 mg daily for the treatment of gastroesophageal reflux disease? A double-blind comparative study [abstract]. Gastroenterology 1992; 102: A110
Chiba N, de Gara CJ, Burget DW, et al. Rapidity of healing in GERD: a comparison of different drug classes by meta-analysis. Gastroenterology 1993; 104: A53
Mundo F, Felix R, Aguilar J, et al. Omeprazole vs ranitidine plus cisapride in the treatment of reflux esophagitis. Comparative endoscopic study. Am J Gastroenterol 1992; 87: 1254
Robinson M, Decktor D. Omeprazole (OME) is superior to ranitidine (RAN) plus metoclopramide (MET) in the short-term treatment of erosive esophagitis. Am J Gastroenterol 1991; 86: 1302
Dallera F, Scanzi G, Gendarini A, et al. Effectiveness of omeprazole associated with levosulpiride in therapy of reflux esophagitis [in Italian]. Minerva Med 1992; 83: 541–3
Hatlebakk JG, Berstad A, Carling L, et al. Lansoprazole versus omeprazole in short-term treatment of reflux oesophagitis. Results of a Scandinavian Multicentre Trial. Scand J Gastroenterol 1993; 28: 224–8
Corallo J, Vicari F, Forestier S, et al. Lansoprazole in acute treatment of reflux oesophagitis [abstract]. Gastroenterology 1993; 104 Suppl: A58
Brossard E, Ollyo J-B, Monnier Ph, et al. Columnar-type epithelium (Barrett’s epithelium) develops after healing in 18% of adults with erosive or ulcerative reflux esophagitis [abstract]. Gastroenterology 1991; 100: A36
Gore S, Healey CJ, Sutton R, et al. Regression of columnar lined (Barrett’s) oesophagus with continuous omeprazole therapy. Aliment Pharmacol Ther 1993; 7: 623–8
Galmiche JP, Dumas R, Boyer J, et al. Long-term omeprazole effects on Barrett’s mucosa [abstract]. Gastroenterology 1993; 104: A85
Bologna S, Blumenkehl M, Schubert TT, et al. Barrett’s esophagus response to long term omeprazole therapy [abstract t15]. Gastrointest Endosc 1992; 38: 229
Francis J, Shaffer R, Kadakia S, et al. Effect of omeprazole on Barrett’s epithelium at 3 and 9 months of therapy [abstract]. Gastroenterology 1993; 104 Suppl: A80
Igbal TH, Neumann CS, Cooper BT. Omeprazole treatment of patients with Barrett’s oesophagus [abstract]. Gut 1993; 34 Suppl: S19
Kundrotas L, Ward RW. Omeprazole vs ranitidine in patients with progressive systemic sclerosis and symptomatic esophagitis [abstract 33]. Am J Gastroenterol 1992; 87; 1250
Hendel L, Hage E, Hendel J, et al. Omeprazole in the long term treatment of severe gastro-oesophageal reflux disease in patients with systemic sclerosis. Aliment Pharmacol Ther 1992; 6: 565–77
Hendel L, Hage E, Hendel J, et al. Therapeutic monitoring of omeprazole treatment of gastro-oesphageal reflux disease [abstract]. Gastroenterology 1993; 104 Suppl: A99
Dalzell AM, Searle JW, Patrick MK. Treatment of refractory ulcerative oesophagitis with omeprazole. Arch Dis Child 1992; 68: 641–2
Gunasekaran TS, Hassall EG. Efficacy and safety of omeprazole for severe gastroesophageal reflux in children. J Pediatr 1993; 123: 148–54
Krischer J, Noblett H, Sandhu BK. The use of proton pump blocker for resistant reflux oesophagitis in children [abstract F242]. Gut 1992; 33 Suppl. 1: S61
Olbe L, Lundell L. Medical treatment of reflux esophagitis. Hepatogastroenterology 1992; 39: 322–4
Sekiguchi T. Initial and maintenance therapy of omeprazole in reflux oesophagitis [in Japanese]. Yakuri to Chiryo 1992; 20: 625–31
Dent J, Yeomans ND, Mackinnon M, et al. Omeprazole versus ranitidine for prevention of relapse of oesophagitis. A controlled double-blind trial of their efficacy and safety. Gut. In press
