
Summary
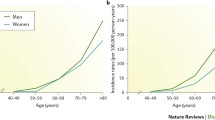
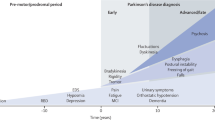
Parkinson’s disease (PD) is the second most common neurodegenerative disorder worldwide and is characterised by cardinal clinical features and specific pathological findings. It is possible to detect PD early on in the course of the disease, and certain laboratory studies may identify preclinical stages. Based on this information, and the hypothesis that there is a long preclinical period, there appears to be a window of opportunity to influence the natural course of the disease.
Postulates regarding pathogenesis, such as oxidative stress and excitotoxicity, have led to the discovery of abnormal mitochondrial function in PD and a search for biochemical markers. Functional imaging studies have detected subclinical nigral dopaminergic dysfunction in individuals at risk of developing PD.
Current symptomatic therapies are aimed at enhancing dopaminergic transmission. However, some commonly used PD medications may have alternative actions with both symptomatic and neuroprotective consequences. Bromocriptine has been postulated to have antioxidant effects and amantadine to have N-methyl-D-aspartate (NMDA) receptor antagonistic properties. Both have been reported to be associated with improved survival in PD. Additionally, monoamine oxidase type B inhibitors may provide neuroprotection.
Recent new medications are also under study with regard to neuroprotection. Despite these advances, until there is a better understanding of the aetiology and pathogenesis of PD, there will be no definitive long-term benefit of early diagnosis and treatment of PD.
Similar content being viewed by others

References
Kurland LT. Epidemiology: incidence, geographic distribution and genetic considerations. In: Fields WS, editor. Pathogenesis and treatment of parkinsonism. Springfield: Charles C. Thomas, 1985: 5–43
Stern G. Clinical diagnosis in early stages of Parkinson’s disease [abstract]. Second Congress of the European Society for Clinical Neuropharmacology. J Neural Transm 1995; 102: XLIV
Bernheimer H, Birkmayer W, Hornykiewicz O, et al. Brain dopamine and the syndromes of Parkinson and Huntington: clinical, morphological, and neurochemical correlations. J Neurol Sci 1973; 20: 415–55
Rajput AH, Rozdilsky B, Rajput A. Accuracy of clinical diagnosis in parkinsonism — a prospective study. Can J Neurol Sci 1991; 18: 275–8
Hughes AJ, Ben-Schlomo Y, Daniel SE. What features improve the accuracy of clinical diagnosis in Parkinson’s disease: a clinicopathologic study. Neurology 1992; 42: 1142–6
Calne DB, Snow BJ, Lee C. Criteria for diagnosing Parkinson’s disease. Ann Neurol 1992; 32: S125–7
Koller WC, Langston JW, Hubble JP, et al. Does a long preclinical period occur in Parkinson’s disease? Neurology 1991; 41Suppl. 2: 8–13
Langston JW, Koller WC. The next frontier in Parkinson’s disease: presymptomatic detection. Neurology 1991; 41Suppl. 2: 5–7
Lees AJ. When did Ray Kennedy’s Parkinson’s disease begin? Mov Disord 1991; 7: 110–6
Przuntek H. Early diagnosis in Parkinson’s disease. J Neural Transm 1992; 38 Suppl.: 105–14
Tetrud JW. Preclinical Parkinson’s disease: detection of motor and nonmotor manifestations. Neurology 1991; 41Suppl. 2: 69–72
Hawkes CM. Diagnosis and treatment of Parkinson’s disease: anosmia is a common finding [letter]. BMJ 1995; 310: 1668
Doty RL, Deems DA, Stellar S. Olfactory dysfunction in parkinsonism: a general deficit unrelated to neurologic signs, disease stage, or disease duration. Neurology 1988; 38: 1237–44
