
Abstract
Background
Lobular carcinoma in situ (LCIS) is a risk factor for breast cancer, but the effect of LCIS found in association with ductal carcinoma in situ (DCIS) is unknown. In this study, we compared contralateral breast cancer (CBC) and ipsilateral breast tumor recurrence (IBTR) rates among women with DCIS with or without synchronous ipsilateral LCIS treated with breast-conserving surgery (BCS).
Methods
DCIS patients undergoing BCS from 2000 to 2011 with a contralateral breast at risk were stratified by the presence or absence of synchronous ipsilateral LCIS with the index DCIS (DCIS + LCIS vs. DCIS). Those with contralateral, bilateral, or prior ipsilateral LCIS were excluded. Associations of patient, tumor, and treatment factors with CBC and IBTR were evaluated.
Results
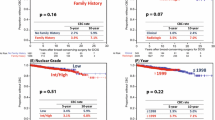
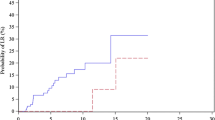
Of 1888 patients identified, 1475 (78%) had DCIS and 413 (22%) had DCIS + LCIS. At median follow-up of 7.2 (range 0–17) years, 307 patients had a subsequent first breast event; 207 IBTR and 100 CBC. The 10-year cumulative incidence of IBTR was similar in both groups: 15.0% vs. 14.2% (log-rank, p = 0.8) for DCIS + LCIS vs. DCIS, respectively. The 10-year cumulative incidence of CBC was greater in the DCIS + LCIS group: 10.9% vs. 6.1% for DCIS (log-rank, p < 0.001). After adjustment for other factors, CBC risk remained higher in DCIS + LCIS compared with DCIS (hazard ratio 2.06, 95% confidence interval 1.36–3.11, p = 0.001); there was no significant difference in IBTR risk.
Conclusions
Compared with DCIS alone, DCIS + LCIS is associated with similar IBTR risk but double the risk of CBC. This finding should inform treatment decisions, in particular regarding endocrine therapy for risk reduction.


Similar content being viewed by others

References
Haagensen CD, Lane N, Lattes R, Bodian C. Lobular neoplasia (so-called lobular carcinoma in situ) of the breast. Cancer. 1978;42(2):737–69.
King TA, Pilewskie M, Muhsen S, et al. Lobular carcinoma in situ: a 29-year longitudinal experience evaluating clinicopathologic features and breast cancer risk. J Clin Oncol. 2015;33(33):3945–52.
Page DL, Dupont WD, Rogers LW, Rados MS. Atypical hyperplastic lesions of the female breast. A long-term follow-up study. Cancer. 1985;55(11):2698–708.
Page DL, Kidd TE, Jr., Dupont WD, Simpson JF, Rogers LW. Lobular neoplasia of the breast: higher risk for subsequent invasive cancer predicted by more extensive disease. Hum Pathol. 1991;22(12):1232–9.
Rosen PP, Kosloff C, Lieberman PH, Adair F, Braun DW, Jr. Lobular carcinoma in situ of the breast. Detailed analysis of 99 patients with average follow-up of 24 years. Am J Surg Pathol. 1978;2(3):225–51.
Wong SM, King T, Boileau JF, Barry WT, Golshan M. Population-based analysis of breast cancer incidence and survival outcomes in women diagnosed with lobular carcinoma in situ. Ann Surg Oncol. 2017;24(9):2509–17.
Chuba PJ, Hamre MR, Yap J, et al. Bilateral risk for subsequent breast cancer after lobular carcinoma-in situ: analysis of surveillance, epidemiology, and end results data. J Clin Oncol. 2005;23(24):5534–41.
Adepoju LJ, Symmans WF, Babiera GV, et al. Impact of concurrent proliferative high-risk lesions on the risk of ipsilateral breast carcinoma recurrence and contralateral breast carcinoma development in patients with ductal carcinoma in situ treated with breast-conserving therapy. Cancer. 2006;106(1):42–50.
Ciocca RM, Li T, Freedman GM, Morrow M. Presence of lobular carcinoma in situ does not increase local recurrence in patients treated with breast-conserving therapy. Ann Surg Oncol. 2008;15(8):2263–71.
Griem KL, Hartsell WF, Recine DC, et al. What is the significance of a lobular carcinoma in situ (LCIS) component in women treated with breast conserving therapy (SCT) for early stage breast cancer? Int J Radiat Oncol Biol Phys. 1993;27 (supplement):269–70.