Koop H, Arnold R. Long-term maintenance treatment of reflux esophagitis with omeprazole. Prospective study in patients with H2-blocker-resistant esophagitis. Dig Dis Sci 1991; 36: 552–7
Laursen LS, Bondesen S, Hansen J, et al. Omeprazole 10 mg or 20 mg daily for the prevention of relapse in gastroesophageal reflux disease? A double-blind comparative study [abstract]. Gastroenterology 1992; 102: A109
Lundell L, Backman L, Ekström P, et al. Prevention of relapse of reflux oesophagitis after endoscopic healing: the efficacy and safety of omeprazole compared with ranitidine. Scand J Gastroenterol 1991; 26: 248–56
Sontag S, Robinson M, Roufail W, et al. Daily omeprazole (OME) is needed to maintain healing in erosive esophagitis (EE). AU.S. multicenter double-blind study [abstract 65]. Am J Gastroenterol 1992; 87: 1258
Toledo-Pimentel V, Ros E, Bordas JM, et al. Reflux esophagitis refractory to high-dose histamine H2-antagonists. Healing with omeprazole [abstract]. Gastroenterology 1992; 102: A179
Hetzel DJ. Controlled clinical trials of omeprazole in the long-term management of reflux disease. Digestion 1992; 51 Suppl. 1:35–42
Bank S, Magier D, Greenberg R, et al. Alternate day omeprazole maintenance therapy in H2RA resistant esophagitis-clinical, gastrin & ECL effects for up to 3 years [abstract]. Gastroenterology 1992; 102: A35
Marks R, Richter JE, Rizzo J, et al. Omeprazole versus H2-receptor antagonists in treating patients with peptic stricture and esophagitis. Gastroenterology 1994; 106: 907–15
Carr SJ, Wicks AC. Omeprazole and oesophageal stricture [correspondence]. Lancet 1992; 339: 316
Jensen RT, Maton PN, Gardner JD. Current management of Zollinger-Ellison syndrome. Drugs 1986; 32: 188–96
Frucht H, Maton PN, Jensen RT. Use of omeprazole in patients with Zollinger-Ellison syndrome. Dig Dis Sci 1991; 36: 394–404
Maton PN. Role of acid suppressants in patients with Zollinger-Ellison syndrome. Aliment Pharmacol Ther 1991; 5 Suppl. 1: 25–35
Metz DC, Pisegna JR, Fishbeyn VA, et al. Currently used doses of omeprazole in Zollinger-Ellison syndrome are too high. Gastroenterology 1992; 103: 1498–508
Rhodes JM. The medical management of Zollinger-Ellison syndrome. Q J Med New Series 1991; 78: 191–3
Tani N. Zollinger-Ellison. Application of proton pump inhibitor to special conditions; Zollinger-Ellison syndrome [in Japanese]. Nippon Rinsho 1992; 50: 154–9
Ramdani A, Paul G, Ruszniewski Ph, et al. Comparative efficacy of lansoprazole and omeprazole on 24-hour intragastric pH measurement in 9 cases of Zollinger-Ellison syndrome [abstract]. Gastroenterology 1992; 102: A151
Daneshmend TK, Hawkey CJ, Langman MJS, et al. Omeprazole versus placebo for acute upper gastrointestinal bleeding: randomised double blind controlled trial. BMJ 1992; 304: 143–7
Brunner GHG, Thiesemann C. The potential clinical role of intravenous omeprazole. Digestion 1992; 51 Suppl. 1: 17–20
Gabbrielli M, Pennati P, Trallori G, et al. Use of intravenous omeprazole in emergency cases of gastroduodenal hemorrhage. Am J Gastroenterol 1992; 87: 1229
o’Leary MJ, Park GR. Intravenous omeprazole in upper gastrointestinal haemorrhage in critically ill patients. Digestion 1991; 48: 59–60
Panos MZ, Walt RP. Current management of bleeding peptic ulcer. A review. Drugs 1993; 46: 269–80
Brown C, Rees WDW. Drug treatment for acute upper gastrointestinal bleeding. BMJ 1992; 304: 135–6
Olsson GL, Hallen B, Hambraeus-Jonzon K. Aspiration during anaesthesia: a computer-aided study of 185 358 anaesthetics. Acta Anaesthesiol Scand 1986; 30: 84–92
