
Abstract
OBJECTIVE
Previous neck surgery (PNS) in patients with primary hyperparathyroidism (PHP) is considered as a contraindication for minimally invasive parathyroidectomy (MIP). The purpose of our study was to determine the effectiveness of MIP in such patients.
DESIGN
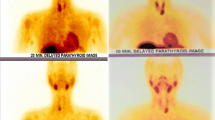
From January 2003 to June 2011, 380 patients with PHP were treated in our department; 42 had had previous neck surgery. Twenty-seven (27/42) were selected to have MIP; the remaining 15 patients had traditional neck explorations. Selection criteria for MIP were unilateral single or two gland disease localized preoperatively with at least two imaging techniques and patient’s informed consent. Imaging studies included high resolution neck ultrasound and sestamibi scan in the majority, and CT scan, selective venous sampling and MRI in seven patients. The type of operation done included unilateral approach under local anesthesia (UALA) (22 cases) with one conversion to general anesthesia and minimally invasive parathyroidectomy under general anesthesia (MIPG) (5 cases).
RESULTS
Twenty-six of the 27 patients became normocalcemic after the operation. The patient with persistent hypercalcemia underwent successful parathyroidectomy 8 months later via mesothoracoscopy, since the parathyroid gland was localized correctly but was beyond access via neck. A single adenoma was found in 21 cases and hyperplasia in six. There were no conversions to traditional exploration and no postoperative complications. Mean duration of the procedure and length of stay were similar to MIP in patients without PNS. Mean follow-up of 40 months (4–89 months) did not reveal any recurrence.
CONCLUSION
These results illustrate that MIP is a valuable option in selected patients with PHP and PNS associated with no morbidity (0%), high biochemical cure rate (96.3% in this series) and rapid recovery, while it also substantially lowers the cost of the procedure. Preoperative localization with two or more agreeing imaging techniques eliminates the need for intraoperative sestamibi or qPTH test.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Inabnet WB, Fulla Y, Richard B, Bonnichon P, Icard P, Chapuis Y, 1999 Unilateral neck exploration under local anesthesia: the approach of choice for asyptomatic primary hyperparathyroidism. Surgery 126: 1004–1009.
Chapuis Y, 2003 New directions in the surgical treatment of primary hyperparathyroidism. Bull Acad Natl Med 187: 493–502.
Barczynski M, 2009 Minimally invasive parathyroidectomy without intraoperative parathyroid hormone monitoring: When and why? J Postgrad Med 55: 239–240.
Pang T, Stalberg P, Sidhu S, et al, 2007 Minimally invasive parathyroidectomy using the lateral focused mini-incision technique without intraoperative parathyroid hormone monitoring. Br J Surg 94: 315–319.
Haciyanli M, Genc H, Damburaci N, Oruk G, Tutuncuoglu P, Erdogan N, 2009 Minimally invasive focused parathyroidectomy without using intraoperative parathy-roid hormone monitoring or gamma probe. J Postgrad Med 55: 242–246.
Thakur A, Sebag F, Slotema E, Ippolito G, Taϊeb D, Henry JF, 2009 Significance of biochemical parameters in differentiating uniglandular from multiglandular disease and limiting use of intraorerative parathormone assay. World J Surg 33: 1219–1223.
Quiros R, Alioto J, Wilhelm S, Ali A, Prinz R, 2004 An algorithm to maximize use of minimally invasive parathyroidectomy. Arch Surg 139: 501–507.
Ghaheri BA, Koslin DB, Wood AH, Cohen JL, 2004 Preoperative ultrasound is worthwhile for reoperative parathyroid surgery. Laryngoscope 114: 2168–2171.
Henry Jean-François, 2010 Reoperation for primary hyperparathyroidism: tips and tricks. Langenbecks Arch Surg 395: 103–109.
Gawande AA, Monchik JM, Abbruzzese TA, Iannuccilli JD, Ibrahim SI, Moore FD Jr, 2006 Reassessment of parathyroid hormone monitoring during parathyroidectomy for primary hyperparathyroidism after 2 preoperative localization studies. Arch Surg 141: 381–384.
Stalberg P, Sidhu S, Sywak M, Robinson B, Wilkinson M, Delbridge L, 2006 Intraoperative parathyroid hormone measurement during minimally invasive parathyroid-ectomy: does it “value-add” to decision-making? J Am Coll Surg 203: 1–6.
Gil-Cardenas A, Gamino A, Reza A, Pantoja JP, Herrera MF, 2007 Is intraoperative parathyroid hormone assay mandatory for the success of targeted parathyroidectomy? J Am Coll Surg 204: 286–290.
Mihai R, Palazzo FF, Gleeson FV, Sadler GP, 2007 Minimally invasive parathyroidectomy without intra-operative parathyroid hormone monitoring in patients with primary hyperparathyroidism. Br J Surg 94: 42–47.
Rotstein L, Irish J, Gullane P, Keller MA, Sniderman K, 1998 Reoperative parathyroidectomy in the era of localization technology. Head Neck 20: 535–539.
Norman J, Denham D, 1998 Minimally invasive radioguided parathyroidectomy in the reoperative neck. Surgery 124: 1088–1092.
Barczynski M, Golkowski F, Konturek A, et al, 2006 Technetium-99m-sestamibi subtraction scintigraphy vs. ultrasonography combined with a rapid parathyroid hormone assay in parathyroid aspirates in preoperative localization of parathyroid adenomas and in directing surgical approach. Clin Endocrinol (Oxf) 65: 106–113.
Barczynski M, Konturek A, Cichon S, Hubalewska-Dydejczyk A, Golkowski F, Huszno B, 2007 Intraoperative parathyroid hormone assay improves outcomes of minimally invasive parathyroidectomy mainly in patients with a presumed solitary parathyroid adenoma and missing concordance of preoperative imaging. Clin Endocrinol (Oxf) 66: 878–885.
Udelsman R, 2011 Approach to the patient with persistent or recurrent primary hyperparathyroidism. J Clin Endocrinol Metab 96: 2950–2958.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dimas, S., Michas, S., Christakis, I. et al. Minimally invasive parathyroidectomy in patients with previous neck surgery. Hormones 11, 160–165 (2012). https://doi.org/10.14310/horm.2002.1343
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.14310/horm.2002.1343