
Abstract
Objective
Little is known about the association between mental health and diminished food worry during the COVID-19 pandemic. This paper examines worry about having enough food to meet household needs and its association with mental health during the early months of the pandemic in Canada.
Methods
Data are drawn from the first round of a multi-round mental health monitoring survey. Online surveys were administered between May 14 and 29, 2020, to a nationally representative sample of Canadian adults (n = 3000). Logistic regression models were used to examine associations between food worry and mental health indicators (anxious/worried, depressed, worse mental health compared with pre-pandemic, and suicidal thoughts/feelings), after adjusting for socio-demographic characteristics and pre-existing mental health conditions. Fully adjusted models explored the impact of controlling for financial worry due to the pandemic in the previous 2 weeks.
Results
Overall, 17.3% of the sample reported food worry due to the pandemic in the previous 2 weeks, with the highest prevalence found among those with a reported disability (29.3%), Indigenous identity (27.1%), or pre-existing mental health condition (25.3%). Compared with participants who did not report food worry, those who did had higher odds of reporting feeling anxious/worried (OR=1.36, 95% CI: 1.08–1.71) and suicidal thoughts/feelings (OR=1.87, 95% CI: 1.24–2.80) when controlling for socio-demographics, pre-existing mental health conditions, and financial worry.
Conclusion
This paper provides insights about the associations between food worry and mental health in Canada during the COVID-19 pandemic and indicates the need for improved policies and social supports to mitigate food worry and associated mental health outcomes.
Résumé
Objectif
On en sait peu sur l’association entre la santé mentale et la diminution des inquiétudes liées à la nourriture durant la pandémie de COVID-19. Notre article porte sur l’inquiétude de ne pas avoir suffisamment de nourriture pour répondre aux besoins du ménage et son association avec la santé mentale au cours des premiers mois de la pandémie au Canada.
Méthode
Nos données proviennent du premier cycle d’une enquête de surveillance de la santé mentale. Des sondages en ligne ont été administrés entre le 14 et le 29 mai 2020 à un échantillon national représentatif de Canadiennes et de Canadiens adultes (n = 3 000). Des modèles de régression logistique ont servi à examiner les associations entre les inquiétudes liées à la nourriture et quelques indicateurs de santé mentale (anxiété/inquiétude, dépression, santé mentale pire qu’avant la pandémie, pensées/sentiments suicidaires) après l’apport d’ajustements pour tenir compte du profil sociodémographique et des troubles de santé mentale préexistants. À l’aide de modèles entièrement ajustés, nous avons exploré l’effet de la prise en compte des soucis financiers dus à la pandémie au cours des deux semaines antérieures.
Résultats
Dans l’ensemble, le pourcentage de l’échantillon ayant fait état d’inquiétudes liées à la nourriture dues à la pandémie au cours des deux semaines antérieures était de 17,3 %, la plus forte prévalence ayant été constatée chez les répondants ayant un handicap déclaré (29,3 %), une identité autochtone (27,1 %) ou un trouble de santé mental préexistant (25,3 %). Comparativement aux participants n’ayant fait état d’aucune inquiétude liée à la nourriture, ceux qui ont fait état de telles inquiétudes présentaient une plus forte probabilité d’avoir déclaré des sentiments d’anxiété ou d’inquiétude (RC = 1,36, IC de 95 % : 1,08-1,71) et des pensées ou sentiments suicidaires (RC = 1,87, IC de 95 % : 1,24-2,80) après la prise en compte du profil sociodémographique, des troubles de santé mentale préexistants et des soucis financiers.
Conclusion
Notre article jette un éclairage sur les associations entre les inquiétudes liées à la nourriture et la santé mentale au Canada durant la pandémie de COVID-19 et montre qu’il faudrait améliorer les politiques et les mesures de soutien social pour atténuer les inquiétudes liées à la nourriture et les résultats de santé mentale associés.