Ruffalo RL. Aspiration pneumonitis: risk factors and management of the critically ill patient. DICP, Ann Pharmacother 1990; 24: S12–6
Moore J, Flynn RJ, Sampaio M, et al. Effect of single-dose omeprazole on intragastric acidity and volume during obstetric anaesthesia. Anaesthesia 1989; 44: 559–62
Orr DA, Bill KM, Gillon KRW, et al. Effects of omeprazole, with and without metoclopramide, in elective obstetric anaesthesia. Anaesthesia 1993; 48: 114–9
Gin T, Ewart MC, Yau G, et al. Effect of oral omeprazole on intragastric pH and volume in women undergoing elective caesarean section. Br J Anaesth 1990; 65: 616–9
Cruickshank RH, Morrison DA, Bamber PA, et al. Effect of I.V. omeprazole on the pH and volume of gastric contents before surgery. Br J Anaesth 1989; 63: 536–40
Atanassoff PG, Alon E, Pasch T. Effects of single-dose intravenous omeprazole and ranitidine on gastric pH during general anesthesia. Anesth Analg 1992; 75: 95–8
Ewart MC, Yau G, Gin T, et al. A comparison of the effects of omeprazole and ranitidine on gastric secretion in women undergoing elective caesarean section. Anaesthesia 1990; 45: 527–30
Yau G, Kan AF, Gin T, et al. A comparison of omeprazole and ranitidine for prophylaxis against pneumonitis in emergency Caesarean section. Anaesthesia 1992; 47: 101–4
Bouly A, Nathan N, Feiss P. Comparison of omeprazole with cimetidine for prophylaxis of acid aspiration in elective surgery. Eur J Anaesthesiol 1993; 10: 209–13
Seveso M, Pesci M, Lualdi M, et al. Studio comparativo degli effetti della famotidina e dell’omeprazolo nella profilassi della sindrome da aspirazione di contenuto gastrico in chirurgia elettiva [in Italian]. Minerva Anesthesiol 1992; 58: 207–10
Barradell LB, McTavish D. Omeprazole: a pharmacoeconomic evaluation of its use in duodenal ulcer and reflux oesophagitis. Pharmacoeconomics 1993; 3: 482–510
Diaz de Rojas F, Rodrigo-Saez L. Cost-effectiveness of omeprazole in the treatment of duodenal ulcer — a Spanish study. J Drug Dev 1993; 6: 49–55
Frampton JE, McTavish D. A pharmacoeconomic evaluation of ranitidine in some acid-related disorders. Pharmacoeconomics. In press
Walan A, Eriksson S. Long-term consequences with regard to clinical outcome and cost-effectiveness of episodic treatment with omeprazole or ranitidine for healing of duodenal ulcer. Scand J Gastroenterol 1994; 29 Suppl. 201: 91–7
Unge P. Cost-effective management of duodenal ulcer; a comparison of omeprazole plus amoxicillin in Helicobacter pylori eradication and ranitidine in maintenance treatment [abstract]. Gastroenterology 1993; 104 Suppl.: A27
Jönsson B, Stålhammar N-O. The cost effectiveness of omeprazole and ranitidine in intermittent and maintenance treatment of reflux oesophagitis — the case of Sweden. Br J Med Econ 1993; 6: 111–26
Joelson S, Joelson I-B, Lundborg P, et al. Safety experience from long-term treatment with omeprazole. Digestion 1992; 51 Suppl. 1:93–101
Simon TJ, Bradstreet DC. Comparative tolerability profile of omeprazole in clinical trials. Dig Dis Sci 1991; 36: 1384–9
Fried M, Siegrist H, Frei R, et al. Duodenal bacterial overgrowth during treatment with omeprazole in outpatients [abstract]. Gastroenterology 1992; 102: A71
Kowdley K, Saltzman J, Pedrosa M, et al. Bacterial overgrowth in subjects with atrophic gastritis or omeprazole-induced achlorhydria does not cause malabsorption [abstract 289]. Am J Gastroenterology 1992; 87: 1314
