
Abstract
Cyclooxygenase-2 (COX-2) and inducible nitric oxide synthase (iNOS) play crucial roles in diabetic angiopathy. In vivo, however, the following facts remain unknown: whether COX-2 and iNOS bind, how peroxynitrite-induced nitration of COX-2 and iNOS affects their binding if they do bind and what effects of this mechanism contribute to diabetic angiopathy. This study focused on the issues above. Diabetes was induced in Wistar male rats by intraperitoneal injection of streptozotocin. As a specific scavenger of peroxynitrite, urate was used. After 13 wks of diabetes, the morphological and biochemical changes of the rats showed obvious diabetic angiopathy. There exists in vivo colocalization and binding of COX-2 and iNOS in diabetic angiopathy. The nitration level of total and coimmunoprecipitated COX-2 and iNOS increased significantly, and, simultaneously, their binding and activity increased in the diabetes group. In the diabetes + urate group, the nitration level of COX-2 and iNOS decreased and their binding reduced, consistent with their decreased activity and the attenuated pathological changes in the rat aorta and glomerulus. The results provide in vivo evidence that COX-2 and iNOS can bind in diabetic angiopathy and that peroxynitrite-induced nitration of COX-2 and iNOS promotes their binding, contributing to diabetic angiopathy.
Similar content being viewed by others


Introduction
The chronic vascular complications of diabetes, including macrovascular (atherosclerosis) and microvascular (nephropathy) diseases, are major causes of morbidity and premature mortality (1,2). Mounting evidence shows that inflammation and oxidative stress are important pathophysiological facts (3–5).
Cyclooxygenase-2 (COX-2) and inducible nitric oxide synthase (iNOS) are key enzymes in inflammation and oxidative stress, respectively (6). Both are inducible enzymes and have synergistic alterations, mediating similar pathological processes (7). In diabetes, COX-2 and iNOS can be upregulated and play a key role in diabetic angiopathy. Interestingly, studies have shown that COX-2 and iNOS can bind in vitro, resulting in their enhanced activity (8,9). However, the potentiality of the in vivo binding of COX-2 and iNOS, and the pathophysiological role of their binding in diabetic angiopathy, are unclear.
Our previous studies demonstrated that peroxynitrite is a key mediator of diabetic complications (10,11). Peroxynitrite can cause conspicuous nitration to tyrosine residue of proteins (11). The product of protein tyrosine nitration, nitrotyrosine (NT), is the marker of peroxynitrite-caused nitration, indirectly reflecting the formation and localization of peroxynitrite (12). Once proteins are nitrated by peroxynitrite, their structure and functions are altered (13,14). However, the effect of peroxynitrite-induced nitration of COX-2 and iNOS on their binding in diabetic angiopathy remains unknown.
Recently, it was shown that urate acts as an endogenous peroxynitrite scavenger and can inhibit the action of peroxynitrite in causing tyrosine nitration in a physiological concentration (15–19).
In this study, diabetes was induced with streptozotocin, and urate was used as a specific scavenger of peroxynitrite. The colocalization and binding of COX-2 and iNOS, their nitration level, their activity and the pathological changes in the rat aorta and glomerulus were evaluated to investigate whether COX-2 and iNOS bind in vivo, how peroxynitrite-induced nitration of COX-2 and iNOS affects their binding and what effect of it contributes to diabetic angiopathy.
Materials and Methods
Animals and Tissue Preparation
The experimental protocol followed the guidelines established by the Ethics Review Committee for Animal Experimentation of Hebei Medical University. A total of 28 healthy Wistar male rats (407.05 ± 59.51 g) were provided by the Department of Experimental Animals of Tongji Medical College, Hubei province, with the animal certificate number 19–25. Rats were divided randomly into three groups: the diabetes group (n = 10), the diabetes + urate group (n = 9) and the control group (n = 9). The former two groups were injected intraperitoneally with streptozotocin (40 mg/kg, dissolved in 0.1 mol/L citrate buffer, pH 4.4, freshly made, 10 mg/mL) to induce diabetes. The control group was injected with equivalent saline (40 mg/kg). Three days after injection, diabetes was confirmed by a concentration of fasting blood glucose >13 mmol/L, determined by a glucometer (Johnson, New Bruswick, NJ, USA), and urine glucose (+ + + or above), determined by urine glucose test kits. Rats in the diabetes + urate group were fed urate solution (160 mg/kg/day) in a physiological concentration (17), and others were given equivalent water. After the rats were raised for 13 wks at room temperature (20–25°C), body weight and fasting blood glucose were measured in the morning. After the rats were killed by femoral artery bleeding, the aorta and renal cortex were collected and analyzed to represent diabetic macrovascular and microvascular complications. Pieces of aorta or renal cortex (1 g) were used for morphological observations and laser confocal microscopy analysis, and the rest of the pieces were put into liquid nitrogen and preserved at −70°C for future molecular biological measurement.
