
Abstract
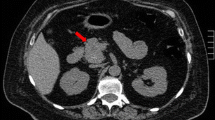
We report a very rare case of Cushing’s syndrome caused by an ileal adrenocorticotrophin-secreting well-differentiated endocrine carcinoma with liver metastases. A 62-yr-old woman presented with clinical and biological signs suggestive of paraneoplastic Cushing’s syndrome. Radiological investigations, including magnetic resonance imaging of the pituitary gland, chest and abdominal computerized tomography scan, small bowel barium study and pancreatic endoscopic scan, 111-pentetreotide scintigraphy (octreoscan), esogastroduodenoscopy, and colonoscopy did not detect the source of the ectopic adrenocorticotropic hormone (ACTH) secretion but showed a few liver nodules. Because a 10-mo-long ketoconazole treatment was not effective, a bilateral adrenalectomy was performed in order to control the Cushing’s syndrome, and a liver nodule biopsy diagnosed a metastatic neuroendocrine tumor. Subsequently, a second laparotomy disclosed a 1.8 cm ileal neuroendocrine tumor, cosecreting ACTH and serotonin on immunohistochemistry with many liver metastases.
ACTH secretion by intestinal neuroendocrine tumors is rare, and the secretion is almost always clinically silent. Cushing’s syndrome caused by an intestinal low-grade neuroendocrine tumor is even rarer, with only two previous cases reported in the literature. Our observation underlines the difficulty of localizing the source of ectopic ACTH secretion in paraneoplastic Cushing’s syndrome.
Similar content being viewed by others


References
Kulke HM, Mayer RJ. Carcinoid Tumors. N Engl J Med 340:858–868, 1999.
Modlin IM, Sandor A. An analysis of 8305 cases of carcinoid tumors. Cancer 79:813–829, 1997.
Kirshbom PM, Kherani AR, Onaitis MW, Feldman JM, Tyler DS. Carcinoids of unknown origin: comparative analysis with foregut, midgut, and hindgut carcinoids. Surgery 124:1063–1070, 1998.
Gabrilove JL, Nicolis GL, Kirschner PA. Cushing’s syndrome in association with carcinoid tumor. Ann Surg 169:240–248, 1969.
Ross RJM, Trainer PJ. Endocrine investigation: Cushing’s syndrome. Clin Endocrinol 49:153–155, 1998.
Trainer PJ, Grossman A. The diagnosis and differential diagnosis of Cushing’s syndrome. Clin Endocrinol 34:317–330, 1991.
Segu VB, Mahvi DM, Wilson MA, et al. Use of In-111 pentreotide scintigraphy in the diagnosis of a midgut carcinoid causing Cushing’s syndrome. Eur J Endocrinol 137:79–83, 1997.
Solcia E, Klöppel G, Sobin LH. Histological typing of Endocrine tumors. International histological classification of tumors, 2nd ed., World Health Organisation, Berlin, Heidelberg, New York, Springer-Verlag 2000.
Tabarin A, Valli N, Chanson P, et al. Usefulness of somatostatin scintigraphy in patients with occult ectopic adrenocorticotropin syndrome. J Clin Endocrinol Metab 84:1193–1202, 1999.
Solcia E, Fiocca R, Rindi G, et al. Endocrine tumors of the small and large intestine. Path Res Pract 191:366–372, 1995.
Kent Jex R, Van Heerden JA, Carpenter PC, Grant CS. Ectopic ACTH syndrome. Am J Surg 149:276–282, 1985.
Miller T, Berstein J, Van Herle. A Cushing’s syndrome cured by resection of appendiceal carcinoid. Arch Surg 103:770–773, 1971.
Dombrovskaia EA, Romenskaia O. Carcinoid tumor of the small intestine associated with Cushing’s syndrome. Problemy endokrinologii 23:63–64, 1977.
Capella C, Heitz PU, Höfler H, Solcia E, Klöppel G. Revised classification of neuroendocrine tumors of the lung, pancreas and gut. Digestion 55(suppl 3):11–23, 1994.
Leveston SA, Mc Keel DW, Buckley PJ, et al. Acromegaly and Cushing’s syndrome associated with a foregut carcinoïd tumor. J Clin Endocrinol Metab 53:682–689, 1981.
Makridis C, Ekbom A, Bring J, et al. Survival and daily physical activity in patients treated for advanced midgut carcinoid tumors. Surgery 122:1075–1082, 1997.
Votte A, Cattan D, Dupas JL. Traitement des tumeurs carcinoïdes du tube digestif. Gastroenterol Clin Biol 19:1031–1042, 1995.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Valo, I., Rohmer, V., Guyétant, S. et al. Cushing’s syndrome caused by a well-differentiated Ileal neuroendocrine carcinoma. Endocr Pathol 11, 359–364 (2000). https://doi.org/10.1385/EP:11:4:359
Issue Date:
DOI: https://doi.org/10.1385/EP:11:4:359