
Abstract
Background
This study aimed to assess the long-term outcomes of video-assisted mediastinoscopic lymphadenectomy (VAMLA) combined with video-assisted thoracic surgery (VATS) for left-sided lung cancer pulmonary resection.
Patients and Methods
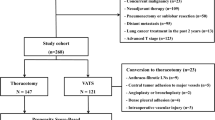
We retrospectively reviewed 1194 consecutive patients who underwent VATS anatomical resection for left-sided lung cancer between January 2007 and December 2016. Using propensity score-based inverse probability of treatment weighting (IPTW), perioperative outcomes and long-term survival outcomes were compared.
Results
Among 1194 patients, 295 (24.7%) underwent additional VAMLA (VATS + VAMLA group) and 899 patients (75.3%) underwent VATS only (VATS group). The proportion of patients with advanced N stage were higher in the VATS + VAMLA group (24.7%) than in the VATS group (18.3%). After IPTW adjustment, all baseline profiles between the two groups became similar. The long-term overall survival (OS) and recurrence-free survival (RFS) rates were similar between the VATS + VAMLA group and the VATS group (5-year OS, 77.8% versus 79.3%, p = 0.957; 5-year RFS, 69.6% versus 70.1%, p = 0.498). However, among patients with borderline pulmonary function (FEV1 ≤ 60% or DLCO ≤ 60%), the VATS + VAMLA group (n = 23) had a better prognosis than the VATS group (n = 36) (5-year OS, 67.4% versus 46.7%, respectively; p = 0.047; 5-year RFS, 74.6% versus 53.5%, respectively; p = 0.027).
Conclusions
VAMLA might be a good complement to VATS for left-sided lung cancer, wherein optimal mediastinal lymph node dissection is not feasible under one-lung ventilation, such as when patients have borderline pulmonary function.




Similar content being viewed by others


References
Rusch VW, Crowley J, Giroux DJ, et al. The IASLC Lung Cancer Staging Project: proposals for the revision of the N descriptors in the forthcoming seventh edition of the TNM classification for lung cancer. J Thorac Oncol. 2007;2(7):603–612
Mokhles S, Macbeth F, Treasure T, et al. Systematic lymphadenectomy versus sampling of ipsilateral mediastinal lymph-nodes during lobectomy for non-small-cell lung cancer: a systematic review of randomized trials and a meta-analysis. Eur J Cardiothorac Surg. 2017;51(6):1149–56.
Doddoli C, Aragon A, Barlesi F, et al. Does the extent of lymph node dissection influence outcome in patients with stage I non-small-cell lung cancer? Eur J Cardiothorac Surg. 2005;27(4):680–5.
Hurtgen M, Friedel G, Toomes H, Fritz P. Radical video-assisted mediastinoscopic lymphadenectomy (VAMLA)–technique and first results. Eur J Cardiothorac Surg. 2002;21(2):348–51.
Leschber G, Holinka G, Linder A. Video-assisted mediastinoscopic lymphadenectomy (VAMLA)–a method for systematic mediastinal lymphnode dissection. Eur J Cardiothorac Surg. 2003;24(2):192–5.
Turna A, Demirkaya A, Ozkul S, Oz B, Gurses A, Kaynak K. Video-assisted mediastinoscopic lymphadenectomy is associated with better survival than mediastinoscopy in patients with resected non-small cell lung cancer. J Thorac Cardiovasc Surg. 2013;146(4):774–80.
Palade E, Passlick B, Osei-Agyemang T, Gunter J, Wiesemann S. Video-assisted vs open mediastinal lymphadenectomy for Stage I non-small-cell lung cancer: results of a prospective randomized trial. Eur J Cardiothorac Surg. 2013;44(2):244–9 (discussion 249).
Witte B, Messerschmidt A, Hillebrand H, et al. Combined videothoracoscopic and videomediastinoscopic approach improves radicality of minimally invasive mediastinal lymphadenectomy for early stage lung carcinoma. Eur J Cardiothorac Surg. 2009;35(2):343–7.
Yoo DG, Kim YH, Kim DK, Kim HR, Park SI. Clinical feasibility and surgical benefits of video-assisted mediastinoscopic lymphadenectomy in the treatment of resectable lung cancer. Eur J Cardiothorac Surg. 2011;40(6):1483–6.
Kim HJ, Kim YH, Choi SH, Kim HR, Kim DK, Park SI. Video-assisted mediastinoscopic lymphadenectomy combined with minimally invasive pulmonary resection for left-sided lung cancer: feasibility and clinical impacts on surgical outcomesdagger. Eur J Cardiothorac Surg. 2016;49(1):308–13.
Yun JK, Bok JS, Lee GD, et al. Long-term outcomes of upfront surgery in patients with resectable pathological N2 non-small-cell lung cancer. Eur J Cardiothorac Surg. 2020;58(1):59–69.
Detterbeck FC, Boffa DJ, Kim AW, Tanoue LT. The eighth edition lung cancer stage classification. Chest. 2017;151(1):193–203
Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat Med. 2015;34(28):3661–79.
Xie J, Liu C. Adjusted Kaplan-Meier estimator and log-rank test with inverse probability of treatment weighting for survival data. Stat Med. 2005;24(20):3089–110.
Silvestri GA, Gonzalez AV, Jantz MA, et al. Methods for staging non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5 Suppl):e211S-e250S.
Lin J, Fernandez F. Indications for invasive mediastinal staging for non-small cell lung cancer. J Thorac Cardiovasc Surg. 2018;156(6):2319–24.
Misthos P, Katsaragakis S, Theodorou D, Milingos N, Skottis I. The degree of oxidative stress is associated with major adverse effects after lung resection: a prospective study. Eur J Cardiothorac Surg. 2006;29(4):591–5.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
None of the authors have a financial relationship with a commercial entity that has an interest in the subject of the presented manuscript or any other conflicts of interest to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Yun, J.K., Yoo, S., Lee, G.D. et al. Comparison of Long-Term Outcomes Between Minimally Invasive Pulmonary Resection With and Without Video-Assisted Mediastinoscopic Lymphadenectomy for Left-Sided Lung Cancer. Ann Surg Oncol 29, 2830–2839 (2022). https://doi.org/10.1245/s10434-021-11191-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-021-11191-8