
Abstract
Background
Definitive chemoradiation therapy or chemotherapy alone is generally recommended for patients with unresectable cT4b esophageal cancer. However, conversion surgery has emerged as a therapeutic option when downstaging is achieved by induction therapy.
Methods
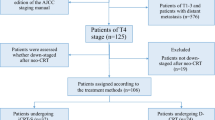
We studied 169 patients with cT4 esophageal cancer who underwent induction therapy. Survival and prognostic factors were examined.
Results
Of 169 patients, 25 who achieved a clinical complete response (cCR) underwent surveillance, 72 patients underwent conversion surgery, while another 72 patients whose tumors were regarded as unresectable after induction therapy did not undergo surgery. Among 169 patients, the 3- and 5-year survival rates were 31.0% and 25.9%, respectively. Sixty-four patients who underwent curative resection showed better survival comparable with survival of 25 patients who achieved cCR (3- and 5-year survival; 56.8% and 48.6% versus 64.0% and 52.0%, respectively). However, the survival of eight patients who underwent noncurative resection was as dismal as that of patients who did not undergo conversion surgery. Multivariate analysis in 169 patients identified female sex and achieving cCR or R0 resection as independent prognostic factors. Multivariate analysis in 72 patients who underwent conversion surgery identified sex, lymph node status, and R0 resection as independent prognostic factors in patients with cT4b esophageal cancer.
Conclusions
The present study showed that conversion surgery after induction therapy can be a potentially curative treatment option for select patients with cT4b esophageal cancer. An important issue for further research is to establish a method for more accurately diagnosing tumor resectability after induction therapy for cT4b esophageal cancer.


Similar content being viewed by others


References
Tepper J, Krasna MJ, Niedzwiecki D, et al. Phase III trial of trimodality therapy with cisplatin, fluorouracil, radiotherapy, and surgery compared with surgery alone for esophageal cancer: CALGB 9781. J Clin Oncol 2008; 26: 1086–1092.
Gebski V, Burmeister B, Smithers BM, et al. Survival benefits from neoadjuvant chemoradiotherapy or chemotherapy in oesophageal carcinoma: a meta-analysis. Lancet Oncol. 2007; 8: 226–234.
van Hagen P, Hulshof MC, van Lanschot JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012; 366: 2074–2084.
Medical Research Council Oesophageal Cancer Working Group. Surgical resection with or without preoperative chemotherapy in oesophageal cancer: a randomised controlled trial. Lancet 2002; 359: 1727–1733.
Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006; 355: 11–20.
Miyata H, Yamasaki M, Miyazaki Y, et al. Clinical Importance of Supraclavicular Lymph Node Metastasis After Neoadjuvant Chemotherapy for Esophageal Squamous Cell Carcinoma. Ann Surg. 2015; 262: 280–285.
NCCN Guidelines Esophageal and Esophagogastric Junction Cancers, Version 2. 2018. Available at: https://www.nccn.org/patients.
Guidelines for Diagnosis and Treatment of Carcinoma of the Esophagus 2017: The Japan Esophageal Society. Tokyo: Kanehara Shuppan; 2017.
Nishimura Y, Suzuki M, Nakamatsu K, Kanamori S, Yagyu Y, Shigeoka H. Prospective trial of concurrent chemoradiotherapy with protracted infusion of 5-fluorouracil and cisplatin for T4 esophageal cancer with or without fistula. Int J Radiat Oncol Biol Phys. 2002; 53: 134–139.
Ohtsu A, Boku N, Muro K, et al. Definitive chemoradiotherapy for T4 and/or M1 lymph node squamous cell carcinoma of the esophagus. J Clin Oncol. 1999; 17: 2915–2921.
Cushman TR, Shaaban SG, Moreno AC, Lin C, Verma V. Management of Unresectable T4b Esophageal Cancer: Practice Patterns and Outcomes From the National Cancer Data Base. Am J Clin Oncol. 2019; 42: 154–159.
Ishida K, Ando N, Yamamoto S, Ide H, Shinoda M. Phase II study of cisplatin and 5-fluorouracil with concurrent radiotherapy in advanced squamous cell carcinoma of the esophagus: a Japan Esophageal Oncology Group (JEOG)/Japan Clinical Oncology Group trial (JCOG9516). Jpn J Clin Oncol. 2004; 34:615–619.
Kaneko K, Ito H, Konishi K, et al. Definitive chemoradiotherapy for patients with malignant stricture due to T3 or T4 squamous cell carcinoma of the oesophagus. Br J Cancer. 2003; 88:18–24.
Ikeda K, Ishida K, Sato N, et al. Chemoradiotherapy followed by surgery for thoracic esophageal cancer potentially or actually involving adjacent organs. Dis Esophagus. 2001; 14:197–201.
