
Abstract
Background
The goal of the present study was to determine the actual incidence, predictive risk factors, and clinical characteristics of levothyroxine supplementation (LT4S) used for the management of hypothyroidism after hemithyroidectomy.
Methods
From 2008 to 2015, we included 535 patients who underwent hemithyroidectomy. LT4S was initiated based on three major criteria: the development of overt hypothyroidism, subclinical hypothyroidism with thyroid-stimulating hormone (TSH) levels > 10 mIU/L, or subclinical hypothyroidism with TSH levels of 4.5–10 mIU/L with associated signs/symptoms.
Results
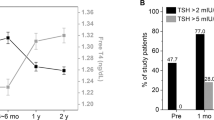
During the 69-month follow-up period, 321 patients (60%) developed overall hypothyroidism following hemithyroidectomy, and 141 ultimately required LT4S, with an overall LT4S incidence of 26.4%. The most common cause of LT4S initiation was subclinical hypothyroidism with TSH levels > 10 mIU/L. In 141 patients with LT4S, the mean maintenance dose of levothyroxine was 1.34 μg/kg, and only 6 patients (4.3%) discontinued LT4S during the follow-up. The 1-, 3-, 5-, and 7-year LT4S-free survival rates of 535 patients were 88.6%, 80.2%, 73.8%, and 69.1%, respectively. Preoperative TSH levels > 2.12 mIU/L and coexistence of Hashimoto’s thyroiditis were significantly associated with LT4S following hemithyroidectomy. The risk of LT4S increased by 1.401 times, as preoperative TSH levels increased by 1 mIU/L.
Discussion
A quarter of patients required LT4S after hemithyroidectomy for the management of hypothyroidism, with a mean maintenance levothyroxine dose of 1.34 μg/kg. The preoperative TSH level and coexistence of Hashimoto’s thyroiditis were significant predictive factors of LT4S following hemithyroidectomy.


Similar content being viewed by others


References
Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26(1):1–133.
Perros P, Boelaert K, Colley S, et al. Guidelines for the management of thyroid cancer. Clin Endocrinol (Oxf). 2014;81(Suppl 1):1–122.
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)—Thyroid Carcinoma v. 2. National Comprehensive Cancer Network. 2018.
Su SY, Grodski S, Serpell JW. Hypothyroidism following hemithyroidectomy: a retrospective review. Ann Surg. 2009;250(6):991–4.
Verloop H, Louwerens M, Schoones JW, Kievit J, Smit JW, Dekkers OM. Risk of hypothyroidism following hemithyroidectomy: systematic review and meta-analysis of prognostic studies. J Clin Endocrinol Metab. 2012;97(7):2243–55.
Said M, Chiu V, Haigh PI. Hypothyroidism after hemithyroidectomy. World J Surg. 2013;37(12):2839–44.
Ahn D, Sohn JH, Jeon JH. Hypothyroidism following hemithyroidectomy: incidence, risk factors, and clinical characteristics. J Clin Endocrinol Metab. 2016;101(4):1429–36.
Park S, Jeon MJ, Song E, et al. Clinical features of early and late postoperative hypothyroidism after lobectomy. J Clin Endocrinol Metab. 2017;102(4):1317–24.
Stoll SJ, Pitt SC, Liu J, Schaefer S, Sippel RS, Chen H. Thyroid hormone replacement after thyroid lobectomy. Surgery. 2009;146(4):554–8 (discussion 558-60).
Lee DY, Seok J, Jeong WJ, Ahn SH. Prediction of thyroid hormone supplementation after thyroid lobectomy. J Surg Res. 2015;193(1):273–8.
Ng P, Ho C, Tan WB, et al. Predictors of thyroxine replacement following hemithyroidectomy in a south east Asian cohort. Head Neck. 2018;41(5):1463–7.
Turner MR, Camacho X, Fischer HD, et al. Levothyroxine dose and risk of fractures in older adults: nested case-control study. BMJ. 2011;342:d2238.
Freudenthal B, Williams GR. Thyroid-stimulating hormone suppression in the long-term follow-up of differentiated thyroid cancer. Clin Oncol (R Coll Radiol). 2017;29(5):325–8.
Shin DW, Suh B, Lim H, Yun JM, Song SO, Park Y. J-shaped association between postoperative levothyroxine dosage and fracture risk in thyroid cancer patients: a retrospective cohort study. J Bone Miner Res. 2018;33(6):1037–43.
Cox C, Bosley M, Southerland LB, et al. Lobectomy for treatment of differentiated thyroid cancer: can patients avoid postoperative thyroid hormone supplementation and be compliant with the American Thyroid Association guidelines? Surgery. 2018;163(1):75–80.
Col NF, Surks MI, Daniels GH. Subclinical thyroid disease: clinical applications. JAMA. 2004;291(2):239–43.
Surks MI, Ortiz E, Daniels GH, et al. Subclinical thyroid disease: scientific review and guidelines for diagnosis and management. JAMA. 2004;291(2):228–38.
Jin J, Allemang MT, McHenry CR. Levothyroxine replacement dosage determination after thyroidectomy. Am J Surg. 2013;205(3):360–3 (discussion 363-4).
Ha TK, Kim DW, Park HK, et al. The effect of levothyroxine discontinuation timing on postoperative hypothyroidism after hemithyroidectomy for papillary thyroid microcarcinoma. Int J Endocrinol. 2016;2016:3240727.
Cooper DS, Specker B, Ho M, et al. Thyrotropin suppression and disease progression in patients with differentiated thyroid cancer: results from the National Thyroid Cancer Treatment Cooperative Registry. Thyroid. 1998;8(9):737–44.
Brabant G. Thyrotropin suppressive therapy in thyroid carcinoma: what are the targets? J Clin Endocrinol Metab. 2008;93(4):1167–9.
Bilimoria KY, Bentrem DJ, Ko CY, et al. Extent of surgery affects survival for papillary thyroid cancer. Ann Surg. 2007;246(3):375–81 (discussion 381-4).
Barney BM, Hitchcock YJ, Sharma P, Shrieve DC, Tward JD. Overall and cause-specific survival for patients undergoing lobectomy, near-total, or total thyroidectomy for differentiated thyroid cancer. Head Neck. 2011;33(5):645–9.
Li X, Zhao C, Hu D, et al. Hemithyroidectomy increases the risk of disease recurrence in patients with ipsilateral multifocal papillary thyroid carcinoma. Oncol Lett. 2013;5(4):1412–6.
Park YM, Lee DY, Oh KH, et al. Clinical implications of pathologic factors after thyroid lobectomy in patients with papillary thyroid carcinoma. Oral Oncol. 2017;75:1–5.
Son HJ, Kim JK, Jung YD, et al. Comparison of outcomes between hemithyroidectomy alone and hemithyroidectomy with elective unilateral central neck dissection in patients with papillary thyroid microcarcinoma. Head Neck. 2018;40(11):2449–54.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Ahn, D., Lee, G.J. & Sohn, J.H. Levothyroxine Supplementation Following Hemithyroidectomy: Incidence, Risk Factors, and Characteristics. Ann Surg Oncol 26, 4405–4413 (2019). https://doi.org/10.1245/s10434-019-07786-x
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-019-07786-x