
Abstract
Background and objectives: Gemcitabine (2,2-difluorodeoxycytidine [dFdC]) can be administered in a standard 30-minute infusion or in a fixed-dose-rate (FDR) infusion to maximize the rate of accumulation of triphosphate, its major intracellular metabolite. The standard 30-minute infusion requires dose adjustment in patients with organ dysfunction, especially in patients with elevated baseline serum bilirubin levels. On the other hand, the FDR infusion is burdened by increased haematological toxicity. The primary aim of this study was to evaluate the pharmacokinetics of dFdC and its metabolite difluorodeoxyuridine (dFdU) in patients with normal and impaired hepatic function.
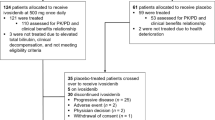
Patients and methods: In this prospective study, patients with pancreatic or biliary tract carcinoma and normal or impaired hepatic function tests were considered eligible for recruitment. Patients were recruited according to the following criteria: (i) serum bilirubin <1.6 mg/dL and AST and ALT <2 times the upper the limit of normal (ULN) [cohort I]; and (ii) serum bilirubin >1.6 mg/dL and/or AST/ALT >2 times the ULN (cohort II). An FDR infusion of gemcitabine 1000 mg/m2 was administered on days 1, 8 and 15 every 4 weeks. The pharmacokinetic analysis of gemcitabine and dFdU was performed with high-performance liquid chromatography-tandem mass spectrometry assay in cycles 1 and 2.
Results: Thirteen patients were enrolled, four in cohort I and nine in cohort II. All patients were assessable for toxicity and pharmacokinetic analysis. The grade and rate of toxicities were similar in both groups, and patients with elevation of bilirubin and/or transaminases did not require dose reduction of gemcitabine. Pharmacokinetic analysis revealed a reduction of the experimental area under the plasma concentration-time curve for gemcitabine and dFdU in patients with hepatic dysfunction when compared with patients with normal hepatic function. All other pharmacokinetic parameters were similar in the two cohorts. No statistical difference was demonstrated for all parameters evaluated between cycle 1 and cycle 2 in the two groups.
Conclusion: Gemcitabine 1000 mg/m2 can be administered as an FDR infusion in patients with altered hepatic function without causing additional toxicity compared with patients with normal hepatic function.













Similar content being viewed by others


References
Stadler WM, Kuzel T, Roth B, et al. Phase II study of single-agent gemcitabine in previously untreated patients with metastatic urothelial cancer. J Clin Oncol 1997; 15: 3394–8
Moore MJ, Tannock IF, Ernst DS, et al. Gemcitabine: a promising new agent in the treatment of advanced urothelial cancer. J Clin Oncol 1997; 15: 3441–5
Heinemann V, Hertel LW, Grindey GB, et al. Comparison of the cellular pharmacokinetics and toxicity of 2′,2′-diflurodeoxycitidine and 1b-D-arabinofuranosylcytosine. Cancer Res 1988; 48: 4024–31
Grunewald R, Kantarjian H, Keating MJ, et al. Pharmacologically directed design of the dose rate and schedule of 2,2-difluorodeoxycytidine administration in leukaemia. Cancer Res 1990; 50: 6823–6
Abbruzzese JL, Grunewald R, Weeks EA, et al. A phase I clinical, plasma and cellular pharmacology study of gemcitabine. J Clin Oncol 1991; 9: 491–8
Heinemann V, Xu YZ, Chubb S, et al. Inhibition of ribonucleotide reduction in CCRF-CEM cells by 2,2-difluorodeoxycytidine. Mol Pharmacol 1990; 38: 567–72
Gandhi V. Questions about gemcitabine dose rate: answered or unanswered? J Clin Oncol 2007; 25(36): 5691–4
