
Abstract
Background: Newly approved drugs, in comparison with older drugs, are more often prescribed to patients who have not responded satisfactorily to established related drugs or as first-line therapy to patients with a high baseline risk for adverse outcomes (i.e. channelling). However, these patients are less likely to benefit from the prescribed drug and/or are more prone to adverse drug reactions. Therefore, it is difficult to unravel whether observed risks or increases in risk of new drugs are real, i.e. related to the pharmacology, or whether these are related to selective prescribing to patients who are more susceptible to adverse events because of some underlying risk factor(s). The channelling paradox may exist for cyclo-oxygenase (COX)-2 selective inhibitors (‘coxibs’) instead of traditional nonselective NSAIDs in relation to both gastrointestinal (GI) and cardiovascular (CV) safety.
Objective: To evaluate the risk profiles for GI and CV adverse effects in nonselective NSAID and coxib new-user populations over time, in terms of a quantitative measure since the introduction of coxibs.
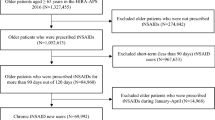
Methods: This was a population-based cohort study using the Dutch pharmaceutical claims database (Foundation for Pharmaceutical Statistics). Eligible patients (≥18 years) were those where the date of their first prescription (index date) of an NSAID (first-line [e.g. ibuprofen] or second-line [e.g. piroxicam] nonselective NSAID, COX-2 preferential NSAID or coxib) was between January 1999 and December 2003. For each patient, GI and CV risk profiles at index date were defined by a cumulative score derived from dispensing data (patient age, sex and history of medication use within 6 months of index date). Risk scores were categorized as low (score = 0), medium (1) or high (2+). Patients were recorded as switchers based on other NSAID use prior to the index date. Other information collected included the Chronic Disease Score (CDS). Crude odds ratios (ORs) were calculated for risk factors for each NSAID group versus first-line nonselective NSAID users as the reference cohort. The effect of calendar time was examined by plotting mean CV or GI risk score by quarter-year. Correlation between GI and CV scores was examined using the Pearson correlation coefficient (R). Data were stratified by patients’ history of switching.
Results: The four cohorts comprised patients using: first-line nonselective NSAIDs (n = 42 750); second-line nonselective NSAIDs (n = 1771); COX-2 preferential NSAIDs (n = 3661) and coxibs (n = 4861) patients. New coxib users were most likely to have high GI and CV risk scores (OR 5.3 [95% CI 5.0, 5.6] and OR 2.2 [95% CI 2.1, 2.4], respectively). At the individual patient level, GI and CV risk profiles were moderately well correlated for all NSAID cohorts (R range 0.48 to 0.62). There was no remarkable change in mean GI or CV risk profile of patients over calendar time since the market introduction of coxibs.
Discussion: Of the four NSAID cohorts, new coxib users tended to have the highest numbers of GI and CV risk factors, with no obvious change over calendar time. There was also evidence of correlation between GI and CV risk scores. Thus, selective prescribing of coxibs applies to people with co-existing CV as well as GI risk factors. This is important when comparing the safety and/or efficacy of new therapies to existing therapies, and emphasizes the difficulties encountered by prescribers in assessing levels of risk when initiating coxib treatment.








Similar content being viewed by others

Notes
1The licence was extended for rofecoxib to include treatment of rheumatoid arthritis in December 2001.