Verdu E, Viani F, Armstrong D, et al. Effect of omeprazole on intragastric bacterial counts, nitrates, nitrites, and N-nitroso compounds. Gut 1994; 35: 455–60
Burger DM, Hopman WPM, Hekster YA, et al. Antimicrobial drug use during treatment with omeprazole. J Pharmaco-epidemiol 1991; 2: 3–14
Creutzfeldt W. Efficacy and safety of proton pump inhibitors during long-term treatment. In Olbe, Itoh, editors. Safety and efficacy of proton pump inhibitors. Amsterdam: Excerpta Medica, 1993: 23–36
Poynter D, Selway SAM. Neuroendocrine cell hyperplasia and neuroendocrine carcinoma of the rodent fundic stomach. Mutation Res 1991; 248: 303–19
Bunce H, Cann PA. Adverse drug reaction [correspondence]. Pharm J 1993; 250: 73
Cox NH. Acute disseminated epidermal necrosis due to omeprazole [correspondence]. Lancet 1992; 340: 857
Haeney MR. Angio-oedema and urticaria associated with omeprazole. BMJ 1992; 305: 870
Convens C, Verhelst J, Mahler C. Painful gynaecomastia during omeprazole therapy [correspondence]. Lancet 1991; 338: 1153
Lindquist M, Edwards IR. Endocrine adverse effects of omeprazole. BMJ 1992; 305: 451–2
Santucci L, Farroni F, Fiorucci S, et al. Gynecomastia during omeprazole therapy [correspondence]. N Engl J Med 1991; 324: 635
Bank S, Greenberg R. Alternate day omeprazole in H2 receptor-antagonist (H2RA) resistant reflux oesophagitis [abstract]. Gastroenterology 1991; 100 Suppl: A29
Raoul JL, Bretagne JF. Zollinger-Ellison syndrome, antisecretory treatment, and body weight [correspondence]. Dig Dis Sci 1992; 37: 1308
Dutertre JP, Soutif D, Jonville AP, et al. Sexual disturbances during omeprazole therapy [correspondence]. Lancet 1991; 338: 1022
Sellapah S. An unusual dose effect of omeprazole: case report. Br J Gen Pract 1990;40:389
Christensen PB, Albertsen KEP, Jensen P. Renal failure after omeprazole [correspondence]. Lancet 1993; 341: 55
Kuiper JJ. Omeprazole-induced acute interstitial nephritis [correspondence]. Am J Med 1993; 95: 248
Ruffenach SJ, Siskind MS, Lien YH. Acute interstitial nephritis due to omeprazole. Am J Med 1992; 93: 472–3
Lee M-L, Piper DW, Fischer GO, et al. Lichen spinulosus after the ingestion of omeprazole [correspondence]. Med J Aust 1989; 150: 410
Marks DR, Joy JV, Bonheim NA. Hemolytic anemia associated with the use of omeprazole. Am J Gastroenterol 1991; 86: 217
Brunner G, Thiesemann C, Ratz H. High plasma concentrations of proton pump inhibitors cause peripheral oedema in female patients. Gastroenterology 1993; 104 Suppl: A48
Jochem V, Kirkpatrick R, Greenson J, et al. Fulminant hepatic failure related to omeprazole. Am J Gastroenterol 1992; 87: 523–5
Gonthier R, Bouchou K, Guy C, et al. Severe hyponatraemia under omeprazole [in French]. Presse Med 1993; 22: 176
Rudelli A, Leduc I, Traulle C, et al. Thrombocytopenia after treatment with omeprazole. Presse Med 1993; 22: 966
Garrote FJ, Lacambra C, Del Ser T, et al. Subacute myopathy during omeprazole therapy [correspondence]. Lancet 1992; 340: 672
Larner AJ, Lendrum R. Oesophageal candidiasis after omeprazole therapy. Gut 1992; 33: 860–1
Mosimann F. Esophageal candidiasis, omeprazole therapy, and organ transplantation — a word of caution [correspondence]. Transplantation 1993; 56: 492–3
Schultz K, Simon L, Toth M. Severe adverse effect of short-term omeprazole treatment - acute hemorrhagic-necrotic/bacterial/gastritis [abstract t660]. Pediatr Res 1991; 29: 113A
Anon. Astra remain calm after another Losec scare. Pharm Bus News 1994; 9(215): 1–2
Schonhofer PS. Intravenous omeprazole and blindness. Lancet 1994; 343: 665