Morphology of Rat Aorta and Glomerulus
A segment of aorta or renal cortex was fixed by 4% paraformaldehyde, followed with routine dehydration, embedding, cutting with microtome, dewaxing, hematoxylin-eosin (HE) staining or periodic acid Schiff staining and then observed under an optical microscope. A segment of aorta or renal cortex was fixed by 4% glutaraldehyde for observation through a transmission electron microscope (TEM). The samples were post-fixed in 2% osmium tetroxide, dehydrated in an ascending series of ethanol and embedded in Epon812. Ultrathin sections were cut on an LKB-8800 ultramicrotome (LKB, Bromma, Sweden) and collected on grids. Sections were stained with uranyl acetate and lead citrate and evaluated under an H-500 TEM (Hitachi, Tokyo, Japan). The number of endothelial cells from 10 visual fields on HE-stained slides at random in each group was recorded, and the ratios of the numbers in the diabetes group and the diabetes + urate group to those in the control group were calculated to evaluate endothelial damage. In each group, the glomerular area of 30 glomeruli on HE-stained slides was measured using MetaVue software (MetaVue, Munich, Germany) to evaluate glomerular hypertrophy. Under TEM observation, the thickness of the glomerular basement membrane was measured in five glomeruli from each group, and 100 measurements per glomerulus were taken (ASM Leitz, Wetzlar, Germany). The perpendicular distance from the endothelial cell boundary to the epithelial cell boundary of the glomerular basement membrane was then measured.
Laser Confocal Microscopy Assay of Colocalization of COX-2 and iNOS
The aorta or renal cortex was frozen at −70°C for at least 2 h, cut into 10-µm thick sections at −20°C and air-dried for 1 h at room temperature. After being washed with phosphate-buffered saline (PBS) three times (5 min per time), the section was incubated with 3% methanol-dioxygen for 15 min and incubated with 1% Triton X-100 for 30 min. The section was then blocked with 10% goat serum for 1 h and incubated with the primary antibody (COX-2: rabbit antirat, iNOS: mouse anti-rat in order, diluted 1:150; Santa Cruz Biotechnology, Santa Cruz, CA, USA) at 37°C for 2 h, respectively. Then, after being washed with PBS three times (5 min per time), the section was incubated with a combination of the secondary antibody (fluorescein isothiocyanate [FITC]: goat antirabbit; tetramethylrhodamine isothiocyanate [TRITC]: goat antimouse, diluted 1:100; Zhongshan, Beijing, China) at 37°C for 30 min. The section was then washed with PBS three times (5 min per time), and images were taken during the same intervals and analyzed with a laser confocal scanning microscope. To get exact results, negative controls (PBS instead of the first antibody and the second antibody) and positive controls (the first antibody or the second antibody only) were designed.
Western Blotting Detection of Nitration of COX-2 and iNOS
A segment of aorta or renal cortex was homogenized in lysis buffer (20 mmol/L Tris-Cl, pH 7.5, 100 mmol/L NaCl, 5 mmol/L MgCl2, 1 mmol/L EDTA, 1% Triton X-100, 1 mmol/L dithiothreitol, 1 mmol/L phenylmethylsulfonyl fluoride) and centrifuged at 12,092g at 4°C for 15 min. The supernatant was collected, and its concentration was determined by the Lowry method. Western blotting was used to detect COX-2, iNOS and NT content. The sample (100 µg), diluted in loading buffer and heated at 100°C for 5 min, was then subjected to electrophoresis on 10% SDS-PAGE at 40 mA. After transfer of the proteins to a polyvinylidene difluoride membrane, the membrane was rinsed briefly in PBS and blocked in blocking buffer (5% bovine serum albumin) for at least 1 h. Then, the membrane was incubated overnight with the primary antibody (monoclonal rabbit anti-COX-2 antibody; polyclonal mouse anti-iNOS antibody; diluted 1:200), washed with PBST (0.05% Tween-20 in PBS) three times (10 min per time) and reacted with the secondary antibody (COX-2: goat antirabbit; iNOS: goat anti-mouse; diluted 1:1,000) for 1.5 h at room temperature. After being washed with PBST three times (10 min per time), the membrane was developed with an enhanced chemiluminescence kit (Pierce, Rockford, IL, USA). Then, after being washed with PBST overnight, the membrane was reused to detect the NT content in the COX-2 or iNOS protein. The membrane was incubated with the primary antibody (monoclonal mouse anti-NT antibody, diluted 1:300; Cayman Chemical, Ann Arbor, MI, USA) and then the secondary antibody (NT: goat anti-mouse, diluted 1:1,000; Zhongshan, Beijing, China). Then, the membrane was developed with an enhanced chemiluminescence kit. The gray scale value was analyzed and calculated. β-Actin was routinely served as a loading control.