Bonuccelli U, Maremmani C, Del Dotto P, et al. Olfactory deficits in Parkinson’s disease [abstract]. Neurology 1992; 42Suppl. 3: 440
Doty RL, Shaman P, Kimmelman CP, et al. University of Pennsylvania Smell Identification Test: a rapid quantitative olfactory function test for the clinic. Laryngoscope 1984; 94: 176–8
Wenning GK, Shephard B, Hawkes C, et al. Olfactory function in atypical parkinsonian syndromes. Acta Neurol Scand 1995; 91: 247–50
Doty RL, Golbe LI, McKeown DA, et al. Olfactory testing differentiates between progressive supranuclear palsy and idiopathic Parkinson’s disease. Neurology 1993; 43: 962–5
Busenbark KL, Huber SJ, Greer G, et al. Olfactory function in essential tremor. Neurology 1992; 42: 1631–2
Hawkes CH, Shephard BC. Olfactory impairment in Parkinson’s disease: evidence of dysfunction measured by olfactory-evoked potentials and smell identification tests [abstract]. Ann Neurol 1992; 32: 248
Watts RL, Mandir AS, Ahn KJ, et al. Electrophysiologic analysis of early Parkinson’s disease. Neurology 1991; 41Suppl. 2: 44–8
Bergui M, Paglia G, Lopiano L, et al. Early modification of stretch reflex in Parkinson’s disease. Acta Neurol Scand 1993; 88: 16–20
Uitti RJ, Calne DB. Pathogenesis of idiopathic parkinsonism. Eur Neurol 1993; 33Suppl. 1: 6–23
Dexter DT, Carter CJ, Wells FR, et al. Basal lipid peroxidation in substantia nigra is increased in Parkinson’s disease. J Neurochem 1989; 52: 381–9
Shoulson I. Experimental therapeutics directed at the pathogenesis of Parkinson’s disease. In: Calne DB, editor. Drugs for the treatment of Parkinson’s disease. New York: Springer-Verlag, 1988: 289–305
Spina MB, Cohen G. Dopamine turnover and glutathione oxidation: implications for Parkinson’s disease. Proc Natl Acad Sci US A 1989; 86: 1398–400
Gotz ME, Freyberger A, Riederer P. Oxidative stress: a role in the pathogenesis of Parkinson’s disease. J Neural Transm 1990; 24: 241–9
Lange KW, Loschmann PA, Sotic E, et al. The competitive NMDA antagonist CPP protects substantia nigra neurons from MPTP-induced neurodegeneration in primates [abstract]. Mov Disord 1992; 7: 293
Turski L, Bressler K, Rettig K, et al. Protection of substantia nigra from MPP+ neurotoxicity by N-methyl-D-aspartate antagonists. Nature 1991; 349: 414–8
Gibson CJ, Logue M, Growdon JH. CSF monoamine metabolite levels in Alzheimer’s and Parkinson’s disease. Arch Neurol 1985; 42: 489–92
Parkinson Study Group. Cerebrospinal fluid homovanillic acid in the DATATOP study on Parkinson’s disease. Arch Neurol 1995; 52: 237–45
Carlsson A, Fornstedt B. Catechol metabolites in the cerebrospinal fluid as possible markers in the early diagnosis of Parkinson’s disease. Neurology 1991; 41Suppl. 2: 50–1
Williams A, Steventon G, Sturman S, et al. Xenobiotic enzyme profiles and Parkinson’s disease. Neurology 1991; 41Suppl. 2: 29–32
Heafield MTE, Fern S, Steventon GB, et al. Plasma cysteine and sulfate levels in patients with motor neurone, Parkinson’s and Alzheimer’s disease. Neurosci Lett 1990; 110: 216–20
Langston JW, Ballard P, Tetrud JW, et al. Chronic parkinsonism in humans due to a product of meperidine synthesis. Science 1983; 219: 979–80
Langston JW, Irwin I, Langston EB, et al. l-Methyl-4-phenylpyridinium ion (MPP+): identification of a metabolite of MPTP, a toxin selective to the substantia nigra. Neurosci Lett 1984; 48: 87–92
Markey SP, Johannessen JN, Chiueh CC, et al. Intraneuronal generation of a pyridinium metabolite may cause drug-induced parkinsonism. Nature 1984; 311: 464–7