Creutzfeldt WC, Blum AL. Safety of omeprazole [correspondence]. Lancet 1994; 343: 1098
Bertaccini G, Coruzzi G. Untoward reactions to gastric anti-secretory drugs. Ital J Gastroenterol 1992; 24: 470–1
Halabi A, Kirch W. Cardiovascular effects of omeprazole and famotidine. Scand J Gastroenterol 1992; 27: 753–6
Koop H. Review article: metabolic consequences of long-term inhibition of acid secretion by omeprazole. Aliment Pharmacol Ther 1992; 6: 399–406
Goggins MG, o’Brian S, Kelleher B, et al. Omeprazole causes malabsorption of protein-bound cobalamin [abstract]. Gastroenterology 1993; 104 Suppl: A88
Klinkenberg-Knol E, Kuipers E, Lamers C, et al. Cobalamin absorption during omeprazole treatment: short and long-term studies [abstract]. Gastroenterology 1993; 104: A77
Marcuard SP, Albernaz L, Khazanie PG. Omeprazole therapy causes malabsorption of cyanocobalamin (vitamin B12). Ann Intern Med 1994; 120: 211–5
Hixson LJ, Kelley CL, Jones WN, et al. Current trends in the pharmacotherapy for gastroesophageal reflux disease. Arch Intern Med 1992; 152: 717–23
McCloy RF. Implications of a review of long term safety of omeprazole and management strategies for peptic disease. Hepatogastroenterology 1992; 39: 90–1
Cadiot G, Lehy T, Ruszniewski P, et al. Gastric endocrine cell evolution in patients with Zollinger-Ellison syndrome. Influence of gastrinoma growth and long-term omeprazole treatment. Dig Dis Sci 1993; 38: 1307–17
Caruana P, Azzoni C, Bertele A, et al. Focal oxyntic gland atrophy with endocrine cell hyperplasia in Zollinger-Ellison syndrome during omeprazole treatment. Histopathol 1992; 21: 359–63
Creutzfeldt W, Lamberts R. Inter-relationship between serum gastrin levels, gastric mucosal histology and gastric endocrine cell growth. Digestion 1992; 51 Suppl. 1: 76–81
Lamberts R, Creutzfeldt W, Strüber HG, et al. Long-term omeprazole therapy in peptic ulcer disease: gastrin, endocrine cell growth, and gastritis. Gastroenterology 1993; 104: 1356–70
Havu N, Maaroos MI, Sipponen P. The association between chronic atrophic gastritis and focal hyperplasia of argyrophil cells in gastric ulcer patients. Scand J Gastroenterol 1991; 26 Suppl. 183: F31
Solcia E, Fiocca R, Havu N, et al. Gastric endocrine cells and gastritis in patients receiving long-term omeprazole treatment. Digestion 1992; 51 Suppl. 1: 82–92
Andersson T. Omeprazole drug interaction studies. Clin Pharmacokinet 1991;21: 195–212
Humphries TJ. Clinical implications of drug interactions with the cytochrome P-450 enzyme system associated with omeprazole. Dig Dis Sci 1992; 36: 1665–9
Andersson T, Andren K, Cederberg C, et al. Effect of omeprazole and cimetidine on plasma diazepam levels. Eur J Clin Pharmacol 1990; 39: 51–4
Gugler R, Jensen JC. Omeprazole inhibits elimination of diazepam [correspondence]. Lancet 1984; 1: 969
Gugler R, Jensen JC. Omeprazole inhibits oxidative drug metabolism. Studies with diazepam and phenytoin in vivo and 7-ethoxycoumarin in vitro. Gastroenterology 1985; 89: 1235–41
Ahmad S. Omeprazole-warfarin interaction [correspondence]. South Med J 1991; 84: 674–5
Sutfin T, Balmer K, Bostrom H, et al. Stereoselective interaction of omeprazole with warfarin in healthy men. Ther Drug Monit 1989; 11: 176–84
Unge P, Svedberg L-E, Nordgren A, et al. A study of the interaction of omeprazole and warfarin in anticoagulated patients. Br J Clin Pharmacol 1992; 34: 509–12
Nousbaum JB, Berthou F, Carlhant D, et al. Four-week treatment with omeprazole increases the metabolism of caffeine. Am J Gastroenterol 1994; 89: 371–5