Coimmunoprecipitation Analysis of Binding of COX-2 and iNOS
After the aorta or renal cortex was homogenized and determined in Western blotting, the sample (500 µg) was reacted with 2 µg of the primary antibody (monoclonal rabbit anti-COX-2 antibody or polyclonal mouse anti-iNOS antibody) for 3 h and then incubated with 20 µL Protein G PLUS-Agarose overnight at 4°C and centrifuged at 447g for 10 min at 4°C. Then the sediment was collected and washed with wash buffer (50 mmol/L Tris Cl, pH 7.5, 50 mmol/L NaCl) three times. The coimmunoprecipitated proteins were collected, diluted in loading buffer, heated at 100°C for 5 min and then subjected to electrophoresis on 10% SDS-PAGE at 40 mA. Western blotting was used to detect the protein content of coimmunoprecipitated iNOS or COX-2 and its NT content, through the procedure followed above.
Analysis of Enzyme Activity of COX-2 and iNOS
Because diabetes-induced inflammation and oxidative stress are widespread in the body, the activity of COX-2 and iNOS in the serum was measured. The activity of COX-2 in the serum was analyzed with a COX activity assay kit (Cayman Chemical) in accordance with the manufacturer’s instructions, using isospecific inhibitors supplied with the kit. The activity of iNOS in the serum was detected by an iNOS activity assay kit (Nanjing Jiancheng, Nanjing City, China), in accordance with the manufacturer’s instructions.
Statistical Analysis
The results are presented as mean ± SD. Differences between the two groups were evaluated by the Student t test, and P < 0.05 was considered statistically significant.
Results
Biochemical and Morphological Changes of Diabetic Angiopathy
Compared with the control group, body weight decreased and blood glucose increased significantly in the diabetes group (P < 0.01). There was no significant difference between the diabetes group and the diabetes + urate group, showing that urate treatment could not affect the body weight and blood glucose of diabetic rats. Data were shown in Table 1.
Typical changes to the aortic endothelium were evaluated by HE staining (Figure 1A) and TEM observation (Figure 1B). The intact endothelium was seen in the control group, the endothelium was falling in the diabetes group and only part of the endothelium was falling in the diabetes + urate group. The ratio of endothelial cell numbers in the diabetes group to that in the control group was 7.5%, and the ratio of the diabetes + urate group was 65.1% (Table 2). Under a TEM, endothelial cells with numerous pinocytosis vesicles and intact mitochondria were observed in the control group. Endothelial cells were damaged severely, which included major mitochondrial crests and cell junction that was fused or had disappeared in the diabetes group. In the diabetes + urate group, the pathological change in the aortic endothelial cell was significantly attenuated.

Pathological changes in the aortic endothelium of diabetic rat. (A) HE staining of the aorta in different groups (×400). The intact endothelium was seen in the control group, the endothelium was falling in the diabetes group and only part of the endothelium was falling in the diabetes + urate group (the black arrow indicates endothelial cells). (B) Ultrastructure of the endothelial cell under a TEM (40,000-fold). An endothelial cell with numerous pinocytosis vesicles (indicated by the black arrow) and intact mitochondria was observed in the control group. However, the endothelial cell was damaged severely in the diabetes group. In the diabetes + urate group, mitochondrial damages attenuated, and only parts of the cell junction were fused in the endothelial cell (red arrows indicate mitochondrium and blue arrows indicate cell junction).