Similar content being viewed by others


Introduction
Food insecurity, defined as inadequate or insecure access to food due to financial constraints (Tarasuk & Mitchell, 2020), is a critical public health challenge associated with substantial negative impacts on physical, social, and emotional well-being; nutritional vulnerability; and mortality risk (Jessiman-Perreault & McIntyre, 2017; Tarasuk et al., 2018; Tarasuk & Mitchell, 2020). Growing evidence also suggests that food insecurity is associated with major depressive episodes, depressive thoughts, anxiety disorders, mood disorders, stress, and suicidal thoughts and behaviours (Ju et al., 2016; Koyanagi et al., 2019; Pourmotabbed et al., 2020). Over 4.4 million people (12.7% of households) in Canada reported some level of food insecurity in the previous year on the 2017–2018 Canadian Community Health Survey (CCHS), the highest rate recorded since national monitoring began (Tarasuk & Mitchell, 2020). Emerging evidence suggests that the COVID-19 pandemic has resulted in both worsened food access (Ahn & Norwood, 2020; Fitzpatrick et al., 2020; Niles et al., 2020; Statistics Canada, 2020c) and mental health stressors (Flentje et al., 2020; Jenkins et al., 2021; Katz, 2020), with growing need to understand the prevalence, predictors, and associations between them, including the need to more closely examine and inform approaches to best support population-level mental health.
Conceptualized along a spectrum, milder forms of food insecurity are characterized by worry, anxiety, and/or uncertainty about access to food, while moderate and the most severe forms incorporate compromised quality and quantity of food intake (Nord et al., 2016; Tarasuk & Mitchell, 2020). Recent research identifies the notion of food worry as a potential determinant of health in its own right (Kousoulis et al., 2020). The worry that food may run out before there is money to get more or having limited selection due to financial concerns (Tarasuk & Mitchell, 2020) has been used to characterize a milder/“marginal” form of food insecurity. Significantly, the pandemic has triggered income shocks through workforce layoffs, lost work hours, workers’ illnesses, and quarantine orders. Moreover, national data suggest that both the prevalence of food insecurity (Men & Tarasuk, 2021) and rates of mental health concerns (Campion et al., 2020; Jenkins et al., 2021; Polsky & Gilmour, 2020) have risen substantially. Studies from multiple countries suggest that worry about access to food is often a precursor to reductions in the quality or variety of foods consumed and an early predictor of more severe forms of food insecurity (Coates et al., 2006; Knowles et al., 2016).
However, food worry is not always related to finances. Experiences commonly reported during the COVID-19 pandemic suggest that there are a variety of conditions that can impact access to and worry about food. For example, data from early in the pandemic illustrate growth in total sales of groceries, especially large increases in purchases of non-perishable foods (Statistics Canada, 2020a). In the United States (USA), there was widespread speculation of a “fractured food supply chain” early in the pandemic, which may have exacerbated anxiety and other mental health challenges (e.g., hoarding, panic-shopping) (Fitzpatrick et al., 2020, p. 2). Similarly, in Canada, the pandemic and its secondary effects have contributed to worry and stress about food (Taylor et al., 2020). Further in the early months of the pandemic, there were concerns about potential virus transmission via food and its packaging or while grocery shopping, as well as substantial grocery delivery service delays (Rizou et al., 2020).
Though food worry is a core component of food insecurity measurement, limited research has examined the prevalence or associations of food worry with mental health, particularly in the context of COVID-19. The purpose of this paper is therefore to describe the prevalence and correlates of food worry, and to examine the associations between this experience and indicators of mental health during the COVID-19 pandemic in Canada after controlling for other known socio-demographic predictors of mental health.
Methods
Data collection
This study utilizes data from the first round of a multi-round national monitoring survey, Assessing the Impacts of COVID-19 on Mental Health, which examines broad mental health impacts of the COVID-19 pandemic among individuals aged 18 years and older living in Canada (Jenkins et al., 2021). This study was conducted in partnership between researchers at the University of British Columbia, the Canadian Mental Health Association (CMHA), and the United Kingdom-based Mental Health Foundation.
