
Abstract
Background
In the current guidelines for differentiated thyroid cancer (DTC), computed tomography (CT) of the neck has a limited role. The authors hypothesized that adding CT to the workup of clinically low-risk DTC size 4 cm or smaller changes the surgical management for a portion of patients due to detection of clinically significant lymph node metastases not located by ultrasound of the neck.
Methods
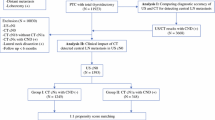
A prospective cohort of DTC patients at an academic referral center between 2012 and 2016 was reviewed. All the patients with fine-needle aspiration cytopathology results suspicious for malignancy or malignant tumor (Bethesda category 5 or 6, respectively) underwent CT before surgery. Clinically low-risk DTC patients were selected if they had a tumor diameter of 4 cm or less and no evidence for local invasion or suspicious lymph nodes seen on ultrasound. Outcomes focused on alteration of the surgical plan based on CT and correlation with pathology.
Results
The CT findings for 25 (22.5%) of 111 patients with clinically low-risk DTC led to a change in surgical management. Of these 25 patients, 16 (14.4% of the entire cohort) benefited due to the removal of clinically significant lymph node disease not seen on ultrasound. Categorization of the group that had a change in management showed that 6 (85.7%) of 7 lateral neck dissections and 10 (55.6%) of 18 central neck dissections (CND) harbored metastatic nodes larger than 2 mm.
Conclusions
In the group with clinically low-risk DTC, CT changed surgical management for a substantial number of the patients with clinically significant nodal disease not detected by ultrasound. This highlights the fact that in certain practice settings, adding CT to the preoperative staging may be favorable for the detection of nodal metastasis.

Similar content being viewed by others


References
Davies L, Morris LG, Haymart M, et al. American Association of Clinical Endocrinologists and American College of Endocrinology Disease state clinical review: the increasing incidence of thyroid cancer. Endocrine Practice. 2015;21:686–96.
Davies L, Welch H. Thyroid cancer survival in the United States: observational data from 1973 to 2005. Arch Otolaryngol Head Neck Surg. 2010;136:440–4.
Lim H, Devesa SS, Sosa JA, Check D, Kitahara CM. Trends in thyroid cancer incidence and mortality in the United States, 1974–2013. JAMA. 2017;317:1338–48.
Nixon IJ, Wang LY, Migliacci JC, et al. An international multi-institutional validation of age 55 years as a cutoff for risk stratification in the AJCC/UICC staging system for well-differentiated thyroid cancer. Thyroid. 2016;26:373–80.
Choi JS, Kim J, Kwak JY, Kim MJ, Chang HS, Kim E-KK. Preoperative staging of papillary thyroid carcinoma: comparison of ultrasound imaging and CT. AJR Am J Roentgenol. 2009;193:871–8.
Lee DY, Kwon T-KK, Sung M-WW, Kim KH, Hah JH. Prediction of extrathyroidal extension using ultrasonography and computed tomography. Int J Endocrinol. 2014. https://doi.org/10.1155/2014/351058.
Choi J, Chung W, Kwak J, Moon H, Kim M, Kim E-K. Staging of papillary thyroid carcinoma with ultrasonography: performance in a large series. Ann Surg Oncol. 2011;18:3572–8.
Gonzalez HE, Cruz F, O’Brien A, et al. Impact of preoperative ultrasonographic staging of the neck in papillary thyroid carcinoma. Arch Otolaryngol Head Neck Surg. 2007;133:1258–62.
Kouvaraki MA, Shapiro SE, Fornage BD, et al. Role of preoperative ultrasonography in the surgical management of patients with thyroid cancer. Surgery. 2003;134:946.
Stulak JM, Grant CS, Farley DR, et al. Value of preoperative ultrasonography in the surgical management of initial and reoperative papillary thyroid cancer. Arch Surg. 2006;141:486–9.
Ahn J, Lee J, Yi J, et al. Diagnostic accuracy of CT and ultrasonography for evaluating metastatic cervical lymph nodes in patients with thyroid cancer. World J Surg. 2008;32:1552.
Kim E PJ, Son K-R, Kim J-H, Jeon SJ, Na DG. Preoperative diagnosis of cervical metastatic lymph nodes in papillary thyroid carcinoma: comparison of ultrasound, computed tomography, and combined ultrasound with computed tomography. Thyroid. 2008;18:411–8.
Lee DW, Ji YB, Sung ES, et al. Roles of ultrasonography and computed tomography in the surgical management of cervical lymph node metastases in papillary thyroid carcinoma. Eur J Surg Oncol. 2013;39:191–6.