The typical changes in the glomerulus were evaluated by HE staining (Figure 2A), periodic acid Schiff staining (Figure 2B) and TEM observation (Figure 2C). The pathological changes in the glomerulus were not found in the control group. Glomerular hypertrophy with broadened capsular space, fused intercapillary cells and thickened basement membrane was observed in the diabetes group. The pathological changes in the glomerulus were significantly lighter in the diabetes + urate group than in the diabetes group. Compared with the control group, the glomerular area and thickness of the glomerular basement membrane increased significantly in the diabetes group (P < 0.01), and urate treatment could inhibit the increase in the diabetes group (P < 0.01) (Table 2).

Pathological changes in the glomerulus of the diabetic rat. HE staining (A) and periodic acid Schiff staining (B) of the glomerulus in different groups (×400). (C) Ultrastructure of glomerulus under a TEM (×20K). The pathological changes in the glomerulus and its basement membrane were not found in the control group. Glomerular swelling was observed in the diabetes group. The pathological changes in the glomerulus and its basement membrane were significantly lighter in the diabetes + urate group than in the diabetes group (arrows indicate the glomerular basement membrane).
Colocalization of COX-2 and iNOS in the Aorta and Glomerulus of Diabetic Rats
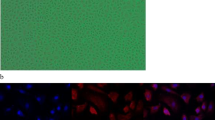
The colocalization of COX-2 and iNOS in the rat aorta (Figure 3A) and glomerulus (Figure 3B) was detected with laser confocal microscopy. The content and colocalization of COX-2 and iNOS in the rat aorta (Figure 3C) and glomerulus (Figure 3D) were evaluated. The above indicators were not detected in the control group. In the diabetes group, the content of COX-2 and iNOS increased significantly, and obvious colocalization was observed. The content of COX-2 and iNOS reduced (P < 0.05 or P < 0.01), and their colocalization weakened in the diabetes + urate group.

Colocalization of COX-2 and iNOS in the rat aorta and glomerulus. The colocalization of COX-2 and iNOS in the aorta (A) and glomerulus (B) was evaluated. COX-2 (green) and iNOS (red) and their colocalization (yellow) were indicated by arrows. In both the aorta (C) and glomerulus (D), the protein content of COX-2 and iNOS could not be detected in the control group, increased sharply with obvious colocalization in the diabetes group and reduced significantly with weakened colocalization in the diabetes + urate group. Data were means ± SD (n = 5 in each group, repeated twice). *P < 0.05 or **P < 0.01 versus the diabetes group. AU, arbitrary units.
Binding of COX-2 and iNOS Increases in Aorta and Renal Cortex of Diabetic Rats
The content of β-actin in different groups was the same, showing no differences in loading. Content of COX-2 and iNOS in the rat aorta (Figure 4A) and renal cortex (Figure 4B) was detected by Western blotting. The binding of COX-2 and iNOS in the rat aorta (Figure 5A) and renal cortex (Figure 5B) was detected by coimmunoprecipitation. If COX-2 binds iNOS, COX-2 can be coimmunoprecipitated by the iNOS antibody, and iNOS can be coimmunoprecipitated by the COX-2 antibody. Therefore, detecting the content of coimmunoprecipitated COX-2 and iNOS can reflect their binding. The ratio of coimmunoprecipitated COX-2 to its protein content and the ratio of coimmunoprecipitated iNOS to its protein content were calculated respectively, to avoid the effect of protein content on their binding. The content of coimmunoprecipitated COX-2 and iNOS in the rat aorta (Figure 5C) and renal cortex (Figure 5D) was hardly detected in the control group, increased in the diabetes group and decreased significantly in the diabetes + urate group (P < 0.05).

Nitration level of COX-2 and iNOS in the rat aorta and renal cortex. The protein and NT content in the aorta (A) and renal cortex (B) was detected by Western blotting. To eliminate the effect of protein content, the ratio of NT content to protein content was calculated to show the nitration level of COX-2 and iNOS in the aorta and renal cortex, respectively (C and D). Data were means ± SD (n = 3 in each group, repeated twice). *P < 0.05 or **P < 0.01 versus the diabetes group.

Content and nitration level of coimmunoprecipitated COX-2 and iNOS in the rat aorta and renal cortex. The coimmunoprecipitated COX-2 or iNOS and their nitration level in the aorta (A) and renal cortex (B) were detected by coimmunoprecipitation and Western blotting. The ratio of the coimmunoprecipitated COX-2 or iNOS to its own total protein content was calculated to eliminate the effect of total protein content in the aorta (C) and renal cortex (D), respectively. The ratio of NT content to the content of coimmunoprecipitated COX-2 or iNOS was calculated to show their nitration level in the aorta and renal cortex, respectively (E and F). Data were means ± SD (n = 3 in each group, repeated twice). *P < 0.05 versus the diabetes group.
