
Abstract
Introduction
To detect a neuronal threshold of tolerance to ischemia, the usefulness of multilobar electrocorticography (mEcoG) during intracranial aneurysm surgery was compared to the scalp EEG and correlated with the postoperative neurological status and the radiological findings.
Methods
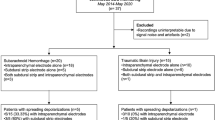
Twenty-one patients harboring intracranial aneurysms were monitored by simultaneous scalp EEG and lobe-dependent mEcoG during surgical clipping. The patients were divided into group A (6 patients with no temporary clipping) and group B (15 patients with temporary clipping).
Results
New focal modifications of the mEcoG signal with high frequency (HF)-β3 and delta waves were observed in none of the patients in group A and all of the patients in group B. These anomalies were followed by focal burst suppression pattern in eight cases (53%) in group B. These changes were detected in only two cases (9%) on the scalp EEG. New corticographic changes resolved in eight patients (53%) in group B. Among the seven patients in group B who had persistent focal burst pattern after clip removal, six (85%) presented with new neurological deficit or new hypodensity on CT. The Glasgow Outcome Scale was good (IV or V) in 85% of cases.
Conclusion
mEcoG is more sensitive than scalp EEG. The appearance and persistence of the focal burst suppression pattern shown on mEcoG, was associated with a new neurological deficit or new hypodensity, whereas HF-β3 or delta waves per se were not associated with new changes. A better comprehension of these EEG anomalies could determine the duration of temporary clipping and consequently influence the surgical strategy.
Similar content being viewed by others


References
Little JR, Lesser RP, Luders H. Electrophysiological monitoring during basilar aneurysm operation. Neurosurgery 1987;20(3): 421–426.
Ulbert I, Halgren E, Heit G, Karmos G. Multiple microelectrode-recording system for human intracortical applications. J Neurosci Methods 2001;106:69–79.
Nuwer MR, Daube J, Fischer C, Schramm J, Yingling CD. Neuromonitoring during surgery. Report of an IFCN committee. Electroencephalogr Clin Neurophysiol 1993;87:263–276.
Huotari AM, Koskinen M, Suominen K, et al. Evoked EEG patterns during burst suppression with propofol. Br J Anesth 2004;92(1):18–24.
Lopez JR, Chang SD, Steinberg GK. The use of electrophysiological monitoring in the intra-operative management of i. c. aneurysms. J Neurol Neurosurg Psych 1999;66:189–196.
Mooij JA, Buchthal A, Belopavlovic M. Somatosensory evoked potential monitoring of temporary middle cerebral artery occlusion during aneurysm operation. Neurosurgery 1987;21: 492–496.
Debatisse D, Pralong E, Dehdashti AR, Regli L. Simultaneous multilobar electrocorticography (mEcoG) and scalp electroencephalography (scalp EEG) during intracranial vascular surgery: a new approach in neuromonitoring. Clin Neurophysiol 2005;116(12):2734–2740.
Emerson RG, Turner CA. Monitoring during supratentorial surgery. J Clin Neurophys 1993;10:404–411.
Mizoi K, Yoshimoto T. Permissible temporary occlusion time in aneurysm surgery as evaluated by evoked potential monitoring. Neurosurgery 1993;33:434–440.
Quinones-Hinojosa A, Alam M, Loyn R, Yingling CD, Lawton MT. Transcranial motor evoked potentials during basilar artery aneurysm surgery: Technique application for 30 consecutive patients. Neurosurgery 2004;54:916–924.
Suzuki K, Kodama N, Sasaki T, et al. Intraoperative monitoring of blood flow insufficiency in the anterior choroidal artery during aneurysm surgery. J Neurosurg 2003;98(3):507–514.
Neuloh G, Schramm J. Monitoring of motor evoked potentials compared with somatosensory evoked potentials and microvascular Doppler US in cerebral aneurysm surgery. J Neurosurg 2004;100(3):389–399.
Jones T, Chiappa K, Young RR, Ojemann RG, Crowell RM. EEG monitoring for induced hypotension for surgery of intracranial aneurysms. Stroke 1979;10(3):292–294.
Nuwer MR, Comi G, Emerson R. IFCN standards for digital recording of clinical EEG. Electroencephalogr Clin Neurophysiol 1998;106:259–261.
Martin CJ, Sinson G, Patterson T, Zager EL, Stecker MM. Sensitivity of scalp EEG, cortical EEG and somatosensory evoked responses during surgery for intracranial aneurysms. Surg Neurol 2002;58:317–321.
Friedman WA, Chadwick GM, Verhoeven FJS, Mahla M, Day AL. Monitoring of somatosensory evoked potentials during surgery for middle cerebral artery aneurysms. Neurosurgery 1991;29: 83–88.
Friedman WA, Kaplan BL, Day AL, Sypert GW, Curran MT. Evoked potential monitoring during aneurysm operation: observations after fifty cases. Neurosurgery 1987;20:678–687.
Krieger D, Adams HP, Albert DIMF, Haken MV, Hacke W. Pure motor hemiparesis with stable somatosensory evoked potential monitoring during aneurysm surgery: case report. Neurosurgery 1992;31:145–150.
Jennet B, Bond M. Assessment of outcome after severe brain damage. Lancet 1975;i:480–484.
Fujimura N, Tanaka E, Yamamoto S, Shigemori M, Hiogashi H. Contribution of ATP-sensitive potassium channels to hypoxic hyperpolarization in rat hippocampal CA1 neurons in vitro. J Neurophysiol 1997;77:378–385.
Muller M, Somjen GG. Na(+) and K(+) concentrations, extra-and intracellular voltages, and the effect of TTX in hypoxic rat hippocampal slices. J Neurophysiol 2000;83:735–745.
O'Connor SC, Robinson PA. Analysis of the electroencephalographic activity associated with thalamic tumors. J Theor Biol 2005;233(3):271–286.
Baker CJ, Ortiz O, Solomon RA. Resolution of CT hypodense lesions in patients with subarachnoid hemorrhage. Surg Neurol 1993;39:158–162.
Schick U, Dohnert J, Meyer JJ, Vitzthum EH. Effects of temporary clips on somatosensory evoked potentials in aneurysm surgery. Neurocrit Care 2005;2(2):141–149.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dehdashti, A.R., Pralong, E., Debatisse, D. et al. Multilobar electrocorticography monitoring during intracranial aneurysm surgery. Neurocrit Care 4, 215–222 (2006). https://doi.org/10.1385/NCC:4:3:215
Issue Date:
DOI: https://doi.org/10.1385/NCC:4:3:215