
Abstract
Background
Gastrointestinal leak (GIL) after cytoreductive surgery with heated intraperitoneal chemotherapy (CRS/HIPEC) is associated with significant morbidity and mortality. This study aimed to identify GIL prognostic factors and its impact on overall survival.
Methods
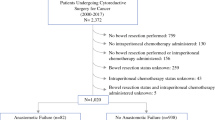
A retrospective analysis of a prospectively maintained database comprising 1270 CRS/HIPEC procedures was performed. Type of GIL, functional and resection status, morbidity, mortality, and survival were reviewed.
Results
Gastrointestinal leaks were identified in 8.7% (110/1270) of CRS/HIPEC procedures, including 53 anastomotic leaks (4.2%), 53 hollow viscus perforations (4.2%), and four leaks at unknown sites. The multivariate predictors of leak were Eastern Cooperative Oncology Group (ECOG) functional status (ECOG 1 vs. 0: odds ratio [OR] 2.12, p = 0.009; ECOG 2 vs. 0: OR 2.90, p = 0.004), and number of anastomoses (OR 5.34; p < 0.0001). The in-hospital mortality rate for the GIL cohort was 21.8% (24/110), with a 72% (80/110) reoperation rate. The leak cohort had a higher major morbidity rate (88.3 vs. 23.3%; p < 0.0001), a longer hospital stay (39.0 vs. 9.9 days; p < 0.0001), and a longer intensive care unit (ICU) stay (7.7 vs. 1.7 days; p = 0.0003). After surgical mortality was excluded, the overall survival periods for the leak and no-leak patients with complete cytoreduction were respectively 1.5 and 4.98 years (p = 0.0001). Clinically significant decreases in survival were observed for all primary malignancies.
Conclusions
Gastrointestinal leak after CRS/HIPEC is a source of significant mortality, with a decrease in overall survival even after complete CRS. Preoperative functional status and number of anastomoses are predictors of leak for CRS/HIPEC patients.

Similar content being viewed by others


References
Levine EA, Stewart JH, Shen P, Russell GB, Loggie BL, Votanopoulos KI. Intraperitoneal chemotherapy for peritoneal surface malignancy: experience with 1000 patients. J Am Coll Surg. 2014;218:573–85.
Glockzin G, Schlitt HJ, Piso P. Peritoneal carcinomatosis: patients selection, perioperative complications, and quality of life related to cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. World J Surg Oncol. 2009;8:1–8.
Ihemelandu CU, Mcquellon R, Shen P, Stewart JH, Votanopoulos K, Levine EA. Predicting postoperative morbidity following cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (CS + HIPEC) with preoperative FACT-C (Functional Assessment of Cancer Therapy) and patient-rated performance status. Ann Surg Oncol. 2013;20:3519–26.
Jacquet P, Sugarbaker PH. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. Cancer Treat Res. 1996;82:359–74.
Sugarbaker PH. Technical Handbook for the Integration of Cytoreductive Surgery and Perioperative Intraperitoneal Chemotherapy Into the Surgical Management of Gastrointestinal and Gynecologic Malignancy. 4th ed. Grand Rapids: The Ludann Company; 2005.
Levine EA, Iv JHS, Russell GB, Geisinger KR, Loggie BL, Shen P. Cytoreductive surgery and intraperitoneal hyperthermic chemotherapy for peritoneal surface malignancy: experience with 501 procedures. J Am Coll Surg. 2007;204:943–53.
Dindo D, Demartines N, Clavien P. Classification of surgical complications. Ann Surg. 2004;240:205–13.
Younan R, Kusamura S, Baratti D, et al. Bowel complications in 203 cases of peritoneal surface malignancies treated with peritonectomy and closed-technique intraperitoneal hyperthermic perfusion. Ann Surg Oncol. 2005;12:910–8.
Sugarbaker PH. Cytoreduction including total gastrectomy for pseudomyxoma peritonei. Br J Surg. 2002;89:208–12.
Elias D, Gilly F, Boutitie F, et al. Peritoneal colorectal carcinomatosis treated with surgery and perioperative intraperitoneal chemotherapy: retrospective analysis of 523 patients from a multicentric French study. J Clin Oncol. 2009;28: 63–8.
Glehen O, Gilly FN, Boutitie F, et al. Toward curative treatment of peritoneal carcinomatosis from nonovarian origin by cytoreductive surgery combined with perioperative intraperitoneal chemotherapy. Cancer. 2010;116:5608–18.
Damrauer SM, Bordeianou L, Berger D. Contained anastomotic leaks after colorectal surgery: are we too slow to act? Arch Surg. 2009;144:333–8.
Desantis M, Bernard JL, Casanova V, et al. Morbidity, mortality, and oncological outcomes of 401 consecutive cytoreductive procedures with hyperthermic intraperitoneal chemotherapy (HIPEC). Langenbecks Arch Surg. 2015;400:37–48.
Saxena A, Yan TD, Morris DL. Critical assessment of preoperative and operative risk factors for complications after iterative peritonectomy procedures. Eur J Surg Oncol. 2010;36:309–14.
Thornton M, Joshi H, Vimalachandran C, Heath R, Carter P, Gur U, Rooney P. Management and outcome of colorectal anastomotic leaks. Int J Colorectal Dis. 2011;26:313–20.
Bartlett EK, Meise C, Roses RE, Fraker DL, Kelz RR, Karakousis GC. Morbidity and mortality of cytoreduction with intraperitoneal chemotherapy: outcomes from the ACS NSQIP database. Ann Surg Oncol. 2014;21:1494–500.
Acknowledgement
This study was supported by Wake Forest University Biostatistics shared resource NCI CCSG P30CA012197.
Disclosure
There are no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Chouliaras, K., Levine, E.A., Fino, N. et al. Prognostic Factors and Significance of Gastrointestinal Leak After Cytoreductive Surgery (CRS) with Heated Intraperitoneal Chemotherapy (HIPEC). Ann Surg Oncol 24, 890–897 (2017). https://doi.org/10.1245/s10434-016-5738-6
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5738-6