Andersson T, Lagerstrom PO, Unge P. A study of the interaction between omeprazole and phenytoin in epileptic patients. Ther Drug Monit 1990; 12: 329–33
Prichard PJ, Walt RP, Kitchingman GK, et al. Oral phenytoin pharmacokinetics during omeprazole therapy. Br J Clin Pharmacol 1987; 24: 543–5
Petersen K-U. Omeprazol und das Cytochrom P450-System der Leber. Leber Magen Darm 1993; 23: 186–92
Arranz R, Yanez E, Franceschi JL, et al. More about omeprazole-cyclosporine interaction [correspondence]. Am J Gastroenterol 1993; 88: 154
Schouler L, Dumas F, Couzigou P, et al. Omeprazole-cyclosporin interaction [correspondence]. Am J Gastroenterol 1991; 86: 1097
Gerber MC, Tejwani GA, Gerber N, et al. Drug interactions with cimetidine: an update. Pharmacol Ther 1985; 27: 353–70
Hansten PD. Drug interactions with antisecretory agents. Aliment Pharmacol Ther 1991; 5 Suppl. 1: 121–8
Armstrong D, Nicolet M, Monnier P, et al. Maintenance therapy: is there still a place for antireflux surgery?. World J Surg 1992; 16: 300–7
Partipilo ML, Woster PS. The role of Helicobacter pylori in peptic ulcer disease. Pharmacotherapy 1993; 13: 330–9
Barradell LB, Whittington R, Benfield P. Misoprostol. Pharmacoeconomics of its use as prophylaxis against gastro-duodenal damage induced by nonsteroidal anti-inflammatory drugs. Pharmacoeconomics 1993; 3: 140–70
Bolten W, Miehlke K. Therapie und Prävention der nichtsteroidalen Antirheumatika-assoziierten Gastropathie. Med Welt 1992; 43: 831–9
Fenn GC. Protection of the gastric mucosa from NSAIDs. [correspondence]. NZ Med J 1992; 105: 436
Fenn GC, Robinson GC. Misoprostol — a logical therapeutic approach to gastroduodenal mucosal injury induced by nonsteroidal anti-inflammatory drugs?. J Clin Pharm Ther 1991; 16: 385–409
Kühler T, Fryklund J, Bergman N-Å, et al. Omeprazole and analogues inhibit urea-dependent ammonia production by Helicobacter pylori. Astra Hassle, Sweden, data on file
Schönhöfer PS. Safety of omeprazole and lansoprazole [correspondence]. Lancet 1994; 343: 1369–70
Author information
Authors and Affiliations
Additional information
Various sections of the manuscript reviewed by: G.D. Bell, Department of Medicine, Ipswich Hospital, Ipswich, England; F. Catalano, Istituto di Medicina Medica, Ospedale Garibaldi, Catania, Italy; W. Creutzfeldt, Division of Gastroenterology and Endocrinology, Department of Medicine, Georg-August- University Göttingen, Göttingen, Germany; J.G. Hatlebakk, Medical Department A, Haukeland Hospital, Bergen, Norway; C.J. Hawkey, Department of Medicine, Division of Gastroenterology, University Hospital, Nottingham, England; J. Labenz, Department of Internal Medicine, Elisabeth Hospital, Essen, Germany; M.J.S. Langman, Department of Internal Medicine, Queen Elizabeth Medical Centre, Birmingham, England; K. Lauritsen, Department of Medical Gastroenterology S, Odense University Hospital, Odense, Denmark; R.P.H. Logan, St Charles Hospital, London, England; I.N. Marks, Gastrointestinal Clinic, Groote Schuur Hospital, Cape Town, South Africa; A. Tucci, Istituto di Clinica Medica E Gastroenterologia dell’ Università di Bologna, Bologna, Italy; P. Unge, Department of Internal Medicine, Sandviken Hospital, Sandviken, Sweden; K.G. Wormsley, Ninewells Hospital, Dundee, Scotland.
Rights and permissions
About this article
Cite this article
Wilde, M.I., McTavish, D. Omeprazole. Drugs 48, 91–132 (1994). https://doi.org/10.2165/00003495-199448010-00008
Published:
Issue Date:
DOI: https://doi.org/10.2165/00003495-199448010-00008