
Abstract
Background: It is controversial whether a low cerebral blood flow (CBF) simply reflects the severity of injury or whether ischemia contributes to the brain’s injury. It is also not clear whether posttraumatic cerebral hypoperfusion results from intracranial hypertension or from pathologic changes of the cerebral vasculature. The answers to these questions have important implications for whether and how to treat a low CBF.
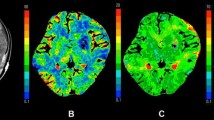
Methods: We performed a retrospective analysis of 77 patients with severe traumatic brain injury who had measurement of CBF within 12 hours of injury. CBF was measured using xenon-enhanced computed tomography (XeCT). Global CBF, physiological parameters at the time of XeCT, and outcome measures were analyzed.
Results: Average global CBF for the 77 patients was 36±16 mL/100g/minutes. Nine patients had an average global CBF <18 (average 12±5). The remaining 68 patients had a global CBF of 39±15. The initial ICP was >20 mmHg in 90% and >30 mmHg in 80% of patients in the group with CBF<18, compared to 33% and 16%, respectively, in the patients with CBF≥18. Mortality was 90% at 6 months postinjury in patients with CBF<18. Mortality in the patients with CBF>18 was 19% at 6 months after injury.
Conclusion: In patients with CBF<18 mL/100 g/minutes, intracranial hypertension plays a major causative role in the reduction in CBF. Treatment would most likely be directed at controlling intracranial pressure, but the early, severe intracranial hypertension also probably indicates a severe brain injury. For levels of CBF between 18 and 40 mL/100 g/minutes, the presence of regional hypoperfusion was a more important factor in reducing the average CBF.
Article PDF
Similar content being viewed by others

References
Overgaard J, Molsdal C, Tweed TA. Cerebral circulation after head injury. Part 3: does reduced regional cerebral blood flow determine recovery of brain function after blunt head injury? J Neurosurg 1981;55:63–74.
Overgaard J, Tweed WA. Cerebral circulation after head injury. Part 4: functional anatomy and boundary-zone flow deprivation in the first week of traumatic coma. J Neurosurg 1983;59:439–446.
Robertson CS, Contant CF, Gokaslan ZL, et al. Cerebral blood flow, arteriovenous oxygen difference, and outcome in head injured patients. J Neurol Neurosurg Psych 1992;55:594–603.
Bouma GJ, Muizelaar JP, Stringer WA, et al. Ultraearly evaluation of regional cerebral blood flow in severely head-injured patients using xenon-enhanced computerized tomography. J Neurosurg 1992;77:360–368.
Muizelaar JP, Marmarou A, DeSalles AA, et al. Cerebral blood flow and metabolism in severely head-injured children. Part 1: relationship with GCS score, outcome, ICP, and PVI. J Neurosurg 1989;71:63–71.
Obrist WD, Gennarelli TA, Segawa H, et al. Relation of cerebral blood flow to neurological status on outcome in head-injured patients. J Neurosurg 1979;51:292–300.
Kelly DF, Kordestani RK, Martin NA, et al. Cerebral blood flow as a predictor of outcome following traumatic brain injury. J Neurosurg 1997;86:633–641.
Cherian L, Goodman JC, Robertson CS. Brain nitric oxide changes after controlled cortical impact injury in rats. J Neurophysiol 2000;83:2171–2178.
Cherian L, Chacko G, Goodman JC, et al. Cerebral hemodynamic effects of phenylephrine and L-arginine after cortical impact injury. Crit Care Med 1999;27:2512–2517.
Bullock RM, Chesnut R, Clifton GL, et al. Management and prognosis of severe traumatic brain injury. Part 1: guidelines for the management of severe traumatic brain injury. J Neurotrauma 2000;17:449–597.
Yonas H, Darby JM, Marks EC, et al. CBF measured by Xe-CT: approach to analysis and normal values. J Cereb Blood Flow Metab 1991;11:716–725.
Leenders KL, Perani D, Lammetsma AA, et al. Cerebral blood flow, blood volume, and oxygen utilization. Normal values and effect of age. Brain 1990;113:27–47.
Robertson CS, Narayan RK, Gokaslan Z, et al. Cerebral arteriovenous oxygen difference as an estimate of cerebral blood flow in comatose patients. J Neurosurg 1989;70:222–230.
Astrup J, Siesjo BK, Symon L. Thresholds in cerebral ischemia—the ischemic penumbra. Stroke 1981;12:723–725.
Cold GE. Cerebral blood flow in acute head injury. The regulation of cerebral blood flow and metabolism during the acute phase of head injury, and its significance for therapy. Acta Neurochir Suppl (Wien) 1990;49:1–64.
Obrist WD, Langfitt T, Jaggi J, et al. Cerebral blood flow and metabolism in comatose patients with acute head injury. Relationship to intracranial hypertension. J Neurosurg 1984;61:241–253.
Marion DW, Darby J, Yonas H. Acute regional cerebral blood flow changes caused by severe head injuries. J Neurosurg 1991;74:407–414.
Bouma GJ, Muizelaar JP, Choi SC, et al. Cerebral blood flow and metabolism after severe traumatic brain injury: the elusive role of ischemia. J Neurosurg 1991;75:685–693.
Feldman Z, Robertson CS. Monitoring of cerebral hemodynamics with jugular bulb catheters. In: Diringer M, ed. Critical Care Clinics. Vol. 13, number 1. Philadelphia: W.B. Saunders Company, 1997, pp. 51–77.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hlatky, R., Contant, C.F., Diaz-Marchan, P. et al. Significance of a reduced cerebral blood flow during the first 12 hours after traumatic brain injury. Neurocrit Care 1, 69–83 (2004). https://doi.org/10.1385/NCC:1:1:69
Issue Date:
DOI: https://doi.org/10.1385/NCC:1:1:69