
Abstract
Background
Multiple adjuvant therapies for melanoma have been approved since 2015 based on randomized trials demonstrating improvements in recurrence-free survival (RFS) with adjuvant therapy after surgical resection of high-risk disease. Inclusion criteria for these trials required performance of a completion lymph node dissection (CLND) for positive sentinel lymph node (pSLN) disease.
Objective
We aimed to describe current practice for adjuvant therapies in patients with pSLN without CLND (active surveillance [AS]), and to evaluate recurrence in these patients.
Methods
Melanoma patients with pSLN between 2016 and 2019 were identified at two institutions. Demographic information, disease and treatment characteristics, and recurrence details were reviewed retrospectively. Patients were stratified by recurrence and patient-, treatment- and tumor-related characteristics were compared using Fisher’s exact test and t test for categorical and continuous variables, respectively.
Results
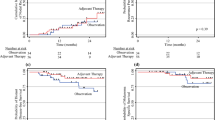
Overall, 245 SLN biopsies were performed, of which 36 (14.7%) were pSLN. Of 36 pSLN, 4 underwent CLND and 32 underwent AS, of whom 22 (68.8%) received adjuvant therapy with the anti-programmed death-1 (PD1) inhibitor nivolumab (16/22), anti-cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) inhibitor ipilimumab (3/22), or BRAF/MEK inhibitors (3/22). At a median follow up of 13.3 months, 7/32 (21.9%) patients on AS recurred, including 4/22 (18.2%) who received adjuvant therapy and 3/10 (30.0%) who did not. Tumor ulceration was significantly associated with recurrence. While not significant, acral lentiginous subtype appeared more common among those with recurrence.
Conclusion
The majority (68.8%) of patients with pSLN managed without CLND were treated with adjuvant therapy. The 1-year RFS for patients managed with adjuvant therapy without CLND was 82%, which is similar to modern adjuvant therapy trials requiring CLND.

Similar content being viewed by others


References
Faries MB, Thompson JF, Cochran AJ, et al. Completion dissection or observation for sentinel-node metastasis in melanoma. N Engl J Med. 2017;376(23):2211–22.
Leiter U, Stadler R, Mauch C, et al. Complete lymph node dissection versus no dissection in patients with sentinel lymph node biopsy positive melanoma (DeCOG-SLT): a multicentre, randomised, phase 3 trial. Lancet Oncol. 2016;17(6):757–67.
Weber J, Mandalà M, Del Vecchio M, et al. Adjuvant therapy with nivolumab (NIVO) versus ipilimumab (IPI) after complete resection of stage III/IV melanoma: updated results from a phase III trial (CheckMate 238) [abstract no. 9502]. J Clin Oncol. 2018;36(Suppl):9502.
Eggermont AMM, Chiarion-Sileni V, Grob JJ, et al. Adjuvant ipilimumab versus placebo after complete resection of stage III melanoma: long-term follow-up results of the European Organisation for Research and Treatment of Cancer 18071 double-blind phase 3 randomised trial. Eur J Cancer. 2019;119:1–10.
Long GV, Hauschild A, Santinami M, et al. Adjuvant dabrafenib plus trametinib in stage III BRAF-mutated melanoma. N Engl J Med. 2017;377:1813–23.
Eggermont AMM, Blank CU, Mandala M, et al. Adjuvant pembrolizumab versus placebo in resected stage III melanoma. N Engl J Med. 2018;378(19):1789–801.
van der Ploeg AP, van Akkooi AC, Schmitz PI, Koljenovic S, Verhoef C, Eggermont AM. EORTC Melanoma Group sentinel node protocol identifies high rate of submicrometastases according to Rotterdam Criteria. Eur J Cancer. 2010;46(13):2414–21.
Acknowledgments
Drs. Farrow and Raman are supported by a National Institutes of Health T-32 Grant (T32-CA093245) for translational research in surgical oncology.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Georgia M. Beasley was a one-time consultant for Regeneron in 2019.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Farrow, N.E., Raman, V., Williams, T.P. et al. Adjuvant Therapy is Effective for Melanoma Patients with a Positive Sentinel Lymph Node Biopsy Who Forego Completion Lymphadenectomy. Ann Surg Oncol 27, 5121–5125 (2020). https://doi.org/10.1245/s10434-020-08478-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-020-08478-7