
Abstract
Background
Post hepatectomy liver failure (PHLF) is associated with significant perioperative morbidity and mortality. A tool to identify patients at risk for PHLF may allow for earlier intervention to mitigate its severity and help clinicians when counseling patients. Our objective was to develop a PHLF risk calculator.
Study Design
Patients who underwent hepatectomy for any indication from 2014 to 2017 were identified from ACS NSQIP. A multivariable logistic regression model was developed that included preoperative and intraoperative variables. Model fit was assessed for discrimination using the C-statistic, and calibration using Hosmer and Lemeshow (HL) Chi square. Validation of the calculator was performed utilizing tenfold cross validation.
Results
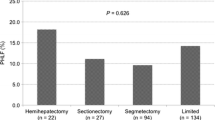
Among 15,636 hepatectomy patients analyzed, the overall incidence of clinically significant PHLF was 2.8%. Preoperative patient factors associated with increased PHLF were male gender, preoperative ascites within 30 days of surgery, higher ASA class, preoperative total bilirubin greater than 1.2 mg/dl, and AST greater than 40 units/l. Disease related factors associated with PHLF included histology, and use of neoadjuvant therapy. Intraoperative factors associated with PHLF were extent of resection, open surgical approach, abnormal liver texture, and biliary reconstruction. The calculator’s C-statistic was 0.83 and the HL Chi square was 10.9 (p = 0.21) demonstrating excellent discrimination and calibration. On tenfold cross validation, the mean test group C-statistic was 0.82 and the HL p value was 0.26.
Conclusion
We present a multi-institutional preoperative and early postoperative PHLF risk calculator, which demonstrated excellent discrimination and calibration. This tool can be used to help identify high-risk patients to facilitate earlier interventions.


Similar content being viewed by others


References
Khatri VP, Petrelli NJ, Belghiti J. Extending the frontiers of surgical therapy for hepatic colorectal metastases: Is there a limit? J Clin Oncol. 2005;23(33):8490–99.
Rahbari NN, Garden OJ, Padbury R, et al. Posthepatectomy liver failure: a definition and grading by the International Study Group of Liver Surgery (ISGLS). Surgery. 2011;149(5):713–24.
Reissfelder C, Rahbari NN, Koch M, et al. Postoperative course and clinical significance of biochemical blood tests following hepatic resection. Br J Surg. 2011;98(6):836–44.
Balzan S, Belghiti J, Farges O, et al. The “50-50 criteria” on postoperative day 5: an accurate predictor of liver failure and death after hepatectomy. Ann Surg. 2005;242(6):824–28 (discussion 828–829).
Rahbari NN, Reissfelder C, Koch M, et al. The predictive value of postoperative clinical risk scores for outcome after hepatic resection: a validation analysis in 807 patients. Ann Surg Oncol. 2011;18(13):3640–49.
Cohen ME, Ko CY, Bilimoria KY, et al. Optimizing ACS NSQIP modeling for evaluation of surgical quality and risk: patient risk adjustment, procedure mix adjustment, shrinkage adjustment, and surgical focus. J Am Coll Surg. 2013;217(2):336–346.e331.
7. Jung Y, Hu J. A K-fold averaging cross-validation procedure. J Nonparametric Stat. 2015;27(2):167–79.
Smith GC, Seaman SR, Wood AM, Royston P, White IR. Correcting for optimistic prediction in small data sets. Am J Epidemiol. 2014;180(3):318–324.
Bilimoria KY, Liu Y, Paruch JL, et al. Development and evaluation of the universal ACS NSQIP surgical risk calculator: a decision aid and informed consent tool for patients and surgeons. J Am Coll Surg. 2013;217(5):833–842.e831-833.
Mullen JT, Ribero D, Reddy SK, et al. Hepatic insufficiency and mortality in 1,059 noncirrhotic patients undergoing major hepatectomy. J Am Coll Surg. 2007;204(5):854–62 (discussion 862–854).
Malinchoc M, Kamath PS, Gordon FD, Peine CJ, Rank J, ter Borg PC. A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts. Hepatology (Baltimore, Md). 2000;31(4):864–71.
Bellavance EC, Lumpkins KM, Mentha G, et al. Surgical management of early-stage hepatocellular carcinoma: resection or transplantation? J Gastroint Surg. 2008;12(10):1699–08.
Teh SH, Nagorney DM, Stevens SR, et al. Risk factors for mortality after surgery in patients with cirrhosis. Gastroenterology. 2007;132(4):1261–69.
Hyder O, Pulitano C, Firoozmand A, et al. A risk model to predict 90-day mortality among patients undergoing hepatic resection. J Am Coll Surg. 2013;216(6):1049–56.
Ray S, Mehta NN, Golhar A, Nundy S. Post hepatectomy liver failure: a comprehensive review of current concepts and controversies. Ann Med Surg (2012). 2018;34:4–10.
Ghaferi AA, Birkmeyer JD, Dimick JB. Complications, failure to rescue, and mortality with major inpatient surgery in medicare patients. Ann Surg. 2009;250(6):1029–34.
17. Rahnemai-Azar AA, Cloyd JM, Weber SM, et al. Update on liver failure following hepatic resection: strategies for prediction and avoidance of post-operative liver insufficiency. J Clin Transl Hepatol. 2018;6(1):97–104.
Merkow RP, Ko CY. Evidence-based medicine in surgery: the importance of both experimental and observational study designs. JAMA. 2011;306(4):436–37.
Funding
This work did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. JY Liu receives salary support through a contract with Agency for Healthcare Research and Quality (HHSP233201500020I).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Liu, J.Y., Ellis, R.J., Hu, Q.L. et al. Post Hepatectomy Liver Failure Risk Calculator for Preoperative and Early Postoperative Period Following Major Hepatectomy. Ann Surg Oncol 27, 2868–2876 (2020). https://doi.org/10.1245/s10434-020-08239-6
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-020-08239-6