
Abstract
Background
Patients with epidermal growth factor receptor 2-positive (HER2+) breast cancer and pathologic complete response (pCR) after neoadjuvant systemic therapy (NST) may be candidates for nonoperative clinical trials if residual invasive and in situ disease are eradicated.
Methods
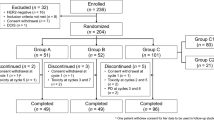
This study analyzed 280 patients with clinical T1-2N0-1 HER2+ breast cancer who underwent NST followed by surgical resection to determine key characteristics of patients with pCR in the breast and lymph nodes compared with those with residual disease.
Results
Of the 280 patients, 102 (36.4%) had pCR in the breast and lymph nodes after NST, and 50 patients (17.9%) had residual ductal carcinoma in situ (DCIS) in the breast only. For 129 patients (46.1%), DCIS was present on the pretreatment biopsy, and NST failed to eradicate the DCIS component in 64.3%. Patients with residual disease were more likely to have hormone receptor-positive (HR+) tumors than those with negative tumors (73.4% vs. 50.8%; p < 0.0001). Radiologic response (odds ratio [OR], 5.62; p = 0.002) and HR+ status (OR, 2.56; p < 0.0001) were predictive of residual disease. Combined imaging methods after NST had a sensitivity of 97.1% and a negative predictive value of 70.6% for detection of residual disease. Patients with invasive disease and DCIS shown on the pretreatment core biopsy were less likely than those without DCIS to achieve pCR in the breast (31% vs. 43%; p = 0.038).
Conclusion
The study results delineate and identify unique characteristics associated with HER2+ breast cancers that are important in selecting patients for inclusion in clinical trials assessing nonoperative management after NST, and the low negative predictive value of imaging mandates image-guided biopsy for selection.
Similar content being viewed by others


References
Untch M, Rezai M, Loibl S, et al. Neoadjuvant treatment with trastuzumab in HER2-positive breast cancer: results from the GeparQuattro study. J Clin Oncol. 2010;28:2024–31.
Gianni L, Eiermann W, Semiglazov V, et al. Neoadjuvant chemotherapy with trastuzumab followed by adjuvant trastuzumab versus neoadjuvant chemotherapy alone in patients with HER2-positive locally advanced breast cancer (the NOAH trial): a randomised controlled superiority trial with a parallel HER2-negative cohort. Lancet. 2010;375:377–84.
Untch M, Fasching PA, Konecny GE, et al. Pathologic complete response after neoadjuvant chemotherapy plus trastuzumab predicts favorable survival in human epidermal growth factor receptor 2-overexpressing breast cancer: results from the TECHNO trial of the AGO and GBG study groups. J Clin Oncol. 2011;29:3351–7.
Mariani G, Fasolo A, De Benedictis E, Gianni L. Trastuzumab as adjuvant systemic therapy for HER2-positive breast cancer. Nat Clin Pract Oncol. 2009;6:93–104.
Buzdar AU, Valero V, Ibrahim NK, et al. Neoadjuvant therapy with paclitaxel followed by 5-fluorouracil, epirubicin, and cyclophosphamide chemotherapy and concurrent trastuzumab in human epidermal growth factor receptor 2-positive operable breast cancer: an update of the initial randomized study population and data of additional patients treated with the same regimen. Clin Cancer Res. 2007;13:228–33.
Tanioka M, Sasaki M, Shimomura A, et al. Pathologic complete response after neoadjuvant chemotherapy in HER2-overexpressing breast cancer according to hormonal receptor status. Breast. 2014;23:466–72.
Kim MM, Allen P, Gonzalez-Angulo AM, et al. Pathologic complete response to neoadjuvant chemotherapy with trastuzumab predicts for improved survival in women with HER2-overexpressing breast cancer. Ann Oncol. 2013;24:1999–2004.
Sanchez-Munoz A, Navarro-Perez V, Plata-Fernandez Y, et al. Proliferation determined by Ki-67 defines different pathologic response to neoadjuvant trastuzumab-based chemotherapy in HER2-positive breast cancer. Clin Breast Cancer. 2015;15:343–7.
Hamy AS, Pierga JY, Sabaila A, et al. Stromal lymphocyte infiltration after neoadjuvant chemotherapy is associated with aggressive residual disease and lower disease-free survival in HER2-positive breast cancer. Ann Oncol. 2017;28:2233–40.
von Minckwitz G, Untch M, Blohmer JU, et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol. 2012;30:1796–804.
Kuerer HM, Rauch GM, Krishnamurthy S, et al. A clinical feasibility trial for identification of exceptional responders in whom breast cancer surgery can be eliminated following neoadjuvant systemic therapy. Ann Surg. 2018;267:946–51.
van la Parra RFD, Tadros AB, Checka CM, et al. Baseline factors predicting a response to neoadjuvant chemotherapy with implications for non-surgical management of triple-negative breast cancer. Br J Surg. 2018;105:535–43.
Hamy-Petit AS, Belin L, Bonsang-Kitzis H, et al. Pathological complete response and prognosis after neoadjuvant chemotherapy for HER2-positive breast cancers before and after trastuzumab era: results from a real-life cohort. Br J Cancer. 2016;114:44–52.
Natoli C, Vici P, Sperduti I, et al. Effectiveness of neoadjuvant trastuzumab and chemotherapy in HER2-overexpressing breast cancer. J Cancer Res Clin Oncol. 2013;139:1229–40.
Jung YY, Hyun CL, Jin MS, et al. Histomorphological factors predicting the response to neoadjuvant chemotherapy in triple-negative breast cancer. J Breast Cancer. 2016;19:261–7.
Kraus JA, Beriwal S, Dabbs DJ, et al. Predictors of pathologic complete response after standard neoadjuvant chemotherapy in triple-negative breast carcinoma. Appl Immunohistochem Mol Morphol. 2012;20:334–9.
Masuda H, Masuda N, Kodama Y, et al. Predictive factors for the effectiveness of neoadjuvant chemotherapy and prognosis in triple-negative breast cancer patients. Cancer Chemother Pharmacol. 2011;67:911–7.
Tadros AB, Yang WT, Krishnamurthy S, et al. Identification of patients with documented pathologic complete response in the breast after neoadjuvant chemotherapy for omission of axillary surgery. JAMA Surg. 2017;152:665–70.
Caudle AS, Kuerer HM, Krishnamurthy S, et al. Feasibility of fine-needle aspiration for assessing responses to chemotherapy in metastatic nodes marked with clips in breast cancer: a prospective registry study. Cancer. 2019;125(3):365–73.
Kuerer HM. Eliminating breast cancer surgery in exceptional responders with neoadjuvant systemic therapy 2018. Retrieved May 6, 2019 from https://clinicaltrials.gov/ct2/show/NCT02945579.
Acknowledgment
This work was supported by the PH and Fay Etta Robinson Distinguished Professorship in Cancer Research (HMK) and a cancer center support grant from the National Institutes of Health (NIH) (CA16672).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
There are no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sun, S., van la Parra, R.F.D., Rauch, G.M. et al. Patient Selection for Clinical Trials Eliminating Surgery for HER2-Positive Breast Cancer Treated with Neoadjuvant Systemic Therapy. Ann Surg Oncol 26, 3071–3079 (2019). https://doi.org/10.1245/s10434-019-07533-2
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-019-07533-2