Data collection was achieved through an online survey distributed from May 14 to 29, 2020, by national polling vendor Maru/Matchbox, which manages the Maru Voice Canada panel consisting of approximately 125,000 Canadian adults. Maru/Matchbox randomly invited panel members to anonymously participate based on Canadian national census-informed stratifications defined by socio-demographic characteristics (age, gender, household income, provincial region), with adjustments made for response propensity. Response-to-invitation ratio was 32% during this survey round. The survey was available in English and French and the time period corresponded with the initial “re-opening” that occurred across Canada following 2 months of widespread restrictions, including school closures, work from home orders, and business shutdowns.
Survey items were informed by a survey commissioned by the Mental Health Foundation in March 2020 and included consultation with people with diverse experiences, including mental health conditions (Kousoulis et al., 2020). The survey was subsequently adapted, in collaboration with the CMHA, to reflect the Canadian context. Survey items are provided as Supplementary Material.
Key variables
Food worry was assessed by asking “Have you been stressed or worried about any of the following as a result of the COVID-19 pandemic in the past 2 weeks?” with one response option being “having enough food to meet my household’s basic needs”. This item was developed by the Mental Health Foundation (Kousoulis et al., 2020) to facilitate cross-country comparisons. Respondents could select “Yes”, “No”, or “Don’t know/Not applicable/Prefer not to say”. Respondents who selected the third option (n = 97) were excluded from this analysis to facilitate clear comparisons between those who did and those who did not endorse food worry. Thus, a subsample of 2903 participants were included in this analysis.
Study outcomes included several mental health indicators. Participants reported emotional responses related to the pandemic in the previous 2 weeks, including feeling depressed and feeling anxious or worried. To assess perceived changes to mental health, participants were asked, “Compared to before the COVID-19 pandemic and related restrictions in Canada, how would you say your mental health is now?” Responses of “Slightly worse now” and “Significantly worse now” were combined into a single “Worse mental health” outcome category. Last, suicidal ideation was assessed by asking whether participants “Experienced suicidal thoughts/feelings” in the previous 2 weeks as a result of the pandemic.
Socio-demographic characteristics measured included age, gender (female or male), annual household income, Indigenous identity, parent/guardian of a minor in the household, disability status, and LGBT2Q+ (lesbian, gay, bisexual, transgender, two-spirit, queer, etc.) identity. Pre-existing (prior to the COVID-19 pandemic) mental health conditions and feeling stress/worry related to financial concerns in the past 2 weeks were examined as likely confounders.
Data analysis
Across analyses, p-values ≤ 0.05 were considered statistically significant. Descriptive statistics and chi-squared tests were used to examine the prevalence of food worry in the past 2 weeks for the full sample and by socio-demographic and mental health variables. A three-step logistic regression modelling approach was used to examine the associations between food worry and each of the four mental health indicators. First, unadjusted models were examined. Second, multivariable logistic regression models, which also included potentially confounding factors (gender, age, household income, Indigenous identity, children in household, disability, LGBT2Q+ identity, and pre-existing mental health conditions), were conducted. In the third and final step, financial worry in the previous 2 weeks as a result of the pandemic was added to the fully adjusted multivariable models. All analyses were performed using SPSS version 25.
Ethics
Ethical approval for this study was obtained from the University of British Columbia Behavioural Research Ethics Board (H20-01273). In advance of commencing the survey, participants provided consent online. Participants were provided with information about accessing mental health supports and received a small honorarium from Maru/Matchbox.
Results
Overall, 2903 participants were included in this analysis, with 50.8% of the sample identifying as female, 3.0% identifying as Indigenous, and 7.5% reporting a household income of less than $25K (see Table 1). Additionally, 18.4% of participants reported a pre-existing mental health condition and 37.3% reported financial worry in the previous 2 weeks. Seventeen percent of respondents (n = 503) indicated stress or worry about having enough food to meet their household’s basic needs in the previous 2 weeks as a result of the COVID-19 pandemic, while 82.7% (n = 2400) did not report this worry. Food worry was more commonly reported among those who: were younger, were Indigenous, were parents/guardians, had low household incomes, reported a pre-existing mental health condition, or had financial worry in the previous 2 weeks.