References
Petri H, Urquhart J. Channeling bias in the interpretation of drug effects. Stat Med 1991 Apr; 10(4): 577–81
Sift R, van Staa TP, Abenhaim L, et al. A study of the longitudinal utilization and switching-patterns of non-steroidal anti-inflammatory drugs using a pharmacy based approach. Pharmacoepidemiol Drug Saf 1997 Jul; 6(4): 263–8
Leufkens HG, Urquhart J, Stricker BH, et al. Channelling of controlled release formulation of ketoprofen (Oscorel) in patients with history of gastrointestinal problems. J Epidemiol Community Health 1992 Aug; 46(4): 428–32
Martin RM, Biswas P, Mann RD. The incidence of adverse events and risk factors for upper gastrointestinal disorders associated with meloxicam use amongst 19,087 patients in general practice in England: cohort study. Br J Clin Pharmacol 2000 Jul; 50(1): 35–42
MacDonald TM, Morant SV, Goldstein JL, et al. Channelling bias and the incidence of gastrointestinal haemorrhage in users of meloxicam, coxibs, and older, non-specific non-steroidal anti-inflammatory drugs. Gut 2003 Sep; 52(9): 1265–70
Movig KL, Egberts AC, Lenderink AW, et al. Selective prescribing of spasmolytics. Ann Pharmacother 2000 Jun; 34(6): 716–20
Egberts AC, Lenderink AW, de Koning FH, et al. Channeling of three newly introduced antidepressants to patients not responding satisfactorily to previous treatment. J Clin Psychopharmacol 1997 Jun; 17(3): 149–55
Inman WH. Non-steroidal anti-inflammatory drugs: assessment of risks. Eur J Rheumatol Inflamm 1987; 8(1): 71–85
FitzGerald GA, Patrono C. The coxibs, selective inhibitors of cyclooxygenase-2. N Engl J Med 2001 Aug 9; 345(6): 433–42
Florentinus SR, Heerdink ER, de BA, et al. The trade-off between cardiovascular and gastrointestinal effects of rofecoxib. Pharmacoepidemiol Drug Saf 2005 Jul; 14(7): 437–41
Girvin B, Rafferty T, Stevenson MR, et al. Uptake of COX-2 selective inhibitors and influence on NSAID prescribing in Northern Ireland. Pharmacoepidemiol Drug Saf 2004 Mar; 13(3): 153–7
Laporte JR, Ibanez L, Vidal X, et al. Upper gastrointestinal bleeding associated with the use of NSAIDs: newer versus older agents. Drug Saf 2004; 27(6): 411–20
Hippisley-Cox J, Coupland C, Logan R. Risk of adverse gastrointestinal outcomes in patients taking cyclo-oxygenase-2 inhibitors or conventional non-steroidal anti-inflammatory drugs: population based nested case-control analysis. BMJ 2005 Dec 3; 331(7528): 1310–6
Bombardier C, Laine L, Reicin A, et al. Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. VIGOR Study Group. N Engl J Med 2000 Nov 23; 343(21): 1520–8, 2
Grosser T, Fries S, FitzGerald GA. Biological basis for the cardiovascular consequences of COX-2 inhibition: therapeutic challenges and opportunities. J Clin Invest 2006 Jan; 116(1): 4–15
Aw TJ, Haas SJ, Liew D, et al. Meta-analysis of cyclooxygenase-2 inhibitors and their effects on blood pressure. Arch Intern Med 2005 Mar 14; 165(5): 490–6
Hernandez-Diaz S, Rodriguez LA. Incidence of serious upper gastrointestinal bleeding/perforation in the general population: review of epidemiologic studies. J Clin Epidemiol 2002 Feb; 55(2): 157–63
Hernandez-Diaz S, Varas-Lorenzo C, Garcia Rodriguez LA. Non-steroidal antiinflammatory drugs and the risk of acute myocardial infarction. Basic Clin Pharmacol Toxicol 2006 Mar; 98(3): 266–74
Zhao SZ, Wentworth C, Burke TA, et al. Drug switching patterns among patients with rheumatoid arthritis and osteoar-thritis using COX-2 specific inhibitors and non-specific NSAIDs. Pharmacoepidemiol Drug Saf 2004 May; 13(5): 277–87
Dai C, Stafford RS, Alexander GC. National trends in cyclooxy-genase-2 inhibitor use since market release: nonselective diffusion of a selectively cost-effective innovation. Arch Intern Med 2005 Jan 24; 165(2): 171–7
Helin-Salmivaara A, Huupponen R, Virtanen A, et al. Frequent prescribing of drugs with potential gastrointestinal toxicity among continuous users of non-steroidal anti-inflammatory drugs. Eur J Clin Pharmacol 2005 Jul; 61(5–6): 425–31
Moride Y, Ducruet T, Boivin JF, et al. Prescription channeling of COX-2 inhibitors and traditional nonselective nonsteroidal anti-inflammatory drugs: a population-based case-control study. Arthritis Res Ther 2005; 7(2): R333–42