Jolly S, Kestin LL, Goldstein NS, Vicini FA. The impact of lobular carcinoma in situ in association with invasive breast cancer on the rate of local recurrence in patients with early-stage breast cancer treated with breast-conserving therapy. Int J Radiat Oncol Biol Phys. 2006;66(2):365–71.
Moran M, Haffty BG. Lobular carcinoma in situ as a component of breast cancer: the long-term outcome in patients treated with breast-conservation therapy. Int J Radiat Oncol Biol Phys. 1998;40(2):353–8.
Ottesen GL, Graversen HP, Blichert-Toft M, Christensen IJ, Andersen JA. Carcinoma in situ of the female breast. 10 year follow-up results of a prospective nationwide study. Breast Cancer Res Treat. 2000;62(3):197–210.
Sasson AR, Fowble B, Hanlon AL, et al. Lobular carcinoma in situ increases the risk of local recurrence in selected patients with stages I and II breast carcinoma treated with conservative surgery and radiation. Cancer. 2001;91(10):1862–9.
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365(9472):1687–717.
Gao X, Fisher SG, Emami B. Risk of second primary cancer in the contralateral breast in women treated for early-stage breast cancer: a population-based study. Int J Radiat Oncol Biol Phys. 2003;56(4):1038–45.
Nichols HB, Berrington de Gonzalez A, Lacey JV, Jr., Rosenberg PS, Anderson WF. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J Clin Oncol. 2011;29(12):1564–9.
Reiner AS, John EM, Brooks JD, et al. Risk of asynchronous contralateral breast cancer in noncarriers of BRCA1 and BRCA2 mutations with a family history of breast cancer: a report from the Women’s Environmental Cancer and Radiation Epidemiology Study. J Clin Oncol. 2013;31(4):433–9.
Reiner AS, Sisti J, John EM, et al. Breast cancer family history and contralateral breast cancer risk in young women: an update from the women’s environmental cancer and radiation epidemiology study. J Clin Oncol. 2018;36(15):1513–20.
Miller ME, Muhsen S, Olcese C, Patil S, Morrow M, Van Zee KJ. Contralateral breast cancer risk in women with ductal carcinoma in situ: is it high enough to justify bilateral mastectomy? Ann Surg Oncol. 2017;24(10):2889–97.
Muhsen S, Barrio AV, Miller M, et al. Outcomes for women with minimal-volume ductal carcinoma in situ completely excised at core biopsy. Ann Surg Oncol. 2017;24(13):3888–95.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66(1):7–30.
Rudloff U, Brogi E, Brockway JP, et al. Concurrent lobular neoplasia increases the risk of ipsilateral breast cancer recurrence in patients with ductal carcinoma in situ treated with breast-conserving therapy. Cancer. 2009;115(6):1203–14.
Bijker N, Meijnen P, Peterse JL, et al. Breast-conserving treatment with or without radiotherapy in ductal carcinoma-in situ: ten-year results of European Organisation for Research and Treatment of Cancer randomized phase III trial 10853–a study by the EORTC Breast Cancer Cooperative Group and EORTC Radiotherapy Group. J Clin Oncol. 2006;24(21):3381–7.
Collins LC, Achacoso N, Haque R, et al. Risk factors for non-invasive and invasive local recurrence in patients with ductal carcinoma in situ. Breast Cancer Res Treat. 2013;139(2):453–60.
Cronin PA, Olcese C, Patil S, Morrow M, Van Zee KJ. Impact of age on risk of recurrence of ductal carcinoma in situ: outcomes of 2996 women treated with breast-conserving surgery over 30 years. Ann Surg Oncol. 2016;23(9):2816–24.
Fisher B, Dignam J, Wolmark N, et al. Tamoxifen in treatment of intraductal breast cancer: National Surgical Adjuvant Breast and Bowel Project B-24 randomised controlled trial. Lancet. 1999;353(9169):1993–2000.
Ringberg A, Nordgren H, Thorstensson S, et al. Histopathological risk factors for ipsilateral breast events after breast conserving treatment for ductal carcinoma in situ of the breast–results from the Swedish randomised trial. Eur J Cancer. 2007;43(2):291–8.
