
Abstract
Background
Cardiovascular disease remains a leading cause of death worldwide, with hypercholesterolemia being a major risk factor. Evidence-based consensus guidelines have recommended consideration of increasingly stringent cholesterol-lowering goals, yet most patients do not meet these targets. Coronary heart disease (CHD) event and mortality rates and mean serum cholesterol levels have declined in Singapore in recent years; however, certain groups remain at elevated risk.
Objective
To determine (i) proportions of patients with CHD in Singapore who achieved goals for serum low-density lipoprotein-cholesterol (LDL-C); and (ii) factors influencing goal attainment.
Methods
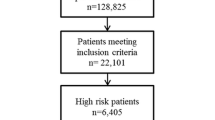
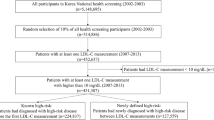
A historical cohort study was conducted using records from the Singapore Cardiac Databank, a national registry of CHD patients. Serum LDL-C goal attainment was assessed in 5174 survivors of acute myocardial infarction or coronary revascularization (i.e. coronary artery bypass graft surgery or percutaneous coronary interventions), of whom 3811 (73.7%) were at very high risk.
Results
At baseline, the mean patient age was 60.3 years, mean serum value of total cholesterol was 228 mg/dL, and mean LDL-C was 163mg/dL. Of all CHD patients, approximately 70% did not achieve a serum LDL-C target of <100mg/dL. Most patients receiving HMG-CoA reductase inhibitor (statin) regimens were treated initially with low- to medium-equipotency regimens and were never titrated to stronger regimens. The vast majority (∼94%) of patients at very high risk did not achieve the stringent serum LDL-C target of <70mg/dL. Patients receiving higher potency statins were significantly more likely to achieve LDL-C goals, whereas those with higher baseline LDL-C levels or Malaysian ethnicity were less likely to achieve LDL-C goals.
Conclusions
Most CHD patients in the large group of Singapore residents with CHD in the present study did not achieve recommended LDL-C targets. A more effective disease-management approach, including patient education concerning lifestyle modification (e.g. diet, physical activity), efforts to enhance medication adherence, and more effective, well tolerated therapies such as high-equipotency or high-dose statins and statin combination regimens, may be needed to improve achievement of consensus cholesterol targets. This is the first study of cholesterol goal attainment in a large group of Southeast Asians and serves as a baseline for future evaluations in Asian populations.








Similar content being viewed by others

References
World Health Organization. World health report 1999: making a difference [online]. Available from URL: http://www.who.int/whr/en/ [Accessed 2006 May 23].
World Health Organization. World health report 2003: shaping the future [online]. Available from URL: http://www.who.int/whr/en/ [Accessed 2006 Jan 29].
Ounpuu S, Yusuf S. Singapore and coronary heart disease: a population laboratory to explore ethnic variations in the epidemiologic transition. Eur Heart J 2003 Jan; 24(2): 127–9.
Stamler J, Wentworth D, Neaton JD. Is relationship between serum cholesterol and risk of premature death from coronary heart disease continuous and graded? Findings in 356,222 primary screenees of the Multiple Risk Factor Intervention Trial (MRFIT). JAMA 1986 Nov; 256(20): 2823–8.
Martin MJ, Hulley SB, Browner WS, et al. Serum cholesterol, blood pressure, and mortality: implications from a cohort of 361,662 men. Lancet 1986 Oct; II(8513): 933–6.
Stason WB. Costs and benefits of risk factor reduction for coronary heart disease: insights from screening and treatment of serum cholesterol. Am Heart J 1990 Nov; 119(3 Pt 2): 718–24.
Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994 Nov; 344 (8934): 1383–9.
Shepherd J, Cobbe SM, Ford I, et al. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia: West of Scotland Coronary Prevention Study Group. N Engl J Med 1995 Nov; 333(20): 1301–7.
Sacks FM, Pfeffer MA, Moyé LA, et al. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels: Cholesterol and Recurrent Events Trial investigators. N Engl J Med 1996 Oct; 335(14): 1001–9.
Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels: the Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med 1998 Nov; 339 (19): 1349–57.
Collins R. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet 2002 Jul; 360(9326): 7–22.
Collins R, Armitage J, Parish S, et al. MRC/BHF Heart Protection Study of cholesterol-lowering with simvastatin in 5963 people with diabetes: a randomised placebo-controlled trial. Lancet 2003 Jun; 361(9374): 2005–16.
Colhoun HM, Betteridge DJ, Durrington PN, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet 2004 Aug; 364(9435): 685–96.
Sever PS, Dahlof B, Poulter NR, et al. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial-Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet 2003 Apr; 361(9364): 1149–58.
Collins R, Armitage J, Parish S, et al. Effects of cholesterol-lowering with simvastatin on stroke and other major vascular events in 20536 people with cerebrovascular disease or other high-risk conditions. Lancet 2004 Mar; 363(9411): 757–67.
Cannon CP, Braunwald E, McCabe CH, et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med 2004 Apr; 350(15): 1495–504.