Nitration of COX-2 and iNOS Promotes Their Binding in the Aorta and Renal Cortex of Diabetic Rats
The nitration level of COX-2 and iNOS was detected by Western blotting. To avoid the effect of protein content on nitration level of COX-2 (Figure 4D) and iNOS (Figure 4C), the ratio of NT content to protein content was calculated to show their nitration level in the rat aorta and renal cortex, respectively. The nitration level of COX-2 and iNOS was not detected in the control group, increased sharply in the diabetes group and decreased significantly in the diabetes + urate group (P < 0.05 or P < 0.01). To show the nitration level of coimmunoprecipitated COX-2 or iNOS, the ratio of NT content to coimmunoprecipitated COX-2 or iNOS was calculated. In the rat aorta and renal cortex, the nitration level of coimmunoprecipitated COX-2 (Figure 5F) or iNOS (Figure 5E) was hardly detected in the control group but was obviously high in the diabetes group and decreased significantly in the diabetes + urate group (P < 0.05). In total and coimmunoprecipitated COX-2 and iNOS, the alteration of their nitration level in different groups was consistent with that of their binding. Therefore, it is shown that nitration of COX-2 and iNOS promoted their binding in diabetic angiopathy.
Nitration of COX-2 and iNOS Enhances Their Activity in Diabetic Rats
Compared with the control group, the activity of COX-2 and iNOS was elevated in the diabetes group (P < 0.01). Their activity was significantly lower in the diabetes + urate group than in the diabetes group (P < 0.01). The results showed that urate could inhibit the activity of COX-2 and iNOS by reducing their nitration. Data are shown in Table 1.
Discussion
Diabetic angiopathy is a major cause of morbidity and mortality in patients with diabetes. The representative vascular complications of diabetes were macrovascular (atherosclerosis) and microvascular (nephropathy) disease, so we chose aorta and glomerulus to represent diabetic angiopathy. Increasingly, studies are demonstrating that inflammation and oxidative stress play a crucial role in pathogenesis of diabetic angiopathy (20,21). COX-2 and iNOS are key enzymes in inflammation and oxidative stress, respectively, mediating similar pathological processes in diabetic complications. This study provides in vivo evidence that COX-2 and iNOS can bind in diabetic angiopathy and that peroxynitrite-induced nitration of COX-2 and iNOS promotes their binding, contributing to diabetic angiopathy.
COX-2 is an inducible enzyme. Once induced, COX-2 can lead to the dramatic and transient synthesis of prostaglandin E2, exaggerating inflammation (22). COX-2 and resultant prostaglandin E2 participate in the pathogenesis of diabetes and its complications, especially diabetic angiopathy. For example, COX-2-mediated endothelial cell apoptosis and vascular smooth muscle hypersensitivity are partially responsible for vascular complications in diabetes (23,24). Importantly, inhibition of COX-2 could reduce renal dysfunctions resulting from diabetes (25). Similar to COX-2, iNOS is also an inducible enzyme, generating excessive NO (26). NO is a free radical, and iNOS-derived NO plays a crucial role in diabetes-related vascular lesions. The iNOS-mediated endothelial dysfunction plays an important role in diabetic vasculopathy (27,28). Also, the iNOS transgene could partly contribute to the pathogenesis of diabetic nephropathy, including glomerular hypertrophy, mesangial expansion and then glomerulosclerosis (29). COX-2 and iNOS usually express at low or undetectable levels but can be significantly induced in a pathological state. In diabetes, COX-2 and iNOS can be upregulated and play a key role in diabetes and its complications (23,27).
In this experiment, the aorta and glomerulus of diabetic rats showed changes typical of diabetic angiopathy, observed by optical microscope and TEM. The content and activity of COX-2 and iNOS increased significantly in the diabetes group, consistent with the pathological changes. Thus, the results of the present study confirmed their roles in the pathogenesis and progression of diabetic angiopathy.