Lesnik D, Cunnane ME, Zurakowski D, et al. Papillary thyroid carcinoma nodal surgery directed by a preoperative radiographic map utilizing CT scan and ultrasound in all primary and reoperative patients. Head Neck. 2014;36:191–202.
Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients With thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26:1–133.
Cibas ES, Ali SZ. The Bethesda system for reporting thyroid cytopathology. Am J Clin Pathol. 2009;132:658–65.
Kim SK, Woo J-WW, Park I, et al. Computed tomography-detected central lymph node metastasis in ultrasonography node-negative papillary thyroid carcinoma: is it really significant? Ann Surg Oncol. 2017;24:442–9.
Hartl DM, Leboulleux S, Vélayoudom-Céphise F-LL, Mirghani H, Déandréis D, Schlumberger M. Management of retropharyngeal node metastases from thyroid carcinoma. World J Surg. 2015;39:1274–81.
Togashi T, Sugitani I, Toda K, Kawabata K, Takahashi S. Surgical management of retropharyngeal nodes metastases from papillary thyroid carcinoma. World J Surg. 2014;38:2831–7.
Adam MA, Thomas S, Youngwirth L, et al. Is there a minimum number of thyroidectomies a surgeon should perform to optimize patient outcomes? Ann Surg. 2017;265:402–7.
Oltmann SC, Schneider DF, Chen H, Sippel RS. All thyroid ultrasound evaluations are not equal: sonographers specialized in thyroid cancer correctly label clinical N0 disease in well-differentiated thyroid cancer. Ann Surg Oncol. 2015;22:422–8.
Rosario PW. Ultrasonography for the follow-up of patients with papillary thyroid carcinoma: how important is the operator? Thyroid. 2010;20:833–4.
Smith-Bindman R, Lipson J, Marcus R, et al. Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer. Arch Intern Med. 2009;169:2078–86.
Mishra A, Pradhan P, Gambhir S, Sabaretnam M, Gupta A, Babu S. Preoperative contrast-enhanced computerized tomography should not delay radioiodine ablation in differentiated thyroid carcinoma patients. J Surg Res. 2015;193:731–7.
Padovani RP, Kasamatsu TS, Nakabashi CCD, et al. One month is sufficient for urinary iodine to return to its baseline value after the use of water-soluble iodinated contrast agents in post-thyroidectomy patients requiring radioiodine therapy. Thyroid. 2012;22:926–30.
Sohn S, Choi J, Kim N, et al. The impact of iodinated contrast agent administered during preoperative computed tomography scan on body iodine pool in patients with differentiated thyroid cancer preparing for radioactive iodine treatment. Thyroid. 2014;24:872–7.
Hong Y, Lee S, Lim D, et al. The stratification of patient risk depending on the size and ratio of metastatic lymph nodes in papillary thyroid carcinoma. World J Surg Oncol. 2017;15:74.
Lang B, Tang AH, Wong K, Shek TW, Wan K, Lo C-Y. Significance of size of lymph node metastasis on postsurgical stimulated thyroglobulin levels after prophylactic unilateral central neck dissection in papillary thyroid carcinoma. Ann Surg Oncol. 2012;19:3472–8.
Ito Y, Miyauchi A, Inoue H, et al. An observational trial for papillary thyroid microcarcinoma in Japanese patients. World J Surg. 2009;34:28–35.
Wada N, Masudo K, Nakayama H, et al. Clinical outcomes in older or younger patients with papillary thyroid carcinoma: impact of lymphadenopathy and patient age. Eur J Surg Oncol. 2008;34:202–7.
Bardet S, Malville E, Rame J-P, et al. Macroscopic lymph node involvement and neck dissection predict lymph node recurrence in papillary thyroid carcinoma. Eur J Endocrinol. 2008;158:551–60.
Randolph GW, Duh Q-YY, Heller KS, et al. The prognostic significance of nodal metastases from papillary thyroid carcinoma can be stratified based on the size and number of metastatic lymph nodes, as well as the presence of extranodal extension. Thyroid. 2012;22:1144–52.
Vaisman F, Tala H, Grewal R, Tuttle MR. In differentiated thyroid cancer, an incomplete structural response to therapy is associated with significantly worse clinical outcomes than only an incomplete thyroglobulin response. Thyroid. 2011;21:1317–22.
Wang LY, Roman BR, Migliacci JC, et al. Cost-effectiveness analysis of papillary thyroid cancer surveillance. Cancer. 2015;121:4132–40.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bongers, P.J., Verzijl, R., Dzingala, M. et al. Preoperative Computed Tomography Changes Surgical Management for Clinically Low-Risk Well-Differentiated Thyroid Cancer. Ann Surg Oncol 26, 4439–4444 (2019). https://doi.org/10.1245/s10434-019-07618-y
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-019-07618-y