Nissen SE, Tuzcu EM, Schoenhagen P, et al. Effect of intensive compared with moderate lipid-lowering therapy on progression of coronary atherosclerosis: a randomized controlled trial. JAMA 2004 Mar; 291(9): 1071–80.
Ridker PM, Cannon CP, Morrow D, et al. C-reactive protein levels and outcomes after statin therapy. N Engl J Med 2005 Jan; 352(1): 20–8.
Nissen SE, Tuzcu EM, Schoenhagen P, et al. Statin therapy, LDL cholesterol, C-reactive protein, and coronary artery disease. N Engl J Med 2005 Jan; 352(1): 29–38.
LaRosa JC, Grundy SM, Waters DD, et al. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med 2005 Apr; 352(14): 1425–35.
Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005 Oct; 366(9493): 1267–78.
Gould AL, Rossouw JE, Santanello NC, et al. Cholesterol reduction yields clinical benefit: impact of statin trials. Circulation 1998 Mar; 97(10): 946–52.
De Backer G, Ambrosioni E, Borch-Johnsen K, et al. European guidelines on cardiovascular disease prevention in clinical practice: Third Joint Task Force of European and other societies on cardiovascular disease prevention and clinical practice. Eur J Cardiovasc Prev Rehabil 2003; 10 Suppl. 1: S1–S78.
International Atherosclerosis Society. Harmonized clinical guidelines on prevention of atherosclerotic vascular disease: executive summary [online]. Available from URL: http://www.athero.org/download/guidelines.pdf [Accessed 2005 May 10].
Adult Treatment Panel. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002 Dec; 106(25): 3143–421.
Grundy SM, Cleeman JI, Merz CN, et al. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation 2004 Jul; 110(2): 227–39.
Pearson TA, Laurora I, Chu H, et al. The Lipid Treatment Assessment Project (L-TAP): a multicenter survey to evaluate the percentages of dyslipidemic patients receiving lipid-lowering therapy and achieving low-density lipoprotein cholesterol goals. Arch Intern Med 2000 Feb; 160(4): 459–67.
EUROASPIRE I and II Group. Clinical reality of coronary prevention guidelines: a comparison of EUROASPIRE I and II in nine countries. EUROASPIRE I and II Group: European Action on Secondary Prevention by Intervention to Reduce Events. Lancet 2001 Mar; 357(9261): 995–1001.
Sueta CA, Chowdhury M, Boccuzzi SJ, et al. Analysis of the degree of undertreatment of hyperlipidemia and congestive heart failure secondary to coronary artery disease. Am J Cardiol 1999 May; 83(9): 1303–7.
Marcelino JJ, Feingold KR. Inadequate treatment with HMG-CoA reductase inhibitors by health care providers. Am J Med 1996 Jun; 100(6): 605–10.
Van Ganse E, Laforest L, Alemao E, et al. Lipid-modifying therapy and attainment of cholesterol goals in Europe: the return on expenditure achieved for lipid therapy (REALITY) study. Curr Med Res Opin 2005 Sep; 21(9): 1389–99.
Singapore Department of Statistics. Statistics Singapore 2005 [online]. Available from URL: http://www.singstat.gov.sg/ [Accessed 2005 May 10].
Lim MK. Health care systems in transition II: Singapore. Part I: an overview of health care systems in Singapore. J Public Health Med 1998 Mar; 20(1): 16–22.
Seow A, Hin-Peng L. From colony to city state: changes in health needs in Singapore from 1950 to 1990. J Public Health Med 1994 Jun; 16(2): 149–58.
Tan CE, Emmanuel SC, Tan BY, et al. Prevalence of diabetes and ethnic differences in cardiovascular risk factors: the 1992 Singapore National Health Survey. Diabetes Care 1999 Feb; 22(2): 241–7.
Janus ED, Postiglione A, Singh RB, et al. The modernization of Asia: implications for coronary heart disease: council on Arteriosclerosis of the International Society and Federation of Cardiology. Circulation 1996 Dec; 94(11): 2671–3.
Deurenberg-Yap M, Chew SK, Deurenberg P. Elevated body fat percentage and cardiovascular risks at low body mass index levels among Singaporean Chinese, Malays and Indians. Obes Rev 2002 Aug; 3(3): 209–15.
Deurenberg-Yap M, Chew SK, Lin VF, et al. Relationships between indices of obesity and its co-morbidities in multi-ethnic Singapore. Int J Obes Relat Metab Disord 2001 Oct; 25(10): 1554–62.
Ng TP, Mak KH, Phua KH, et al. Trends in mortality, incidence, hospitalisation, cardiac procedures and outcomes of care for coronary heart disease in Singapore, 1991–1996. Ann Acad Med Singap 1999 May; 28(3): 395–401.
Mak KH, Chia KS, Kark JD, et al. Ethnic differences in acute myocardial infarction in Singapore. Eur Heart J 2003 Jan; 24(2): 151–60.
