
Abstract
Introduction
The effect of neoadjuvant systemic therapies (NST) on technical aspects of operation for resectable stage III melanoma is unknown. Prospective capture of the estimated and actual degree of difficulty of therapeutic lymphadenectomy at presentation and after NST may inform the relative merits of NST versus surgery followed by adjuvant therapy.
Methods
We designed surgeon survey tools to capture key impressions at baseline prior to NST and postoperatively. We conducted a sub-study within a multi-institutional clinical trial for high-risk operable stage III melanoma (NeoACTIVATE, NCT03554083) which enrolls clinically node-positive patients to 12 weeks of combinatorial NST determined by BRAF status. Survey data were analyzed.
Results
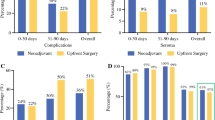
Surveys were completed for 24 of 25 patients (96%). Affected nodal basins were cervical (3, 13%) axillary (9, 38%), inguinal ± pelvic (14, 58%); 2 (8%) involved ≥ 2 basins. Baseline estimates included largest affected node size (median/range 4/1.4–11 cm), number of involved nodes (median/range 3/1–10) and tumor fixation (present in 12, 50%). At operation, actual degree of difficulty increased from the baseline estimate in 4 (17%) and decreased in 6 (25%). Surgery was less difficult, average, or more difficult versus usual operation in 4, 9, and 11 cases (17%, 38%, 46%), respectively.
Conclusions
Although many operations were judged to be more difficult than the usual therapeutic lymphadenectomy, operation following NST was more often perceived as easier than more difficult versus baseline impression. Engaging surgical oncologists to perform similar structured assessments across clinical trials will permit cross-study analysis of the effect of NSTs on the technical conduct of lymphadenectomy.



Similar content being viewed by others


References
NCCN Clinical Practice Guidelines in Oncology, Melanoma: Cutaneous, v2.2021, available at https://www.nccn.org/professionals/physician_gls/pdf/cutaneous_melanoma.pdf, Accessed 1 June 2021.
Seth R, Messersmith H, Kaur V, Kirkwood JM, Kudchadkar R, McQuade JL, et al. Systemic therapy for melanoma: ASCO guideline. J Clin Oncol. 2020;38(33):3947–70.
Dummer R, Hauschild A, Santinami M, et al. Five-year analysis of adjuvant Dabrafenib plus Trametinib in stage III melanoma. N Engl J Med. 2020;383:1139–48.
Ascierto PA, Del Vecchio M, Mandala M, et al. Adjuvant nivolumab versus ipilimumab in resected stage III or IV melanoma. Lancet Oncol. 2020;21:1465–77.
Eggermont AMM, Blank CU, Mandala M, et al. Longer follow-up confirms recurrence-free survival benefit of adjuvant pembrolizumab in high-risk stage III melanoma: updated results from the EORTC 1325-MG/KEYNOTE-054 trial. J Clin Oncol. 2020;38:3925–36.
Weber J, Mandala M, Del Vecchio M, et al. Adjuvant nivolumab versus ipilimumab in resected stage III or IV melanoma. N Engl J Med. 2017;377:1824–35.
Bloemendal M, van Willigen W, Bol KF, et al. Early recurrence in completely resected IIIB and IIIC melanoma warrants restaging prior to adjuvant therapy. Ann Surg Oncol. 2019;26:3945–52.
Liu J, Blake SJ, Yong MCR, et al. Improved efficacy of neoadjuvant compared to adjuvant immunotherapy to eradicate metastatic disease. Cancer Dis. 2016;6(12):1382–99.
Menzies AM, Amaria RN, Rozeman EA, et al. Pathological response and survival with neoadjuvant therapy in melanoma: a pooled analysis from the International Neoadjuvant Melanoma Consortium (INMC). Nat Med. 2021;27:301–9.
Rozeman EA, Hoefsmit EP, Reijers LM, et al. Survival and biomarker analyses from the OpACIN-neo and OpACIN neoadjuvant immunotherapy trials in stage III melanoma. Nat Med. 2021;27:256–63.
Garcia-Aguilar J, Smith D, Avila K, Bergsland E, Chu P, Krieg R. Optimal timing of surgery after chemoradiation for advanced rectal cancer. Annals Surg. 2011;254(1):97–102.
Hieken TJ, Suman VJ, Holtan SG, Flotte TJ, Kottschade LA, Block MS. Neoadjuvant combination targeted and immunotherapy for high-risk resectable stage III melanoma (NeoACTIVATE), NCT03554083 [abstract]. In: Proceedings of the American Association for Cancer Research Annual Meeting 2019; Cancer Res. 2019;79(13 Suppl):Abstract nr CT121.
Neoadjuvant Combination Targeted and Immunotherapy for Patients With High-Risk Stage III Melanoma (NeoACTIVATE) Identifier: NCT03554083 Available at: https://clinicaltrials.gov/ct2/show/NCT03554083. Accessed 1 July 2021.
Long GV, Saw RPM, Lo S, et al. Neoadjuvant dabrafenib combined with trametinib for resectable, stage IIIB-C, BRAF V600 mutation-positive melanoma (NeoCombi): a single-arm, open-label, single-centre, phase 2 trial. Lancet Oncol. 2019;20:961–71.
Amaria R, Menzies AM, Burton EM, et al. Neoadjuvant systemic therapy in melanoma: recommendations of the International Neoadjuvant Melanoma Consortium. Lancet Oncol. 2019;20(7):e378–89.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
This work was funded by a Stand Up to Cancer Catalyst® Award supported by Genentech.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hieken, T.J., Price, D.L., Piltin, M.A. et al. Surgeon Assessment of the Technical Impact of Neoadjuvant Systemic Therapy on Operable Stage III Melanoma. Ann Surg Oncol 29, 780–786 (2022). https://doi.org/10.1245/s10434-021-11112-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-021-11112-9