Mental health indicators are described in Table 2. A total of 45.8% of respondents reported feeling anxious or worried, and 22.6% felt depressed in the previous 2 weeks. Furthermore, 37.4% reported having worse mental health as compared with before the COVID-19 pandemic, while 5.9% reported experiencing suicidal thoughts/feelings as a result of the pandemic in the past 2 weeks. The prevalence of reporting feeling anxious/worried, depressed, having worse mental health, and experiencing suicidal thoughts/feelings was all higher among those reporting food worry than among those who did not (p < 0.001).
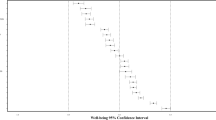
Table 3 presents the results from the unadjusted and multivariable regression models, with results presented as odds ratios and 95% confidence intervals. Food worry was significantly associated with higher odds of all mental health indicators examined in the unadjusted models from the first step of the modelling process. Compared with those without food worry, those who reported food worry had higher odds of feeling anxious or worried (OR = 1.95, 95% CI: 1.60, 2.37), feeling depressed (OR = 2.00, 95% CI: 1.62, 2.47), identifying worse mental health (OR = 1.92, 95% CI: 1.59, 2.34), and over triple the odds of experiencing suicidal thoughts/feelings (OR = 3.31, 95% CI: 2.39, 4.58).
The effect size of the associations between food worry and mental health outcomes decreased but remained statistically significant for all four outcomes after adding socio-demographic characteristics and reporting a pre-existing mental health condition to the models in the second modelling step. Specifically, the odds ratios associated with food worry were 1.76 (95% CI: 1.42, 2.19) for feeling anxious or worried, 1.62 (95% CI: 1.27, 2.05) for feeling depressed, 1.66 (95% CI: 1.34, 2.06) for worse mental health, and 2.25 (95% CI: 1.54, 3.30) for experiencing suicidal thoughts/feelings.
The magnitude of associations between food worry with mental health outcomes further decreased after adding financial worry to the models, alongside the socio-demographic characteristics and pre-existing mental health in the third and final modelling step. The association between food worry and feeling anxious or worried remained statistically significant in the fully adjusted models, with an odds ratio of 1.36 (95% CI: 1.08, 1.71). Similarly, the magnitude of the relation between food worry and experiencing suicidal thoughts/feelings remained statistically significant but was weakened with an odds ratio of 1.87 (95% CI: 1.24, 2.80). However, the relation between food worry and feeling depressed was no longer statistically significant (OR = 1.25, 95% CI: 0.97, 1.61), nor was the relationship between food worry and reporting worse mental health (OR = 1.26, 95% CI: 1.00, 1.59) in the final models.
Discussion
Food worry—the experience of stress or worry about having enough food to meet basic needs—is an emerging secondary effect of social interventions needed to reduce the spread of the COVID-19 virus. This study adds to the growing body of research on food worry and indicates that 17.3% of Canadian adults were concerned about having enough food to meet their household’s basic needs in the early months of the pandemic. This aligns with data collected by Statistics Canada during the week prior to this survey, which found that 14.6% of Canadians experienced some level of food insecurity during the previous 30 days (Polsky & Gilmour, 2020; Statistics Canada, 2020c). Comparisons with national data collected pre-pandemic suggest that the level of food worry and food insecurity was likely higher early in the pandemic than beforehand. For example, in the 2017–2018 CCHS Household Food Security Survey Model (HFSSM), 12.7% of households in Canada indicated any level of food insecurity within the previous year (Tarasuk & Mitchell, 2020).
Findings from our study also inform understandings about the inequitable distribution of food worry in Canada. Specifically, younger adults, parents of young children, those with low household income, individuals who identify as Indigenous, those who live with a disability or pre-existing mental health condition, or those who experienced financial worry within the previous 2 weeks were more likely to report food worry. Our findings align with the wider food security literature both preceding and emerging from the pandemic era showing that risk of experiencing food insecurity, including the most severe forms, is inequitably distributed across society (Boyraz & Legros, 2020; Deaton & Deaton, 2020; Tarasuk & Mitchell, 2020). For example, during the COVID-19 pandemic, a report on food insecurity in the USA found that between April and May 2020, households with children, larger households, and racialized people were more likely to be food insecure compared with other groups (Niles et al., 2020).
