
Abstract
Background
Current recommendations for persistent or recurrent locoregional papillary thyroid cancer (PTC) include consideration of surgical resection versus active surveillance. The purpose of this study is to determine long-term outcomes after surgical resection of recurrent or persistent metastatic PTC in cervical lymph nodes after failure of initial surgery and radioactive iodine therapy using newer validated clinical outcomes measures.
Methods
Outcomes of 70 patients who underwent cervical lymphadenectomy (n = 110) from 1999 to 2013 for recurrent or persistent locoregional PTC metastases were reviewed. Measures included biochemical remission (BCR) based on Tg levels, American Thyroid Association classifications for response to treatment [biochemical incomplete response (BIR), structural incomplete response (SIR), indeterminate response (IR), and excellent response (ER)], need for reoperation, surgical complications, disease progression, and death.
Results
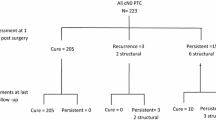
The median follow-up was 13.1 years, with only two additional reoperations since 2010, one of which had no metastasis on pathology with the other developing anaplastic thyroid cancer in background PTC. ER was achieved in 31 (44%) patients, all of whom remained in ER at time of last follow-up (median 14.1 years). There were no structural recurrences in patients with persistent BIR or IR after reoperation. Patients with SIR had stable disease, except for one who died due to anaplastic thyroid cancer.
Conclusions
Patients who achieved ER after reoperation had no need for further treatment. Patients with persistent detectable Tg levels after reoperation rarely developed structural recurrence. ATA outcomes can be safely used to guide treatment decisions over a decade after reoperation for PTC.


Similar content being viewed by others


References
Nguyen QT, Lee EJ, Huang MG, Park YI, Khullar A, Plodkowski RA. Diagnosis and treatment of patients with thyroid cancer. Am Health Drug Benefits. 2015;8(1):30–40.
Cancer Facts and Figures. 2018. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2018/cancer-facts-and-figures-2018.pdf. Accessed 27 August 2018.
Kloos RT. Papillary thyroid cancer: medical management and follow-up. Curr Treat Options Oncol. 2005;6(4):323–338.
Kloos RT, Mazzaferri EL. A single recombinant human thyrotropin-stimulated serum thyroglobulin measurement predicts differentiated thyroid carcinoma metastases three to five years later. J Clin Endocrinol Metab. 2005;90(9):5047–5057.
Cooper DS, Doherty GM, Haugen BR, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19(11):1167–1214..
Schlumberger MJ. Papillary and follicular thyroid carcinoma. N Engl J Med. 1998;338(5):297–306.
Tuttle RM, Tala H, Shah J, et al. Estimating risk of recurrence in differentiated thyroid cancer after total thyroidectomy and radioactive iodine remnant ablation: using response to therapy variables to modify the initial risk estimates predicted by the new American Thyroid Association staging system. Thyroid. 2010;20(12):1341–1349.
Yim JH, Kim WB, Kim EY, et al. The outcomes of first reoperation for locoregionally recurrent/persistent papillary thyroid carcinoma in patients who initially underwent total thyroidectomy and remnant ablation. J Clin Endocrinol Metab. 2011;96(7):2049–2056.
Schuff KG, Weber SM, Givi B, Samuels MH, Andersen PE, Cohen JI. Efficacy of nodal dissection for treatment of persistent/recurrent papillary thyroid cancer. Laryngoscope. 2008;118(5):768–775.
Rondeau G, Fish S, Hann LE, Fagin JA, Tuttle RM. Ultrasonographically detected small thyroid bed nodules identified after total thyroidectomy for differentiated thyroid cancer seldom show clinically significant structural progression. Thyroid. 2011;21(8):845–853.
Robenshtok E, Fish S, Bach A, DomÌnguez JM, Shaha A, Tuttle RM. Suspicious cervical lymph nodes detected after thyroidectomy for papillary thyroid cancer usually remain stable over years in properly selected patients. J Clin Endocrinol Metab. 2012;97(8):2706–2713.
Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26(1):1–133.
Al-Saif O, Farrar WB, Bloomston M, Porter K, Ringel MD, Kloos RT. Long-term efficacy of lymph node reoperation for persistent papillary thyroid cancer. J Clin Endocrinol Metab. 2010;95(5):2187–2194.
Vaisman F, Momesso D, Bulzico DA, et al. Spontaneous remission in thyroid cancer patients after biochemical incomplete response to initial therapy. Clin Endocrinol (Oxf). 2012;77(1):132–138.
Lee SG, Lee WK, Lee HS, et al. Practical Performance of the 2015 American Thyroid Association guidelines for predicting tumor recurrence in patients with papillary thyroid cancer in South Korea. Thyroid. 2017;27(2):174–181.
Tufano RP, Clayman G, Heller KS, et al. Management of recurrent/persistent nodal disease in patients with differentiated thyroid cancer: a critical review of the risks and benefits of surgical intervention versus active surveillance. Thyroid. 2015;25(1):15–27.
Urken ML, Milas M, Randolph GW, et al. Management of recurrent and persistent metastatic lymph nodes in well-differentiated thyroid cancer: a multifactorial decision-making guide for the Thyroid Cancer Care Collaborative. Head Neck. 2015;37(4):605–614.
Acknowledgements
Funding support for this paper is through National Cancer Institute Award Number Grants P50 CA168505 (Thyroid SPORE) and P01 CA124570 from the National Cancer Institute, Award Number Grant KL2TR002734 from the National Center For Advancing Translational Sciences, and Award Number Grant 1T32AI106704-01A1 (Advanced Research Training in Immunology for Surgery Trainees) from the National Institute of Allergy and Infectious Diseases. The research reported in this publication and the content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
All authors declare that they have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Onuma, A.E., Beal, E.W., Nabhan, F. et al. Long-Term Efficacy of Lymph Node Reoperation for Persistent Papillary Thyroid Cancer: 13-Year Follow-Up. Ann Surg Oncol 26, 1737–1743 (2019). https://doi.org/10.1245/s10434-019-07263-5
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-019-07263-5