Nicklas WJ, Vyas I, Heikkila RE. Inhibition of NADH-linked oxidation in brain mitochondria by l-methyl-4-phenylpyridine, a metabolite of the neurotoxin, l-methyl-4-phenyl-1,2,3,6-tetrahydropyridine. Life Sci 1985; 36: 2503–8
Di Monte DA. Mitochondrial DNA and Parkinson’s disease. Neurology 1991; 41Suppl. 2: 38–42
Rajput AH, Uitti RJ, Stern W, et al. Geography, drinking water chemistry, pesticides and herbicides and the etiology of Parkinson’s disease. Can J Neurol Sci 1987; 14: 414–8
Di Monte DA, Chan P, Sandy MS. Glutathione in Parkinson’s disease: a link between oxidative stress and mitochondrial damage? Ann Neurol 1992; 32 Suppl.: S111–5
Parker Jr WD, Boyson SJ, Parks JK. Abnormalities of the electron transport chain in idiopathic Parkinson’s disease. Ann Neurol 1989; 26: 719–23
Benecke R, Strumper P, Weiss H. Electron transport complexes I and IV of platelets are abnormal in Parkinson’s disease but normal in Parkinson-plus syndromes. Brain 1993; 116: 1451–63
Shoffner JM, Watts RL, Juncos JL, et al. Mitochondrial oxidative phosphorylation defects in Parkinson’s disease. Ann Neurol 1991; 30: 332–9
Schapira AHV, Mann VM, Cooper JM, et al. Anatomic and disease specificity of NADH CoQ reductase (complex I) deficiency in Parkinson’s disease. J Neurochem 1990; 55: 2142–5
Ikebe S, Tanaka M, Ohno K, et al. Increase of deleted mitochondrial DNA in the striatum in Parkinson’s disease and senescence. Biochem Biophys Res Commun 1990; 170: 1044–8
Shapira AHV, Holt IJ, Sweeney M, et al. Mitochondrial DNA analysis in Parkinson’s disease. Mov Disord 1990; 5: 294–7
Sandy MS, Langston JW, Smith MT, et al. PCR analysis of platelet mtDNA: lack of specific changes in Parkinson’s disease. Mov Disord 1993; 8: 74–82
DiDonato S, Zeviani M, Giovannini P, et al. Respiratory chain and mitochondrial DNA in muscle and brain in Parkinson’s disease patients. Neurology 1993; 43: 2262–8
Brooks J, Ibanez V, Sawle GV, et al. Differing patterns of striatal 18F-dopa uptake in Parkinson’s disease, multiple system atrophy, and progressive supranuclear palsy. Ann Neurol 1990; 28: 547–55
Garnett ES, Nahmias C, Firnau G. Central dopaminergic pathways in hemiparkinsonism examined by positron emission tomography. Can J Neurol Sci 1984; 11Suppl. 1: 174–9
German DC, Manaye K, Smith WK, et al. Midbrain dopaminergic cell loss in Parkinson’s disease: computer visualization. Ann Neurol 1989; 26: 507–14
Leenders KL, Salmon EP, Tyrrell P, et al. The nigrostriatal dopaminergic system assessed in vivo by positron emission tomography in healthy volunteer subjects and patients with Parkinson’s disease. Arch Neurol 1990; 47: 1290–8
Calne DB, Langston JW, Martin WRW, et al. Positron emission tomography after MPTP: observations relating to the cause of Parkinson’s disease. Nature 1985; 317: 246–8
Vingerhoets FJG, Snow BJ, Tetrud JW, et al. Positron emission tomographic evidence for progression of human MPTP-induced dopaminergic lesions. Ann Neurol 1994; 36: 765–70
Vingerhoets FJG, Snow BJ, Lee CS, et al. Longitudinal fluorodopa positron emission tomographic studies of the evolution of idiopathic parkinsonism. Ann Neurol 1994; 36: 759–64
Sawle GV, Wroe SJ, Lees AJ, et al. The identification of presymptomatic parkinsonism: Clinical and 18Fdopa positron emission tomography studies in an Irish kindred. Ann Neurol 1992; 32: 609–17
Burn DJ, Mark MH, Playford ED, et al. Parkinson’s disease in twins studied with 18F-dopa and positron emission tomography. Neurology 1992; 42: 1894–900
