
Abstract
Ranolazine is a compound that is approved by the US FDA for the treatment of chronic angina pectoris in combination with amlodipine, β-adrenoceptor antagonists or nitrates, in patients who have not achieved an adequate response with other anti-anginals. The anti-anginal effect of ranolazine does not depend on changes in heart rate or blood pressure. It acts through different pharmacological mechanisms where inhibition of the late inward sodium current (reducing calcium overload and thereby left ventricular diastolic tension) is one plausible mechanism of reduced oxygen consumption. Initial studies used an oral solution or an immediate-release (IR) capsule, but subsequently an extended-release (ER) formulation was developed to allow for twice-daily administration with maintained efficacy.
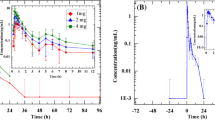
Following administration of an oral solution or IR capsule, peak plasma concentrations (Cmax) are observed within 1 hour. After administration of radio-labelled ranolazine, 73% of the dose was excreted in urine, and unchanged ranolazine accounted for <5% of radioactivity in both urine and faeces. The absolute bioavailability ranges from 35% to 50%. Food has no effect on rate or extent of absorption from the ER formulation. Ranolazine protein binding is about 61–64% over the therapeutic concentration range. Volume of distribution at steady state ranges from 85 to 180L.
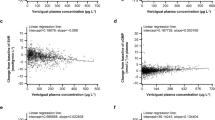
Ranolazine is extensively metabolised by cytochrome P450 (CYP) 3A enzymes and, to a lesser extent, by CYP2D6, with approximately 5% excreted renally unchanged. Elimination half-life of ranolazine is 1.4–1.9 hours but is apparently prolonged, on average, to 7 hours for the ER formulation as a result of extended absorption (flip-flop kinetics). Elimination occurs through parallel linear and saturable elimination pathways, where the saturable pathway is related to CYP2D6, which is partly inhibited by ranolazine. Oral plasma clearance diminishes with dose from, on average, 45 L/h at 500mg twice daily to 33 L/h at 1000mg twice daily. The departure from dose proportionality for this dose range is modest, with increases in steady-state Cmax and area under plasma concentration-time curve (AUC) from 0 to 12 hours of 2.5- and 2.7-fold, respectively. Ranolazine pharmacokinetics are unaffected by sex, congestive heart failure and diabetes mellitus. AUC increases up to 2-fold with advancing degree of renal impairment.
Ranolazine is a weak inhibitor of CYP3A, and increases AUC and Cmax for simvastatin, its metabolites and HMG-CoA reductase inhibitor activity <2-fold. Digoxin AUC is increased 40–60% by ranolazine through P-glycoprotein inhibition. Ranolazine AUC is increased by C YP3 A inhibitors ranging from 1.5-fold for diltiazem 180mg once daily to 3.9-fold for ketoconazole 200mg twice daily. Verapamil increases ranolazine exposure approximately 2-fold. CYP2D6 inhibition has a negligible effect on ranolazine exposure.















Similar content being viewed by others

Notes
The use of trade names is for product identification purposes only and does not imply endorsement.
References
Cocco G, Rousseau MF, Bouvy T, et al. Effects of a new metabolic modulator, ranolazine, on exercise tolerance in angina pectoris patients treated with beta-blocker or diltiazem. J Cardiovasc Pharmacol 1992; 20(1): 131–8
Chaitman BR, Pepine CJ, Parker JO, et al. Effects of ranolazine with atenolol, amlodipine, or diltiazem on exercise tolerance and angina frequency in patients with severe chronic angina: a randomized controlled trial. JAMA 2004; 291(3): 309–16
Chaitman BR, Skettino SL, Parker JO, et al. Anti-ischemic effects and long-term survival during ranolazine monotherapy in patients with chronic severe angina. J Am Coll Cardiol 2004; 43(8): 1375–82
Rousseau MF, Pouleur H, Cocco G, et al. Comparative efficacy of ranolazine versus atenolol for chronic angina pectoris. Am J Cardiol 2005; 95(3): 311–6
Antzelevitch C, Belardinelli L, Zygmunt AC, et al. Electrophysiological effects of ranolazine, a novel antianginal agent with antiarrhythmic properties. Circulation 2004; 110: 904–10
Song Y, Shryock JC, Wu L, et al. Antagonism by ranolazine of the pro-arrhythmic effects of increasing late INa in guinea pig ventricular myocytes. J Cardiovasc Pharmacol 2004; 44(2): 192–9
Belardinelli L, Antzelevitch C, Fraser H. Inhibition of late (sustained/persistent) sodium current: a potential drug target to reduce intracellular sodium-dependent calcium overload and its detrimental effects on cardiomyocyte function. Eur Heart J Suppl I 2004; 6: 113–17
Meyer M, Keweloh B, Guth K, et al. Frequency-dependence of myocardial energetics in failing human myocardium as quantified by a new method for the measurement of oxygen consumption in muscle strip preparations. J Mol Cell Cardiol 1998; 30(8): 1459–70