Norgard B, Pedersen L, Johnsen SP, et al. COX-2-selective inhibitors and the risk of upper gastrointestinal bleeding in high-risk patients with previous gastrointestinal diseases: a population-based case-control study. Aliment Pharmacol Ther 2004 Apr 1; 19(7): 817–25
Joshua FF, Oakley SP, Major GA. Impact of selective cyclooxy-genase-2 inhibitors on anti-ulcer medication and non-steroidal anti-inflammatory drug use in patients with rheumatic disease. Intern Med J 2004 Apr; 34(4): 153–61
Mosis G, Stijnen T, Castellsague J, et al. Channeling and prevalence of cardiovascular contraindications in users of cyclooxygenase 2 selective nonsteroidal antiinflammatory drugs. Arthritis Rheum 2006 Aug 15; 55(4): 537–42
Florentinus SR, Souverein PC, Griens FA, et al. Linking community pharmacy dispensing data to prescribing data of general practitioners. BMC Med Inform Decis Mak 2006; 6: 18
Garcia Rodriguez LA, Cattaruzzi C, Troncon MG, et al. Risk of hospitalization for upper gastrointestinal tract bleeding associated with ketorolac, other nonsteroidal anti-inflammatory drugs, calcium antagonists, and other antihypertensive drugs. Arch Intern Med 1998 Jan 12; 158(1): 33–9
Eccles M, Freemantle N, Mason J. North of England evidence based guideline development project: summary guideline for non-steroidal anti-inflammatory drugs versus basic analgesia in treating the pain of degenerative arthritis. The North of England Non-Steroidal Anti-Inflammatory Drug Guideline Development Group. BMJ 1998 Aug 22; 317(7157): 526–30
Laine L. Approaches to nonsteroidal anti-inflammatory drug use in the high-risk patient. Gastroenterology 2001 Feb; 120(3): 594–606
Hernandez-Diaz S, Garcia Rodriguez LA. Cardioprotective aspirin users and their excess risk of upper gastrointestinal complications. BMC Med 2006; 4: 22
de Abajo FJ, Rodriguez LA, Montero D. Association between selective serotonin reuptake inhibitors and upper gastrointestinal bleeding: population based case-control study. BMJ 1999 Oct 23; 319(7217): 1106–9
Von-Korff M, Wagner EH, Saunders K. A chronic disease score from automated pharmacy data. J Clin Epidemiol 1992 Feb; 45(2): 197–203
Clark DO, Von Korff M, Saunders K, et al. A chronic disease score with empirically derived weights. Med Care 2005 Aug 1; 8: 783–98
Arellano FM, Yood MU, Wentworth CE, et al. Use of cyclooxygenase 2 inhibitors (COX-2) and prescription non-steroidal anti-inflammatory drugs (NSAIDS) in UK and USA populations. Implications for COX-2 cardiovascular profile. Pharmacoepidemiol Drug Saf 2006 Dec; 15(12): 861–72
Layton D, Riley J, Wilton LW, et al. Safety profile of rofecoxib as used in general practice in England: results of a prescription-event monitoring study. Br J Clin Pharmacol 2002; 55: 166–74
Layton D, Wilton LV, Shakir SA. Safety profile of celecoxib as used in general practice in England: results of a prescription-event monitoring study. Eur J Clin Pharmacol 2004 Sep; 60(7): 489–501
Langman M, Kahler KH, Kong SX, et al. Drug switching patterns among patients taking non-steroidal anti-inflammatory drugs: a retrospective cohort study of a general practitioners database in the United Kingdom. Pharmacoepidemiol Drug Saf 2001 Oct; 10(6): 517–24
Kaufman DW, Kelly JP, Rosenberg L, et al. Are cyclooxygenase-2 inhibitors being taken only by those who need them? Arch Intern Med 2005 May 9; 165(9): 1066–7
Rahme E, Hunsche E, Toubouti Y, et al. Retrospective analysis of utilization patterns and cost implications of coxibs among seniors in Quebec, Canada: what is the potential impact of the withdrawal of rofecoxib? Arthritis Rheum 2006 Feb 15; 55(1): 27–34
Solomon DH, Schneeweiss S, Glynn RJ, et al. Determinants of selective cyclooxygenase-2 inhibitor prescribing: are patient or physician characteristics more important? Am J Med 2003 Dec 15; 115(9): 715–20
McGettigan P, Henry D. Cardiovascular risk and inhibition of cyclooxygenase: a systematic review of the observational studies of selective and nonselective inhibitors of cyclooxygenase 2. JAMA 2006 Oct 4; 296(13): 1633–44
Visser LE, Graatsma HH, Stricker BH. Contraindicated NSAIDs are frequently prescribed to elderly patients with peptic ulcer disease. Br J Clin Pharmacol 2002 Feb; 53(2): 183–8