Schwarz J, Tatsch K, Arnold G, et al. 123I-Iodobenzamide-SPECT in 83 patients with de novo parkinsonism. Neurology 1993; 43Suppl. 6: S17–20
Bergstrom KA, Kuikka JT, Ahonen A, et al. [1231] β-CIT, a tracer for dopamine and serotonin re-uptake sites: preparation and preliminary SPECT studies in humans. J Nucl Biol Med 1994; 38 (4 Suppl. 1): 128–31
Brucke T, Kornhuber J, Angelberger P, et al. SPECT imaging of dopamine and serotonin transporters with [123I]beta-CIT: binding kinetics in the human brain. J Neural Transm Gen Sect 1993; 94: 137–46
Marsden CD, Parkes JD. Success and problems of long-term levodopa therapy in Parkinson’s disease. Lancet 1977; I: 345–9
Uitti RJ, Ahlskog JE, Maraganore DM, et al. Levodopa therapy and survival in idiopathic Parkinson’s disease: Olmstead County project. Neurology 1993; 43: 1918–26
Diamond SG, Markham CH, Hoehn MM, et al. Multi-center study of Parkinson mortality with early versus later dopa treatment. Ann Neurol 1987; 22: 8–12
McDermott MP, Jankovic J, Carter J, et al. Factors predictive of the need for levodopa therapy in early, untreated Parkinson’s disease. Arch Neurol 1995; 52: 565–70
Przedborski S, Jackson-Lewis V, Muthane U, et al. Chronic levodopa administration alters cerebral mitochondrial respiratory chain activity. Ann Neurol 1993; 34: 715–23
Grimes JD, Hassan MN. Evidence to support the simultaneous initiation of dopamine agonist and levodopa therapy in the management of de novo patients with Parkinson’s disease [abstract]. Arch Neurol 1988; 45: 206
Cedarbaum JM, Gandy SE, McDowell FH. ‘Early’ initiation of levodopa treatment does not promote the development of motor response fluctuations, dyskinesias, or dementia in Parkinson’s disease. Neurology 1991; 41: 622–9
Caraceni T, Scigliano G, Musicco M. The occurrence of motor fluctuations in parkinsonian patients treated long term with levodopa: role of early treatment and disease progression. Neurology 1991; 41: 380–4
Factor SA, Weiner WJ. Early combination therapy with bromocriptine and levodopa in Parkinson’s disease. Mov Disord 1993; 8: 257–62
Rinne UK. Early combination of bromocriptine and levodopa in the treatment of Parkinson’s disease: a 5-year follow-up. Neurology 1987; 37: 826–8
Przuntek H, Welzel D, Blumner E, et al. Bromocriptine lessens the incidence of mortality in L-dopa-treated Parkinsonian patients: Prado study discontinued. Eur J Clin Pharmacol 1992; 43: 357–63
Factor SA, Weiner WJ. Early combination therapy with bromocriptine and levodopa in Parkinson’s disease. Mov Disord 1993; 8: 257–62
Hely MA, Morris JG, Reid WG, et al. The Sydney multicenter study of Parkinson’s disease: a randomised, prospective five year study comparing low dose bromocriptine with low dose levodopa-carbidopa. J Neurol Neurosurg Psychiatry 1994; 57: 903–10
Ahlskog JE, Muenter MD. Treatment of Parkinson’s disease with pergolide: a double-blind study. Mayo Clin Proc 1988; 63: 969–78
Stoof JC, Booij J, Drukarch B. Amantadine as N-methyl-D-as-partic acid receptor antagonist: new possibilities for therapeutic applications. Clin Neurol Neurosurg 1992; 94 Suppl.: S4–6
Jackisch R, Link T, Neufang B, et al. Studies on the mechanism of action of the antiparkinsonian drugs memantine and amantadine: no evidence for direct dopaminomimetic or anti-muscarinic properties. Arch Int Pharm 1992; 320: 21–42
Greenamyre JT, O’Brien CF. N-methyl-D-aspartate antagonists in the treatment of Parkinson’s disease. Arch Neurol 1991; 48: 977–81