On the ground of numerous studies of COX-2 and iNOS, Kim et al. found that iNOS can bind COX-2 and S-nitrosylate COX-2 and then activate COX-2 in vitro (8). They found that binding and S-nitrosylation were selective and specific, since iNOS did not bind COX-1 and hydrogen peroxide did not elicit S-nitrosylation of COX-2. The iNOS inhibitor, at drug concentrations that provide 50% inhibition of iNOS activity, can reduce 50% formation of prostaglandin E2. Thus, about 50% of induced COX-2 activity is determined by S-nitrosylation. Furthermore, they identified the binding domain of COX-2 and iNOS, elucidating the molecular mechanism of their binding in vitro. On the other hand, Xu et al. demonstrated that COX-2 also had the ability to enhance iNOS-induced S-nitrosylation by direct binding (9). Although COX-2 and iNOS can bind to each other with a synergistic effect, whether they bind in vivo in diabetic angiopathy is not clear.
The results of laser confocal microscopy in this experiment showed the colocalization of COX-2 and iNOS in the aorta and glomerulus of diabetic rats, suggesting that they might bind in diabetic angiopathy. The binding of COX-2 and iNOS in vivo was further confirmed by coimmunoprecipitation. The content of coimmunoprecipitated COX-2 and iNOS represents their binding. In the diabetes group, the binding of COX-2 and iNOS increased obviously. To eliminate the effect of protein content on their binding, the ratio of coimmunoprecipitated COX-2 or iNOS to its own total protein content was calculated. In both the aorta and renal cortex of diabetic rats, the binding of COX-2 and iNOS was promoted significantly. As the binding of COX-2 and iNOS may promote the activity of both COX-2 and iNOS, their enhanced activity ultimately resulted in the pathological changes, aggravating diabetic angiopathy. And the enhanced activity of COX-2 and iNOS, consistent with the typical changes of diabetic angiopathy, was also observed in the study. Thus, we provided evidence that the binding of COX-2 and iNOS existed in vivo, contributing to diabetic angiopathy.
Peroxynitrite, a highly reactive oxidant, is produced by the reaction of NO with free radical superoxide (30,31). Peroxynitrite and its derivatives are the one species with the strongest oxidation known at present, playing a crucial role in the pathogenesis of diabetes and its complications (12,30–34). Peroxynitrite could cause conspicuous nitration to proteins, and NT is believed to be a marker of peroxynitrite-caused damage (12,31–33). Our previous study found that peroxynitrite can induce protein nitration in diabetic complications (11,35). It is reported that peroxynitrite could cause nitration of COX-2 and iNOS, enhancing their activity (36,37). In the present experiment, the increased activity of COX-2 and iNOS decreased with urate treatment, and we could conclude that protein nitration could enhance COX-2 and iNOS activity. However, it remains unclear whether protein nitration enhanced COX-2 and iNOS activity through affecting their binding and what the effect is of peroxynitrite-induced nitration of COX-2 and iNOS on their binding in vivo in diabetic angiopathy.
In this study, the ratio of NT content to protein content was evaluated to exclude the effect of protein content on their nitration level. The results showed that COX-2 and iNOS can be nitrated by peroxynitrite in diabetic angiopathy.
In total protein content and also in the coimmunoprecipitated COX-2 and iNOS, determined by Western blotting and coimmunoprecipitation detection, the nitration level was high in the diabetes group, consistent with their promoted binding. With inhibition of nitration of COX-2 and iNOS by peroxynitrite scavenger urate, their binding, their activity and the pathological changes in the diabetic aorta and glomerulus decreased significantly. The results showed that peroxynitrite-induced nitration of COX-2 and iNOS can promote their binding, contributing to diabetic angiopathy. This study also revealed that nitration of COX-2 and iNOS enhanced their activity through promoting their binding in vivo in diabetic angiopathy.
However, how the nitration of COX-2 and iNOS promotes their binding and which nitrated site will have main effects on their binding in diabetes are still unknown. Maybe nitration of COX-2 and iNOS could cause the alteration of their spatial structure, facilitating or strengthening their binding. Furthermore, the underlying mechanism of the synergistic alterations of COX-2 and iNOS in diabetic angiopathy is not clear. Further studies are needed to clarify these items, with the hope of elucidating the pathogenesis and progression of diabetic angiopathy.
In conclusion, in vivo binding of COX-2 and iNOS exists in diabetic angiopathy, and peroxynitrite-induced nitration of COX-2 and iNOS can promote their binding, which contributes to diabetic angiopathy. Therefore, scavenging peroxynitrite to attenuate binding of COX-2 and iNOS may be a more effective intervention of diabetic angiopathy.