Konstantinopoulos PA, Lehmann DF. The cardiovascular toxicity of selective and nonselective cyclooxygenase inhibitors: comparisons, contrasts, and aspirin confounding. J Clin Pharmacol 2005 Jul; 45(7): 742–50
Singh G, Miller JD, Huse DM, et al. Consequences of increased systolic blood pressure in patients with osteoarthritis and rheumatoid arthritis. J Rheumatol 2003 Apr; 30(4): 714–9
Arellano FM, Zhao SZ, Reynolds MW. Case of cholestatic hepatitis with celecoxib did not fulfil international criteria [letter]. BMJ 2002 Mar 30; 324(7340): 789
McMahon AD. Approaches to combat with confounding by indication in observational studies of intended drug effects. Pharmacoepidemiol Drug Saf 2003 Oct; 12(7): 551–8
Usher C, Bennett K, Teeling M, et al. Characterizing new users of NSAIDs before and after rofecoxib withdrawal. Br J Clin Pharmacol 2006 Oct 19; 63(4): 494–7
Yood MU, Watkins E, Wells K, et al. The impact of NSAID or COX-2 inhibitor use on the initiation of antihypertensive therapy. Pharmacoepidemiol Drug Saf 2006 Dec; 15(12): 852–60
Blot WJ, McLaughlin JK. Over the counter non-steroidal anti-inflammatory drugs and risk of gastrointestinal bleeding. J Epidemiol Biostat 2000; 5(2): 137–42
Scheiman JM, Fendrick AM. NSAIDs without a prescription: over-the-counter access, under-counted risks. Am J Gastroenterol 2002 Sep; 97(9): 2159–61
Bombardier C. An evidence-based evaluation of the gastrointestinal safety of coxibs. Am J Cardiol 2002 Mar 21; 89(6A): 3D–9D
Becker JC, Domschke W, Pohle T. Current approaches to prevent NSAID-induced gastropathy: COX selectivity and beyond. Br J Clin Pharmacol 2004 Dec; 58(6): 587–600
Former H. NHG-Standpunt over de preventie van NSAID-geinduceerde maagproblemen en de plaats van de coxibs in de huisartpraktijk.2004 [online]. Available from URL: http://nhg.artsennet.nl/content/resources/AMGATE_6059_104_TICH_L1297846793/AMGATE_6059_104_TICH_R120544452391946// [Accessed 2007 May 1]
National Institute of Clinical Excellence. Technology Appraisal No. 27. Guidance on use of cyclo-oxygenase (COXII) selective inhibitors celecoxib, rofecoxib, meloxicam and etodoloac for osteoarthritis and rheumatoid arthritis [online]. Available from URL: http://www.nice.org.uk/nicemedia/pdf/coxiifullguidance.pdf [Accessed 2001 Aug 1]
Lanas A, Garcia-Rodriguez LA, Arroyo MT, et al. Risk of upper gastrointestinal ulcer bleeding associated with selective cyclooxygenase-2 inhibitors, traditional non-aspirin non-steroidal anti-inflammatory drugs, aspirin and combinations. Gut 2006 Dec; 55(12): 1731–8
Inman W, Pearce G. Prescriber profile and post-marketing surveillance. Lancet 1993 Sep 11; 342(8872): 658–61
Cleveland Clinic. Cleveland clinic launches large-scale global trial to examine cardiovascular safety of popular pain relievers. 2006 Dec 13 [online]. Available from URL: http://www.clevelandclinic.org/heartcenter/pub/news/archive/2005/painre-lief12_13print.htm. [Accessed 2006 Dec 18]
European Medicines Agency. Public CHMP assessment report for medicinal products containing non-selective non steroidal anti-inflammatory drugs (NSAIDs) [online]. Available from URL: http://www.emea.europa.eu/pdfs/human/opiniongen/44213006en.pdf. [Accessed 2007 Feb 12]
Acknowledgements
The Drug Safety Research Unit (DSRU) is an independent charity that works in association with the University of Portsmouth, UK. It receives unconditional donations (unrelated to this article) from pharmaceutical companies including the manufacturers of COX-2 inhibitors and NSAIDs. The companies have no control on the conduct or the publication of the studies conducted by the DSRU.
The authors from the Utrecht Institute for Pharmaceutical Sciences, The Netherlands, have no conflict of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Layton, D., Souverein, P.C., Heerdink, E.R. et al. Evaluation of Risk Profiles for Gastrointestinal and Cardiovascular Adverse Effects in Nonselective NSAID and COX-2 Inhibitor Users. Drug-Safety 31, 143–158 (2008). https://doi.org/10.2165/00002018-200831020-00004
Published:
Issue Date:
DOI: https://doi.org/10.2165/00002018-200831020-00004