Grunewald R, Abbruzzese JL, Tarassoff P, et al. Saturation of 2′, 2′-difluorodeoxycytidine 5′-triphosphate accumulation by mononuclear cells during a phase I trial of gemcitabine. Cancer Chemother Pharmacol 1991; 27: 258–62
Grunewald R, Kantarjian H, Du M, et al. Gemcitabine in leukaemia: a phase I clinical, plasma, and cellular pharmacology study of gemcitabine. J Clin Oncol 1991; 9: 491–8
Patel SR, Gandhi V, Jenkins J, et al. Phase II clinical investigation of gemcitabine in advanced soft tissue sarcomas and window evaluation of dose rate on gemcitabine triphosphate accumulation. J Clin Oncol 2001; 19: 3483–9
Brand R, Capadano M, Tempero M. A phase I trial of weekly gemcitabine administered as a prolonged infusion in patients with pancreatic cancer and other solid tumors. Invest New Drugs 1997; 15: 331–41
Grunewald R, Kantarjian H, Du M, et al. Gemcitabine in leukemia: a phase I clinical, plasma, and cellular pharmacology study. J Clin Oncol 1992; 10:406–13
Tempero M, Plunkett W, Ruiz Van Haperen V, et al. Randomized phase II comparison of dose intense gemcitabine: thirty minute infusion and fixed dose rate infusion in patients with pancreatic adenocarcinoma. J Clin Oncol 2003; 21: 3402–8
Grimison P, Galettis P, Manners S, et al. Randomized crossover study evaluating the effect of gemcitabine infusion rate: evidence of autoinduction of gemcitabine accumulation. J Clin Oncol 2007; 25(36): 5704–9
Venook A, Egorin MJ, Rosner G, et al. Phase I and pharmacokinetic trial of gemcitabine in patients with hepatic or renal dysfunction: Cancer and Leukemia Group B 9565. J Clin Oncol 2000; 18: 2780–7
Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst 2000; 92(3): 205–16
Sottani C, Massimo Zucchetti M, Zaffaroni M, et al. Validated procedure for simultaneous trace level determination of the anti-cancer agent gemcitabine and its metabolite in human urine by high-performance liquid chromatography with tandem mass spectrometry. Rapid Commun Mass Spectrom 2004; 18: 1017–23
Fogli S, Danesi R, Gennai A, et al. Gemcitabine, epirubicin and paclitaxel: pharmacokinetic and pharmacodynamic interactions in advanced breast cancer. Ann Oncol 2002; 13(6): 919–27
Sessa C, Aamdal S, Wolff I, et al. Gemcitabine in patients with advanced malignant melanoma or gastric cancer: phase II studies of the EORTC Early Clinical Trials Group. Ann Oncol 1994; 5: 471–2
Gelibter A, Malaguti P, Di Cosimo S, et al. Fixed dose-rate gemcitabine infusion as first-line treatment for advanced-stage carcinoma of the pancreas and biliary tree. Cancer 2005; 104(6): 1237–45
Fossella FV, Lippman SM, Shin DM, et al. Maximum-tolerated dose defined for single-agent gemcitabine: a phase I dose-escalation study in chemotherapy-naive patients with advanced non-small-cell-lung cancer. J Clin Oncol 1997; 15: 310–6
Soo RA, Wang LZ, Tham LA, et al. A multicenter randomized phase II study of carboplatin I combination with gemcitabine at standard rate or fixed dose rate infusion in patients with advanced stage non-small cell lung cancer. Ann Oncol 2006; 17(7): 1128–33
Acknowledgements
This study was supported by grants from the Italian Ministry of Health. The authors have no conflicts of interest that are directly relevant to the content of this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Felici, A., Di Segni, S., Milella, M. et al. Pharmacokinetics of Gemcitabine at Fixed-Dose Rate Infusion in Patients with Normal and Impaired Hepatic Function. Clin Pharmacokinet 48, 131–141 (2009). https://doi.org/10.2165/00003088-200948020-00005
Published:
Issue Date:
DOI: https://doi.org/10.2165/00003088-200948020-00005