Disclosure
The authors declare that they have no competing interests as defined by Molecular Medicine, or other interests that might be perceived to influence the results and discussion reported in this paper.
References
Rahman S, Rahman T, Ismail AA, Rashid AR. (2007) Diabetes-associated macrovasculopathy: pathophysiology and pathogenesis. Diabetes Obes. Metab. 9:767–80.
Brown WV. (2008) Microvascular complications of diabetes mellitus: renal protection accompanies cardiovascular protection. Am. J. Cardiol. 102:10L–13L.
Agrawal NK, Maiti R, Dash D, Pandey BL. (2007) Cilostazol reduces inflammatory burden and oxidative stress in hypertensive type 2 diabetes mellitus patients. Pharmacol. Res. 56:118–23.
Loomans CJ, et al. (2009) Differentiation of bone marrow-derived endothelial progenitor cells is shifted into a proinflammatory phenotype by hyperglycemia. Mol. Med. 15:152–9.
Wenzel P, et al. (2008) Mechanisms underlying recoupling of eNOS by HMG-CoA reductase inhibition in a rat model of streptozotocin-induced diabetes mellitus. Atherosclerosis 198:65–76.
Blanco M, Rodriguez-Yánez M, Sobrino T, Leira R, Castillo J. (2005) Platelets, inflammation, and atherothrombotic neurovascular disease: the role of endothelial dysfunction. Cerebrovasc. Dis. 20 Suppl 2:S32–9.
Kiritoshi S, et al. (2003) Reactive oxygen species from mitochondria induce cyclooxygenase-2 gene expression in human mesangial cells: potential role in diabetic nephropathy. Diabetes 52:2570–7.
Kim SF, Huri DA, Snyder SH. (2005) Inducible nitric oxide synthase binds, S-nitrosylates, and activates cyclooxygenase-2. Science 310:1966–70.
Xu L, Han C, Lim K, Wu T. (2008) Activation of cytosolic phospholipase A2alpha through nitric oxide-induced S-nitrosylation: involvement of inducible nitric oxide synthase and cyclooxygenase-2. J. Biol. Chem. 283:3077–87.
Qi JS, Li YN, Zhang BS, Niu T, Liang JH. (2008) Peroxynitrite mediates high glucose-induced osteoblast apoptosis. J. Endocrinol. Invest. 31:314–20.
Ren XY, Li YN, Qi JS, Niu T. (2008) Peroxynitrite-induced protein nitration contributes to liver mitochondrial damage in diabetic rats. J. Diabetes Complications 22:357–64.
Taguchi K, Kobayashi T, Hayashi Y, Matsumoto T, Kamata K. (2007) Enalapril improves impairment of SERCA-derived relaxation and enhancement of tyrosine nitration in diabetic rat aorta. Eur. J. Pharmacol. 556:121–8.
Wu F, Wilson JX. (2009) Peroxynitrite-dependent activation of protein phosphatase type 2A mediates microvascular endothelial barrier dysfunction. Cardiovasc. Res. 81:38–45.
Zou MH. (2007) Peroxynitrite and protein tyrosine nitration of prostacyclin synthase. Prostaglandins Other Lipid Mediat. 82:119–27.
Robinson KM, Morré JT, Beckman JS. (2004) Triuret: a novel product of peroxynitrite-mediated oxidation of urate. Arch. Biochem. Biophys. 423:213–7.
Demicheli V, Quijano C, Alvarez B, Radi R. (2007) Inactivation and nitration of human superoxide dismutase (SOD) by fluxes of nitric oxide and superoxide. Free Radic. Biol. Med. 42:1359–68.
El-Remessy AB, et al. (2003) Experimental diabetes causes breakdown of the blood-retina barrier by a mechanism involving tyrosine nitration and increases in expression of vascular endothelial growth factor and urokinase plasminogen activator receptor. Am. J. Pathol. 162:1995–2004.
Garcia-Ruiz I, et al. (2006) Uric acid and anti-TNF antibody improve mitochondrial dysfunction in ob/ob mice. Hepatology 44:581–91.
Scott GS, Hooper DC. (2001) The role of uric acid in protection against peroxynitrite-mediated pathology. Med. Hypotheses 56:95–100.
Cosentino F, et al. (2003) High glucose causes up-regulation of cyclooxygenase-2 and alters prostanoid profile in human endothelial cells: role of protein kinase C and reactive oxygen species. Circulation 107:1017–23.