Supporting previously identified associations between food security and mental health (Elgar et al., 2020; Tarasuk et al., 2018), we found associations between food worry and both suicidal ideation and self-reported mental health during the pandemic in unadjusted models. While limited research has examined these associations in the COVID-19 context, a recent US study identified that those experiencing food insecurity during the pandemic indicated higher rates of suicidal ideation (Fitzpatrick et al., 2020). Furthermore, in the unadjusted results from our study, participants who reported food worry also reported being nearly twice as likely to report feeling anxious/worried and depressed due to the pandemic in the previous 2 weeks.
Results from the partially adjusted models further suggest that food worry is independently associated with worsened mental health beyond the effects of income, pre-existing mental health conditions, and other socio-demographic factors. While food worry is only one of several components that comprise the larger construct of food insecurity, these findings are consistent with Statistics Canada’s 2020 data collected during the pandemic, indicating that 45.3% of participants from moderately food-insecure households and 51.0% from severely food-insecure households perceived their mental health as “fair” or “poor” compared with 22.0% of those in food-secure households (Polsky & Gilmour, 2020).
One finding of note was that adding financial worry in the previous 2 weeks due to the pandemic as a covariate, alongside other socio-demographic characteristics, reduced the magnitude of the food worry coefficients across all models and resulted in non-significance for the associations between food worry and worse mental health and food worry and feeling depressed. While lessened, the effect sizes of the relations between food worry and suicidal thoughts and feeling anxious/worried remained statistically significant, and considerable in magnitude. The fact that adding financial worry to the model reduced but did not completely eliminate the relationship between food worry and suicidal thoughts/worries and anxious/worried feelings suggests that food worry may be associated with mental health through financial worry, as well as independently associated with some mental health indicators. However, directionality cannot be determined given the cross-sectional nature of our data.
Given that the rate of food worry among those reporting financial worry was 33.5%, compared with 7.6% among those who did not report financial worry, our findings suggest that food worry was more prevalent among, although not necessarily limited to, households experiencing COVID-19-related income shocks and other financial concerns. This is a finding that aligns with previous household food security literature (Deaton et al., 2019; Tarasuk & Mitchell, 2020) as well as Canadian and US COVID-19 studies (Ahn & Norwood, 2020; Polsky & Gilmour, 2020). Niles et al. (2020) reported that during the pandemic, food-insecure households in the USA were more likely to include an individual who had been furloughed, seen a reduction in hours, or lost their job since the start of the pandemic compared with food-secure households. Still, even after controlling for financial concerns, food worry was associated with higher odds of suicidal thoughts/feelings, and our findings show that food worry was reported by 12% of participants with annual household incomes over $100K per year. These findings and the robustness of the association of food worry with suicidal thoughts/feelings, while controlling for a set of potentially confounding variables, indicate there may be a robust association between non-financial food worry and some indicators of mental health during COVID-19. These worries could be related to lack of food availability in grocery stores, worries about food safety due to potential virus contamination, insufficient food quantities, and inability to physically distance from others while shopping.
Emerging evidence indicates that ensuring a guaranteed livable income could contribute to ensuring that Canadians could worry less about accessing food due to financial concerns (Tarasuk et al., 2018). While sufficient income and access to adequate food are necessary conditions for reducing food worry, this study suggests further need to ensure that people are connected to sufficient social supports, resources, and accurate information to address their food-related needs and mental health. This includes ensuring stable and secure access to food and acknowledging the deep-rooted and intersecting inequities related to race, class, pre-existing disability, and mental health experiences.
Strengths and limitations
This paper utilized data from a large, nationally representative sample to examine the mental health impacts of the COVID-19 pandemic in relation to food worry, an underexplored component of the wider food insecurity literature. Sampling design ensured participation from people of diverse backgrounds and those typically under-represented in research. While our data were representative of the Canadian population for age, gender, region, and income (Statistics Canada, 2020b), other characteristics may not have been representative. Strategies did include oversampling and community partnerships to minimize selection bias and reduce technology barriers; however, it is possible that survey respondents and non-respondents differed on key measures including underrepresentation of racial and ethnic groups, few responses from people who live in the territories, and possible internet access issues (Statistics Canada, 2019).