Uitti RJ, Rajput AH, Ahlskog JE, et al. Amantadine treatment is an independent predictor of improved survival in Parkinson’s disease. Neurology 1996; 46: 1551–6
Halliwell B, Gutteridge JMC. Oxygen radicals and the nervous system. Trends Neurosci 1985; 8: 22–6
Parkinson Study Group. The effects of tocopherol and deprenyl on the progression of disability in early Parkinson’s disease. N Engl J Med 1993; 328: 176–83
Glover V, Sandler M, Owen F, et al. Dopamine is a monoamine B substrate in man. Nature 1977; 265: 80–1
Cohen G, Pasik P, Cohen B, et al. Pargyline and deprenyl prevent the neurotoxicity of 1-methyl-4-pheny 1-1,2,3,6-tetrahydropyridine (MPTP) in monkeys. Eur J Pharmacol 1985; 106: 209–10
Heikkila RE, Manzino L, Cabbats FS, et al. Protection against the dopaminergic neurotoxicity of l-methyl-4-phenyl-1,2,3,6-tetrahydropyridine by monoamine oxidase inhibitors. Nature 1984; 311: 467–9
Cohen G, Spina MB. Deprenyl suppresses the oxidant stress associated with increased dopamine turnover. Ann Neurol 1989; 26: 689–90
Tatton WG. Selegiline can mediate neuronal rescue rather than neuronal protection. Mov Disord 1993; 8Suppl. 1: S20–30
Schulzer M, Mak E, Calne DB. The antiparkinsonian efficacy of deprenyl derives from transient improvement that is likely to be symptomatic. Ann Neurol 1992; 32: 795–8
Parkinson Study Group. Impact of deprenyl and tocopherol treatment on Parkinson’s disease in DATATOP subjects not requiring levodopa. Ann Neurol 1996; 39: 29–36
Olanow CW, Calne D. Does selegiline monotherapy in Parkinson’s disease act by symptomatic or protective mechanisms? Neurology 1991; 42: 13–26
Karoum F, Chuang LW, Eisler T, et al. Metabolism of (−) deprenyl to amphetamine and methamphetamine may be responsible for deprenyl’s therapeutic benefit: a biochemical assessment. Neurology 1982; 32: 503–9
Shults CW. Future perfect? Presymptomatic diagnosis, neural transplantation, and trophic factors. Neurol Clin 1992; 10: 567–93
Parkinson Study Group. A controlled trial of lazabemide (RO19-6327) in untreated Parkinson’s disease. Ann Neurol 1993; 33: 350–6
Fowler JS, Volkow ND, Logan J, et al. Monoamine oxidase B (MAO B) inhibitor therapy in Parkinson’s disease: the degree and reversibility of human brain MAO B inhibition by Ro 19 6327. Neurology 1993; 43: 1984–92
Henriot S, Kuhn C, Kettler R, et al. Lazabemide (RO 19-6327), a reversible and highly sensitive MAO-B inhibitor: preclinical and clinical findings. J Neural Transm 1994; 41 Suppl.: 321–5
Greenamyre JT, Eller RV, Zhang Z, et al. Antiparkinsonian effects of remacemide hydrochloride, a glutamate antagonist, in rodent and primate models of Parkinson’s disease. Ann Neurol 1994; 35: 655–61
Hyman C, Hofer M, Barde YA, et al. BDNF is a neurotrophic factor for dopaminergic neurons of the substantia nigra. Nature 1991; 350: 230–2
Date I, Yoshimoto Y, Imaoka T, et al. Enhanced recovery of the nigrostriatal dopaminergic system in MPTP-treated mice following intrastriatal injection of basic fibroblast growth factor in relation to aging. Brain Res 1993; 621: 150–4
Ventrella LLE. Effect of intracerebroventricular infusion of epidermal growth factor in rats hemitransected in the nigro-striatal pathway. J Neurol Sci 1993; 37: 1–8
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Di Paola, R., Uitti, R.J. Early Detection of Parkinson’s Disease. Drugs & Aging 9, 159–168 (1996). https://doi.org/10.2165/00002512-199609030-00002
Published:
Issue Date:
DOI: https://doi.org/10.2165/00002512-199609030-00002