Van Zee KJ, Liberman L, Samli B, et al. Long term follow-up of women with ductal carcinoma in situ treated with breast-conserving surgery: the effect of age. Cancer. 1999;86(9):1757–67.
Allred DC, Anderson SJ, Paik S, et al. Adjuvant tamoxifen reduces subsequent breast cancer in women with estrogen receptor-positive ductal carcinoma in situ: a study based on NSABP protocol B-24. J Clin Oncol. 2012;30(12):1268–73.
Cuzick J, Sestak I, Pinder SE, et al. Effect of tamoxifen and radiotherapy in women with locally excised ductal carcinoma in situ: long-term results from the UK/ANZ DCIS trial. Lancet Oncol. 2011;12(1):21–9.
Donker M, Litiere S, Werutsky G, et al. Breast-conserving treatment with or without radiotherapy in ductal carcinoma In Situ: 15-year recurrence rates and outcome after a recurrence, from the EORTC 10853 randomized phase III trial. J Clin Oncol. 2013;31(32):4054–9.
Wapnir IL, Dignam JJ, Fisher B, et al. Long-term outcomes of invasive ipsilateral breast tumor recurrences after lumpectomy in NSABP B-17 and B-24 randomized clinical trials for DCIS. J Natl Cancer Inst. 2011;103(6):478–88.
Warnberg F, Garmo H, Emdin S, et al. Effect of radiotherapy after breast-conserving surgery for ductal carcinoma in situ: 20 years follow-up in the randomized SweDCIS Trial. J Clin Oncol. 2014;32(32):3613–8.
Claus EB, Stowe M, Carter D, Holford T. The risk of a contralateral breast cancer among women diagnosed with ductal and lobular breast carcinoma in situ: data from the Connecticut Tumor Registry. Breast. 2003;12(6):451–6.
Innos K, Horn-Ross PL. Risk of second primary breast cancers among women with ductal carcinoma in situ of the breast. Breast Cancer Res Treat. 2008;111(3):531–40.
Flanagan MR, Rendi MH, Gadi VK, Calhoun KE, Gow KW, Javid SH. Adjuvant endocrine therapy in patients with ductal carcinoma in situ: a population-based retrospective analysis from 2005 to 2012 in the National Cancer Data Base. Ann Surg Oncol. 2015;22(10):3264–72.
Karavites LC, Kane AK, Zaveri S, et al. Tamoxifen acceptance and adherence among patients with ductal carcinoma in situ (DCIS) treated in a multidisciplinary setting. Cancer Prev Res (Phila). 2017;10(7):389–97.
Livaudais JC, Hwang ES, Karliner L, et al. Adjuvant hormonal therapy use among women with ductal carcinoma in situ. J Womens Health (Larchmt). 2012;21(1):35–42.
Narod SA, Iqbal J, Giannakeas V, Sopik V, Sun P. Breast cancer mortality after a diagnosis of ductal carcinoma in situ. JAMA Oncol. 2015;1(7):888–96.
Nichols HB, Bowles EJ, Islam J, et al. Tamoxifen initiation after ductal carcinoma in situ. Oncologist. 2016;21(2):134–40.
McCormick B, Winter K, Hudis C, et al. RTOG 9804: a prospective randomized trial for good-risk ductal carcinoma in situ comparing radiotherapy with observation. J Clin Oncol. 2015;33(7):709–15.
Pilewskie M, Stempel M, Rosenfeld H, Eaton A, Van Zee KJ, Morrow M. Do LORIS Trial eligibility criteria identify a ductal carcinoma in situ patient population at low risk of upgrade to invasive carcinoma? Ann Surg Oncol. 2016;23(11):3487–93.
Acknowledgment
The preparation of this study was funded in part by NIH/NCI Cancer Center Support Grant No. P30 CA008748 to Memorial Sloan Kettering Cancer Center. This study was presented in poster format at the 41st Annual San Antonio Breast Cancer Symposium, December 4–8, 2018, San Antonio, TX.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Dr. Kimberly J. Van Zee has served on the Advisory Board of Genomic Health.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Miller, M.E., Muhsen, S., Zabor, E.C. et al. Risk of Contralateral Breast Cancer in Women with Ductal Carcinoma In Situ Associated with Synchronous Ipsilateral Lobular Carcinoma In Situ. Ann Surg Oncol 26, 4317–4325 (2019). https://doi.org/10.1245/s10434-019-07796-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-019-07796-9