Notable limitations also include the cross-sectional nature of this study survey which cannot determine causal pathways or potential bidirectionality of associations, as poor mental health also likely contributes to additional food worry. Furthermore, the purpose of this study was to examine associations between food worry, socio-demographic characteristics, and mental health; however, the analysis did not control for or analyze whether respondents experienced food worry either before or unrelated to the pandemic. Similarly, analysis for suicidal ideation focused on this experience as related to the pandemic, thus potentially missing suicidal ideation that the respondent did not attribute to pandemic effects. This study did not measure the prevalence of specific mental health outcomes or include clinical assessments of mental illness. This study also did not take into account baseline measures of mental health and was specific to the Canadian context during the first re-opening phase of the COVID-19 pandemic. Finally, the food worry item used in our survey was initially developed and used for pandemic research in the UK which informed this investigation in order to perform cross-national comparisons (Kousoulis et al., 2020). However, the question is not derived from a validated household food security scale, and therefore, cannot be used to make direct comparisons with food insecurity data. In order to more robustly identify marginal food insecurity in the Canadian context, we have since added a question from the Canadian HFSSM to subsequent survey rounds, allowing for future comparisons of these measures. Notably, the framing of a tool such as the Canadian HFSSM focuses on financial causes of food insecurity (Bush, 2007), potentially “excluding” households experiencing food worry for non-financial reasons. Research is needed to further examine the various factors that drive food worry and their intersections to inform a comprehensive response to mitigate this worry and broader experiences of food insecurity at the population level, as well as to better tease apart causal mechanisms and pathways.
Conclusion
The long-term impacts to population-level mental health challenges and food insecurity due to the COVID-19 pandemic are projected to have profound effects on millions of people worldwide for many years to come. Our findings suggest that the COVID-19 pandemic may have contributed to high levels of food worry across Canada, which were associated with negative mental health outcomes, including increased suicidal ideation, even after controlling for the potentially confounding effects of financial worries due to the pandemic, low income, and pre-existing mental health challenges. Worrying about having sufficient access to food may, in its own right, be a useful indicator for better understanding the early impacts of the COVID-19 pandemic in Canada. Future research is needed to explore how this food worry construct differs from validated measures of marginal food insecurity and to more broadly evaluate how improved social policies, such as a guaranteed livable income and supports that ensure adequate and secure food access, can reduce further population-level mental health consequences.
Contributions to knowledge
What does this study add to existing knowledge?
-
Our findings suggest that the COVID-19 pandemic may have contributed to high levels of food worry across Canada, associated with negative mental health outcomes, including increased suicidal ideation.
-
This demonstrates the link between access to food and population mental health, and further identifies the need for proactive policy solutions.
What are the key implications for public health interventions, practice or policy?
-
Future research is needed to more broadly evaluate how improved social policies, such as a guaranteed livable income, built environmental adjustments, and supports that ensure adequate and secure food access, can reduce further population-level mental health consequences.
Data Availability
Data are available upon reasonable request from the corresponding author.
References
Ahn, S., & Norwood, F. B. (2020). Measuring food insecurity during the COVID-19 pandemic of spring 2020. Applied Economic Perspectives and Policy, 1–7.
Boyraz, G., & Legros, D. N. (2020). Coronavirus disease (COVID-19) and traumatic stress: Probable risk factors and correlates of posttraumatic stress disorder. Journal of Loss and Trauma, 1–20.
Bush, M. (2007). Canadian Community Health Survey, Cycle 2.2, Nutrition (2004): Income-Related Household Food Security in Canada. In: Health Canada, Ottawa, Canada.
Campion, J., Javed, A., Sartorius, N., & Marmot, M. (2020). Addressing the public mental health challenge of COVID-19. The Lancet. Psychiatry.