Hayashida W, van Eyll C, Rousseau MF, et al. Effects of ranolazine on left ventricular regional diastolic function in patients with ischemic heart disease. Cardiovasc Drugs Ther 1994; 8(5): 741–7
Beal SL, Sheiner LB. NONMEM users guide. Part I: users basic guide. USCF, San Francisco (CA): NONMEM Project Group, 1989
Cockroft D, Gault M. Prediction of creatinine clearance from serum creatinine. Nephron 1976; 16: 31–41
Jerling M, Huan B-L, Leung K, et al. Studies to investigate the pharmacokinetic interactions between ranolazine and ketoconazole, diltiazem, or simvastatin during combined administration in healthy subjects. J Clin Pharmacol 2005; 45(4): 422–33
Jerling M, Farrell C. Population pharmacokinetics of ranolazine [abstract]. J Clin Pharmacol 2005; 45: 29
Prueksaritanont T, Gorham LM, Ma B, et al. In vitro metabolism of simvastatin in humans [SBT]identification of metabolizing enzymes and effect of the drug on hepatic P450s. Drug Metab Dispos 1997; 25(10): 1191–9
Prueksaritanont T, Ma B, Yu N. The human hepatic metabolism of simvastatin hydroxy acid is mediated primarily by CYP3A, and not CYP2D6. Br J Clin Pharmacol 2003; 56(1): 120–4
Lilja JJ, Kivisto KT, Neuvonen PJ. Grapefruit juice-simvastatin interaction: effect on serum concentrations of simvastatin, simvastatin acid, and HMG-CoA reductase inhibitors. Clin Pharmacol Ther 1998; 64(5): 477–83
Neuvonen PJ, Kantola T, Rivisto KT. Simvastatin but not pravastatin is very susceptible to interaction with the CYP3A4 inhibitor itraconazole. Clin Pharmacol Ther 1998; 63(3): 332–41
CVT technical report CVT303.010-N: the P170-glycoprotein transporter as a potential site of the ranolazine/digoxin drug interaction. 2002 Aug 20
Tiberghien F, Loor F. Ranking of P-glycoprotein substrates and inhibitors by a calcein-AM fluorometry screening assay. Anticancer Drugs 1996; 7(5): 568–78
Yeo KR, Yeo WW. Inhibitory effects of verapamil and diltiazem on simvastatin metabolism in human liver microsomes. Br J Clin Pharmacol 2001; 51(5): 461–70
Koren G, Woodland C, Ito S. Toxic digoxin-drug interactions: the major role of renal P-glycoprotein. Vet Hum Toxicol 1998; 40(1): 45–6
Wakasugi H, Yano I, Ito T, et al. Effect of clarithromycin on renal excretion of digoxin: interaction with P-glycoprotein. Clin Pharmacol Ther 1998; 64(1): 123–8
Westphal K, Weinbrenner A, Giessmann T, et al. Oral bioavailability of digoxin is enhanced by talinolol: evidence for involvement of intestinal P-glycoprotein. Clin Pharmacol Ther 2000; 68(1): 6–12
Breckenridge A, Orme M, Wesseling H, et al. Pharmacokinetics and pharmacodynamics of the enantiomers of warfarin in man. Clin Pharmacol Ther 1974; 15(4): 424–30
Rettie AE, Korzekwa KR, Kunze KL, et al. Hydroxylation of warfarin by human cDNA-expressed cytochrome P-450: a role for P-4502C9 in the etiology of (S)-warfarin-drug interactions. Chem Res Toxicol 1992; 5(1): 54–9
Kaminsky LS, Zhang ZY. Human P450 metabolism of warfarin. Pharmacol Ther 1997; 73(1): 67–74
Cotreau MM, von Moltke LL, Greenblatt DJ. The influence of age and sex on the clearance of cytochrome P450 3A substrates. Clin Pharmacokinet 2005; 44(1): 33–60
Fleisher D, Li C, Zhou Y, et al. Drug, meal and formulation interactions influencing drug absorption after oral administration: clinical implications. Clin Pharmacokinet 1999; 36: 233–54
Jerling M, Abdallah H. Effect of renal impairment on multiple-dose pharmacokinetics of extended-release ranolazine. Clin Pharmacol Ther 2005; 78(3): 288–97
Dreisbach AW, Lertora JJ. The effect of chronic renal failure on hepatic drug metabolism and drug disposition. Semin Dial 2003; 16(1): 45–50
Abdallah H, Jerling M. Effect of hepatic impairment on the multiple-dose pharmacokinetics of ranolazine sustained-release tablets. J Clin Pharmacol 2005; 45(7): 802–9
Pugh RN, Murray-Lyon IM, Dawson JL, et al. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg 1973; 60(8): 646–9
Leithe M, Margorien R, Hermiller J, et al. Relationship between central hemodynamics and regional blood flow in normal subjects and in patients with congestive heart failure. Circulation 1984; 69(1): 57–64
Matzke G, Frye R, Early J, et al. Evaluation of the influence of diabetes mellitus on antipyrine metabolism and CYP1A2 and CYP2D6 activity. Pharmacotherapy 2000; 20: 182–90
Acknowledgements
Funding to assist in the preparation of this review was provided by CV Therapeutics, Inc., Palo Alto, CA, USA
Dr Jerling was an employee of CV Therapeutics at the time of studies conduct and reporting, and is currently a consultant to CV Therapeutics.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jerling, M. Clinical Pharmacokinetics of Ranolazine. Clin Pharmacokinet 45, 469–491 (2006). https://doi.org/10.2165/00003088-200645050-00003
Published:
Issue Date:
DOI: https://doi.org/10.2165/00003088-200645050-00003