Ministry of Health Singapore. National Health Survey 2004 [online]. Available from URL: http://www.moh.gov.sg/corp/hottopics/NationalHealthSurvey/index.do#31457517 [Accessed 2006 Jan 29].
Emmanuel SC, Tan AT, Tunstall-Pedoe H, et al. The operational research study for the Singapore Myocardial Infarction Register. Singapore Med J 1988 Oct; 29(5): 446–57.
Maron DJ, Fazio S, Linton MF. Current perspectives on statins. Circulation 2000 Jan; 101(2): 207–13.
Nagashima H, Kasunaki H. The status of lipid management in 1836 patients with coronary artery disease. J Atheroscl Thrombosis 2005; 12: 338–42.
Dwyer T, Emmanuel SC, Janus ED, et al. The emergence of coronary heart disease in populations of Chinese descent. Atherosclerosis 2003 Apr; 167(2): 303–10.
Tan CE, Tai ES, Tan CS, et al. APOE polymorphism and lipid profile in three ethnic groups in the Singapore population. Atherosclerosis 2003 Oct; 170(2): 253–60.
Hughes K, Yeo PP, Lun KC, et al. Cardiovascular diseases in Chinese, Malays, and Indians in Singapore: II. Differences in risk factor levels. J Epidemiol Community Health 1990 Mar; 44(1): 29–35.
Middleton A, Binbrek AS, Fonseca FA, et al. Achieving 2003 European lipid goals with rosuvastatin and comparator statins in 6743 patients in real-life clinical practice: DISCOVERY meta-analysis. Curr Med Res Opin 2006; 22: 1181–91.
Bullano MF, Wertz DA, Yang GW, et al. Effect of rosuvastatin compared with other statins on lipid levels and National Cholesterol Education Program goal attainment for low-density lipoprotein cholesterol in a usual care setting. Pharmacotherapy 2006; 26: 469–78.
Stein E, Stender S, Mata P, et al. Achieving lipoprotein goals in patients at high risk with severe hypercholesterolemia: efficacy and safety of ezetimibe co-administered with atorvastatin. Am Heart J 2004 Jan; 148(3): 447–55.
Gagné C, Bays HE, Weiss SR, et al. Efficacy and safety of ezetimibe added to ongoing statin therapy for treatment of patients with primary hypercholesterolemia. Am J Cardiol 2002 Nov; 90(10): 1084–91.
Ballantyne CM, Abate N, Yuan Z, et al. Dose-comparison study of the combination of ezetimibe and simvastatin (Vytorin) versus atorvastatin in patients with hypercholesterolemia: the Vytorin Versus Atorvastatin (VYVA) study. Am Heart J 2005 Mar; 149(3): 464–73.
Zow HC, Hsu AA, Eng PC. Smoking cessation programme: the Singapore General Hospital experience. Singapore Med J 2004; 45: 430–4.
Koh WP, Yuan JM, Sun CL, et al. Middle-aged and older Chinese men and women in Singapore who smoke have less healthy diets and lifestyles than nonsmokers. J Nutr 2005; 135: 2473–7.
Alemao E, Yin D, Sintonen H, et al. Evaluation of lipid-lowering therapy and cholesterol goal attainment in Finland: the national FINRISK study. Am J Cardiovasc Drugs 2006 Oct; 6(5): 349–55.
Acknowledgments
Assistance in manuscript preparation was provided by Stephen W. Gutkin, Rete Biomedical Communications Corp. (Ridgewood, NJ, USA). Med Data Analytics Inc. had access to the database on which this study report was based. Dr Binayak Deb assisted in acquiring, analyzing, and interpreting data.
Author contributions: Study concept: Kheng-Thye Ho; Study design: Dr Ho and all other authors; Acquisition of data: Dr Ho, Khong-Whee Chin, and Kheng-Siang Ng; Analysis and interpretation of data; all authors; Drafting of the manuscript: Dr Ho with editorial assistance from Stephen W. Gutkin; Critical revision of the manuscript for important intellectual content: all authors; Statistical analysis: Srinivasan Rajagopalan; Obtained funding: Dr Ho; Administrative, technical, and material support: Evo Alemao; Study supervision: Dr Ho. Financial support for the study was provided by a grant from MSP (Merck/Schering-Plough) Singapore Company, LLC.
Conflicts of interest are as follows: Khong-Whee Chin is an employee of Merck Research Laboratories, Merck and Co., Inc. Evo Alemao and Don Yin are employees of Merck and Co., Inc., and are Merck shareholders (stocks and stock options). Srinivasan Rajagopalan and Stephen W. Gutkin are paid consultants to Merck. Neither Kheng-Thye Ho nor Kheng-Siang Ng has any affiliation with the sponsor or any financial interests in this report.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ho, KT., Chin, KW., Ng, KS. et al. The A-SACT (Achievement in Singapore of Cholesterol Targets) Study in Patients with Coronary Heart Disease. Am J Cardiovasc Drugs 6, 383–391 (2006). https://doi.org/10.2165/00129784-200606060-00005
Published:
Issue Date:
DOI: https://doi.org/10.2165/00129784-200606060-00005