Coates, J., Frongillo, E. A., Rogers, B. L., Webb, P., Wilde, P. E., & Houser, R. (2006). Commonalities in the experience of household food insecurity across cultures: What are measures missing? The Journal of Nutrition, 136(5), 1438S–1448S.
Deaton, B. J., & Deaton, B. J. (2020). Food security and Canada's agricultural system challenged by COVID-19. Canadian Journal of Agricultural Economics/Revue canadienne d’agroéconomie, 1–7
Deaton, B. J., Scholz, A., & Lipka, B. (2019). An empirical assessment of food security on First Nations in Canada. Canadian Journal of Agricultural Economics/Revue canadienne d’agroéconomie, 68(1), 5–19
Elgar, F. J., Pickett, W., Pförtner, T.-K., Gariépy, G., Gordon, D., Georgiades, K., . . . Da Silva, M. A. (2020). Relative food insecurity, mental health and wellbeing in 160 countries. Social Science & Medicine, 113556.
Fitzpatrick, K. M., Harris, C., & Drawve, G. (2020). How bad is it? Suicidality in the middle of the COVID-19 pandemic. Suicide and Life-threatening Behavior, 50(6), 1241–1249.
Flentje, A., Obedin-Maliver, J., Lubensky, M. E., Dastur, Z., Neilands, T., & Lunn, M. R. (2020). Depression and anxiety changes among sexual and gender minority people coinciding with onset of COVID-19 pandemic. Journal of General Internal Medicine, 35(9), 2788–2790.
Jenkins, E. K., McAuliffe, C., Hirani, S., Richardson, C., Thomson, K. C., McGuinness, L., . . . Gadermann, A. (2021). A portrait of the early and differential mental health impacts of the COVID-19 pandemic in Canada: Findings from the first wave of a nationally representative cross-sectional survey. Preventive Medicine, 106333.
Jessiman-Perreault, G., & McIntyre, L. (2017). The household food insecurity gradient and potential reductions in adverse population mental health outcomes in Canadian adults. Social Science and Medicine Population Health, 3, 464–472.
Ju, Y. J., Park, E.-C., Han, K.-T., Choi, J. W., Kim, J. L., Cho, K. H., & Park, S. (2016). Low socioeconomic status and suicidal ideation among elderly individuals. International Psychogeriatrics, 28(12), 2055–2066.
Katz, B. (2020). Mood symptoms predict COVID-19 pandemic distress but not vice versa: An 18-month longitudinal study. Retrieved from osf.io/sjp4a
Knowles, M., Rabinowich, J., De Cuba, S. E., Cutts, D. B., & Chilton, M. (2016). “Do you wanna breathe or eat?”: Parent perspectives on child health consequences of food insecurity, trade-offs, and toxic stress. Maternal and Child Health Journal, 20(1), 25–32.
Kousoulis, A., McDaid, S., Crepaz-Keay, D., Solomon, S., Lombardo, C., Yap, J., . . . Davidson, G. (2020). The COVID-19 pandemic, financial inequality and mental health. Retrieved from UK: https://www.mentalhealth.org.uk/sites/default/files/MHF-covid-19-inequality-mental-health-briefing.pdf
Koyanagi, A., Stubbs, B., Oh, H., Veronese, N., Smith, L., Haro, J. M., & Vancampfort, D. (2019). Food insecurity (hunger) and suicide attempts among 179,771 adolescents attending school from 9 high-income, 31 middle-income, and 4 low-income countries: A cross-sectional study. Journal of Affective Disorders, 248, 91–98.
Men, F., & Tarasuk, V. (2021). Food insecurity amid the COVID-19 pandemic: Food charity, government assistance and employment. Canadian Public Policy, e2021001.
Niles, M. T., Bertmann, F., Morgan, E. H., Wentworth, T., Biehl, E., & Neff, R. (2020). The impact of coronavirus on Vermonters experiencing food insecurity. College of Agriculture and Life Sciences Faculty Publications, 9 Retrieved from https://scholarworks.uvm.edu/calsfac/19.
Nord, M., Cafiero, C., & Viviani, S. (2016). Methods for estimating comparable prevalence rates of food insecurity experienced by adults in 147 countries and areas. Journal of Physics: Conference Series, 772, 012060.
