
Abstract
OBJECTIVE
Hypopituitarism is a recognized complication of Traumatic Brain Injury (TBI). Resolution of established anterior pituitary hormones deficiency is rare.
CASE REPORT
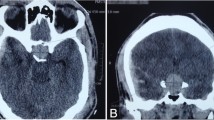
A woman was initially presented at the age of 22 years with amenorrhoea. Two years earlier she had been involved in a car accident with consequent TBI. At our evaluation, serum oestradiol (E2) was low (3 pmol/l), Luteinizing Hormone (LH) and Follicle Stimulating Hormone (FSH) were borderline low [1.7 and 2.5 mIU/l, normal range (NR) for 20–35 yr old women being 1.4–13 and 2.5–13, respectively] with poor response to Gonadotropin Releasing Hormone (GnRH) (ΔLH = 2.4 and, ΔFSH = 4.0 mIU/l), while serum Prolactin (PRL) was elevated (951 mIU/l; NR: 102-496). No other pituitary hormone deficiencies were observed. Magnetic resonance imaging (MRI) showed a partially empty sella and very thin stalk. Ten years later a new endocrine evaluation was performed. On day 4 of her menstrual cycle, serum values of PRL (196 mIU/l), FSH (4.7 mIU/l), LH (4.8 mIU/l) and E2 (103 pmol/l) were within normal limits for women aged 20–35. Six months after this evaluation (that is, 12 years after trauma), the patient became pregnant and delivered a healthy baby.
CONCLUSIONS
Our case shows that spontaneous resolution of post-head trauma anterior hypopituitarism occur even many years after head injury. Medicolegal implications are self-evident.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Benvenga S, Campenní A, Ruggeri RM, Trimarchi F, 2000 Hypopituitarism secondary to head trauma. J Clin Endocrinol Metab 85: 1353–1361.
Schneider HJ, Aimaretti G, Kreitschmann-Andermahr I, Stalla GK, Ghigo E, 2007 Hypopituitarism. Lancet 369: 1461–1470.
Agha A, Rogers B, Sherlock M, et al, 2004 Anterior pituitary dysfunction in survivors of traumatic brain injury. J Clin Endocrinol Metab 89: 4929–4936.
Kreitschmann-Andermahr I, Hoff C, Saller B, et al, 2004 Prevalence of pituitary deficiency in patients after aneurysmal subarachnoid hemorrhage. J Clin Endocrinol Metab 89: 4986–4992.
Benvenga S, 2005 Brain injury and hypopituitarism: the historical background. Pituitary 8: 193–195.
Schneider HJ, Kreitschmann-Andermahr I, Ghigo E, Stalla GK, Agha A, 2007 Hypothalamo-pituitary dysfunction following traumatic brain injury and aneurysmal subarachnoid hemorrhage: a systematic review. JAMA 298: 1429–1438.
Aimaretti G, Ambrosio MR, Di Somma C, et al, 2005 Residual pituitary function after brain injury-induced hypopituitarism: a prospective 12-month study. J Clin Endocrinol Metab 90: 6085–6092.
Herrmann BL, Rehder J, Kahlke S, et al, 2006 Hypopituitarism following severe traumatic brain injury. Exp Clin Endocrinol Diabetes 114: 316–321.
Berg C, Oeffner A, Schumm-Draeger PM, et al, 2009 Prevalence of Anterior Pituitary Dysfunction in Patients following Traumatic Brain Injury in a German Multi-centre Screening Program. Exp Clin Endocrinol Diabetes 118: 139–144.
Klose M, Juul A, Struck J, Morgenthaler NG, Kosteljanetz M, Feldt-Rasmussen U, 2007 Acute and long-term pituitary insufficiency in traumatic brain injury: a prospective single-centre study. Clin Endocrinol (Oxf) 67: 598–606.
Tanriverdi F, Senyurek H, Unluhizarci K, Selcuklu A, Casanueva FF, Kelestimur F, 2006 High risk of hypopituitarism after traumatic brain injury: a prospective investigation of anterior pituitary function in the acute phase and at 12-months after the trauma. J Clin Endocrinol Metab 91: 2105–2111.
Schneider HJ, Schneider M, Saller B, et al, 2006 Prevalence of anterior pituitary insufficiency 3 and 12 months after traumatic brain injury. Eur J Endocrinol 154: 259–265.
Sesmilo G, Halperin I, Puig-Domingo M, 2007 Endocrine evaluation of patients after brain injury: what else is needed to define specific clinical recommendations? Hormones (Athens) 6: 132–137.
Agha A, Rogers B, Mylotte D, et al, 2004 Neuroendocrine dysfunction in the acute phase of traumatic brain injury. Clin Endocrinol (Oxf) 60: 584–591
Lee SC, Zasler ND, Kreutzer JS, 1994 Male pituitarygonadal dysfunction following severe traumatic brain injury. Brain Inj 8: 571–577.
Woolf PD, Hamill RW, McDonald JV, Lee LA, Kelly M, 1986 Transient hypogonadotrophic hypogonadism after head trauma: effects on steroid precursors and correlation with sympathetic nervous system activity. Clin Endocrinol (Oxf) 25: 265–274.
Speroff L, Glass R, Kase N 2005. In Clinical Gynecologic Endocrinology and Infertility. 7th edn. Lippincott Williams & Wilkins, Baltimore, pp, 438–439.
Falsetti L, Gambera A, Barbetti L, Specchia CM, 2002 Long term follow-up of functional hypothalamic amenorrhea and prognostic factors. J Clin Endocrinol Metab 87: 500–505.
Benvenga S, Lo Giudice F, Campenni A, Longo M, Trimarchi F, 1997 Post-traumatic selective hypogonadotropic hypogonadism. J Endocrinol Invest 20: 675–680.
Raivio T, Falardeau J, Dwyer A, et al, 2007 Reversal of idiopathic hypogonadotropic hypogonadism. N Engl J Med 357: 863–873.
Agha A, Ryan J, Sherlock M, Thompson CJ, 2005 Spontaneous recovery from posttraumatic hypopituitarism. Am J Phys Med Rehabil 84: 381–385.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ruggeri, R.M., Smedile, G., Granata, F. et al. Spontaneous recovery from isolated post-traumatic central hypogonadism in a woman. Hormones 9, 332–337 (2010). https://doi.org/10.14310/horm.2002.1285
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.14310/horm.2002.1285