Zhang M, et al. (2006) Effects of eicosapentaenoic acid on the early stage of type 2 diabetic nephropathy in KKA(y)/Ta mice: involvement of anti-inflammation and antioxidative stress. Metabolism 55:1590–8.
St-Onge M, et al. (2007) Characterization of prostaglandin E2 generation through the cyclooxygenase (COX)-2 pathway in human neutrophils. Biochim. Biophys. Acta. 1771:1235–45.
Sheu ML, et al. (2005) High glucose induces human endothelial cell apoptosis through a phosphoinositide 3-kinase-regulated cyclooxygenase-2 pathway. Arterioscler. Thromb. Vasc. Biol. 25:539–45.
Shi Y, Vanhoutte PM. (2008) Oxidative stress and COX cause hyper-responsiveness in vascular smooth muscle of the femoral artery from diabetic rats. Br. J. Pharmacol. 154:639–51.
Chen YJ, Quilley J. (2008) Fenofibrate treatment of diabetic rats reduces nitrosative stress, renal cyclooxygenase-2 expression, and enhanced renal prostaglandin release. J. Pharmacol. Exp. Ther. 324:658–63.
Massi D, et al. (2009) Inducible nitric oxide synthase expression in melanoma: implications in lymphangiogenesis. Mod. Pathol. 22:21–30.
Amore A, et al. (2004) Amadori-configurated albumin induces nitric oxide-dependent apoptosis of endothelial cells: a possible mechanism of diabetic vasculopathy. Nephrol. Dial. Transplant. 19:53–60.
Zheng L, et al. (2007) Critical role of inducible nitric oxide synthase in degeneration of retinal capillaries in mice with streptozotocin-induced diabetes. Diabetologia 50:1987–96.
Inagi R, et al. (2006) A severe diabetic nephropathy model with early development of nodule-like lesions induced by megsin overexpression in RAGE/iNOS transgenic mice. Diabetes 55:356–66.
Pacher P, Szabo C. (2006) Role of peroxynitrite in the pathogenesis of cardiovascular complications of diabetes. Curr. Opin. Pharmacol. 6:136–41.
Vareniuk I, Pavlov IA, Obrosova IG. (2008) Inducible nitric oxide synthase gene deficiency counteracts multiple manifestations of peripheral neuropathy in a streptozotocin-induced mouse model of diabetes. Diabetologia 51:2126–33.
Obrosova IG, et al. (2007) Role of nitrosative stress in early neuropathy and vascular dysfunction in streptozotocin-diabetic rats. Am. J. Physiol. Endocrinol. Metab. 293:E1645–55.
Pacher P, Beckman JS, Liaudet L. (2007) Nitric oxide and peroxynitrite in health and disease. Physiol. Rev. 87:315–424.
Rachek LI, Musiyenko SI, LeDoux SP, Wilson GL. (2007) Palmitate induced mitochondrial deoxyribonucleic acid damage and apoptosis in l6 rat skeletal muscle cells. Endocrinology 148:293–9.
Xiao H, Li YN, Qi JS, Wang H, Liu K. (2009) Peroxynitrite plays a key role in glomerular lesion of diabetic rat. J. Nephrol. 22:800–8.
Beharka AA, Wu D, Serafini M, Meydani SN. (2002) Mechanism of vitamin E inhibition of cyclooxygenase activity in macrophages from old mice: role of peroxynitrite. Free Radic. Biol. Med. 32:503–11.
Cooke CL, Davidge ST. (2002) Peroxynitrite increases iNOS through NF-kappa B and decreases prostacyclin synthase in endothelial cells. Am. J. Physiol. Cell Physiol. 282:C395–402.
Acknowledgments
This study was supported by the Hebei Natural Science Foundation (C2009001092), the Bureau of Education of Hebei province (B2004122), the Bureau of Science and Technology of Hebei province (07276101D), the Bureau of Science and Technology of Shijiazhuang city (04146173A and 07120803a), the Bureau of Sanitation of Hebei province (04062) and Hebei Medical University (040028).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Li, Y., Qi, J., Liu, K. et al. Peroxynitrite-induced Nitration of Cyclooxygenase-2 and Inducible Nitric Oxide Synthase Promotes Their Binding in Diabetic Angiopathy. Mol Med 16, 335–342 (2010). https://doi.org/10.2119/molmed.2010.00034
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.2119/molmed.2010.00034