Polsky, J., & Gilmour, H. (2020). Food insecurity and mental health during the COVID-19 pandemic. Statistics Canada Health Reports, 31(12), 1–11 Retrieved from https://www150.statcan.gc.ca/n1/en/pub/82-003-x/2020012/article/00001-eng.pdf?st=-I-nE_ko.
Pourmotabbed, A., Moradi, S., Babaei, A., Ghavami, A., Mohammadi, H., Jalili, C., et al. (2020). Food insecurity and mental health: A systematic review and meta-analysis. Public Health Nutrition, 23(10), 1778–1790.
Rizou, M., Galanakis, I. M., Aldawoud, T. M., & Galanakis, C. M. (2020). Safety of foods, food supply chain and environment within the COVID-19 pandemic. Trends in Food Science & Technology, 102, 293–299.
Statistics Canada. (2019). Canadian Internet Use Survey. Retrieved from https://www150.statcan.gc.ca/n1/daily-quotidien/191029/dq191029a-eng.htm
Statistics Canada. (2020). Food insecurity during the COVID-19 pandemic, May 2020. Retrieved from https://www150.statcan.gc.ca/n1/pub/45-28-0001/2020001/article/00039-eng.htm
Statistics Canada. (2020a). Canadian consumers prepare for COVID-19. Retrieved from https://www150.statcan.gc.ca/n1/pub/62f0014m/62f0014m2020004-eng.htm
Statistics Canada. (2020b). Data Products, 2016 Census. Retrieved from https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/index-eng.cfm
Tarasuk, V., & Mitchell, A. (2020). Household food insecurity in Canada (pp. 2017–2018). Research to identify policy options to reduce food insecurity. Retrieved from PROOF https://proof.utoronto.ca/.
Tarasuk, V., Cheng, J., Gundersen, C., de Oliveira, C., & Kurdyak, P. (2018). The relation between food insecurity and mental health care service utilization in Ontario. The Canadian Journal of Psychiatry, 63(8), 557–569.
Taylor, S., Landry, C. A., Paluszek, M. M., Fergus, T. A., McKay, D., & Asmundson, G. J. (2020). COVID stress syndrome: Concept, structure, and correlates. Depression and Anxiety, 37(8), 706–714.
Acknowledgements
We are appreciative of the support and partnership we received in mobilizing this project from the Canadian Mental Health Association and Mental Health Foundation in the UK. Special thanks to Katherine Janson and Margaret Eaton (Canadian Mental Health Association) for facilitating study communications and government relations outreach, and to Jacqueline Campbell, Neesha Mathew, and Stacey Kinley (Maru/Matchbox) for supporting survey deployment and data preparation. Jennifer Black received support from the University of British Columbia Peter Wall Institute for Advanced Study at the time of this study. EJ and AG both hold Scholar Awards from the Michael Smith Foundation for Health Research, which has supported their time contributions to the study.
Code availability
Not applicable.
Funding
The Canadian Mental Health Association (CMHA) funded survey data collection through national polling vendor Maru/Matchbox.
Author information
Authors and Affiliations
Contributions
EJ, CM, and AG led the conceptualization of the study, including study design and data collection. CM, ZD, JP, and CR led the analysis, interpretation, and writing of this manuscript. JB, AG, AS, KT, and EJ further contributed to the data interpretation and writing of this manuscript.
Corresponding author
Ethics declarations
Ethics approval
Ethical approval for this study was obtained from the University of British Columbia Behavioural Research Ethics Board (H20-01273).
Consent to participate
In advance of commencing the survey, participants provided consent online. Participants were provided with information about accessing mental health supports and received a small honorarium from Maru/Matchbox.
Consent for publication
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(PDF 177 kb)
Rights and permissions
About this article

Cite this article
McAuliffe, C., Daly, Z., Black, J. et al. Examining the associations between food worry and mental health during the early months of the COVID-19 pandemic in Canada. Can J Public Health 112, 843–852 (2021). https://doi.org/10.17269/s41997-021-00557-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.17269/s41997-021-00557-w