Noguchi T, Moriyama H, Wada S, et al. Resection surgery with neoadjuvant chemoradiotherapy improves outcomes of patients with T4 esophageal carcinoma. Dis Esophagus. 2003;16: 94–98.
Van Raemdonck D, Van Cutsem E, Menten J, et al. Induction therapy for clinical T4 oesophageal carcinoma; a plea for continued surgical exploration. Eur J Cardiothorac Surg. 1997; 11: 828–837.
de Manzoni G, Pedrazzani C, Pasini F, et al. Chemoradiotherapy followed by surgery for squamous cell carcinoma of the thoracic esophagus with clinical evidence of adjacent organ invasion. J Surg Oncol. 2007; 95: 261–266.
Yano M, Shiozaki H, Tsujinaka T, et al. Squamous cell carcinoma of the esophagus infiltrating the respiratory tract is less sensitive to preoperative concurrent radiation and chemotherapy. J Am Coll Surg. 2000;191: 626–634.
Yokota T, Kato K, Hamamoto Y, et al. Phase II study of chemoselection with docetaxel plus cisplatin and 5-fluorouracil induction chemotherapy and subsequent conversion surgery for locally advanced unresectable oesophageal cancer. Br J Cancer. 2016; 115:1328–1334.
Motoori M, Yano M, Ishihara R, et al. Comparison between radical esophagectomy and definitive chemoradiotherapy in patients with clinical T1bN0M0 esophageal cancer. Ann Surg Oncol. 2012; 19: 2135–2141.
Sugimura K, Miyata H, Yano M, et al. Is 18F-FDG-PET useful for predicting R0 resection after induction therapy for initially unresectable locally advanced esophageal carcinoma? Gen Thorac Cardiovasc Surg. 2017; 65: 455–462.
Miyata H, Sugimura K, Yamasaki M, et al. Clinical Impact of the Location of Lymph Node Metastases After Neoadjuvant Chemotherapy for Middle and Lower Thoracic Esophageal Cancer. Ann Surg Oncol. 2019; 26: 200–208.
Japanese Classification of Esophageal Cancer. 11th edition. The Japan Esophageal Society. Tokyo: Kanehara Shuppan; 2015.
Miyata H, Yamasaki M, Takiguchi S, et al. Prognostic value of endoscopic biopsy findings after induction chemoradiotherapy with and without surgery for esophageal cancer. Ann Surg. 2010; 253: 279–284.
Brierley J, Gospodarowicz M, Wittekind C. TNM Classification of Malignant Tumours. 8th edition. Oxford: Wiley; 2017.
Ancona E, Ruol A, Castoro C, et al. First-line chemotherapy improves the resection rate and long-term survival of locally advanced (T4, any N, M0) squamous cell carcinoma of the thoracic esophagus: final report on 163 consecutive patients with 5-year follow-up. Ann Surg. 1997; 226: 714–723.
Ishikawa K, Nakamatsu K, Shiraishi O, Yasuda T, Nishimura Y. Clinical results of definitive-dose (50 Gy/25 fractions) preoperative chemoradiotherapy for unresectable esophageal cancer. Int J Clin Oncol. 2015; 20: 531–537.
Tachibana M, Dhar DK, Kinugasa S, et al. Surgical treatment for locally advanced (T4) squamous cell carcinoma of the thoracic esophagus. Dysphagia. 2002; 17: 255–261.
Piessen G, Messager M, Mirabel X, et al. Is there a role for surgery for patients with a complete clinical response after chemoradiation for esophageal cancer? An intention-to-treat case-control study. Ann Surg. 2013; 258: 793–799.
Karimata H, Shimoji H, Nishimaki T. Clinicopathological factors predicting R0 resection and long-term survival after esophagectomy in patients with T4 esophageal cancer undergoing induction chemotherapy or chemoradiotherapy. Surg Today. 2015; 45: 479–486.
van der Werf LR, Dikken JL, van der Willik EM, et al. Time interval between neoadjuvant chemoradiotherapy and surgery for oesophageal or junctional cancer: a nationwide study. Eur J Cancer. 2018; 91: 76–85.
Shaikh T, Ruth K, Scott WJ, et al. Increased time from neoadjuvant chemoradiation to surgery is associated with higher pathologic complete response rates in esophageal cancer. Ann Thorac Surg. 2015; 99: 270–276.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Miyata, H., Sugimura, K., Motoori, M. et al. Clinical Implications of Conversion Surgery After Induction Therapy for T4b Thoracic Esophageal Squamous Cell Carcinoma. Ann Surg Oncol 26, 4737–4743 (2019). https://doi.org/10.1245/s10434-019-07727-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-019-07727-8