
Abstract
Background
Sentinel lymph node biopsy (SLNB) is recommended for patients with intermediate-thickness melanoma, but the use of SLNB for patients with thick melanoma is debated. This report presents a single-institution study investigating factors predictive of sentinel lymph node (SLN) metastasis and outcome for thick-melanoma patients .
Methods
A retrospective review of a single-institution database from 1997 to 2012 identified 147 patients with thick primary cutaneous melanoma (≥4 mm) who had an SLNB. Clinicopathologic characteristics were correlated with nodal status and outcome.
Results
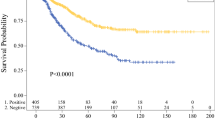
The median age of the patients was 67 years, and 61.9 % of the patients were men. The median tumor thickness was 5.5 mm, and 54 patients (36.7 %) had a positive SLN. Multivariable analysis showed that only tumor thickness significantly predicted SLN metastasis (odds ratio 1.14; 95 % confidence interval (CI) 1.02–1.28; P = 0.02). The overall median follow-up period was 34.6 months. Overall survival (OS) and melanoma-specific survival (MSS) were significantly worse for the positive versus negative-SLN patients. Multivariable analysis showed that age [hazard ratio (HR) 1.04; 95 % CI 1.01–1.07; P = 0.02] and SLN status (HR 2.24; 95 % CI 1.03–4.88; P = 0.04) significantly predicted OS, whereas only SLN status (HR 3.85; 95 % CI 2.13–6.97; P < 0.01) significantly predicted MSS.
Conclusions
Tumor thickness predicts SLN status in thick melanomas. Furthermore, SLN status is prognostic for OS and MSS in thick-melanoma patients, with positive-SLN patients having significantly worse OS and MSS. These findings show that SLNB should be recommended for thick-melanoma patients, particularly because detection of SLN metastasis can identify patients for potential systemic therapy and treatment of nodal disease at a microscopic stage.

Similar content being viewed by others


References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65:5–29.
Balch CM, Gershenwald JE, Soong SJ, et al. Final version of 2009 AJCC melanoma staging and classification. J Clin Oncol. 2009;27:6199–206.
Morton DL, Thompson JF, Cochran AJ, et al. Sentinel-node biopsy or nodal observation in melanoma. N Engl J Med. 2006;355:1307–17.
Morton DL, Thompson JF, Cochran AJ, et al. Final trial report of sentinel-node biopsy versus nodal observation in melanoma. N Engl J Med. 2014;370:599–609.
Wong SL, Balch CM, Hurley P, et al. Sentinel lymph node biopsy for melanoma: American Society of Clinical Oncology and Society of Surgical Oncology joint clinical practice guideline. J Clin Oncol. 2012;30:2912–8.
de Oliveira Filho RS, da Silva AM, de Oliveira DA, Oliveira GG, Nahas FX. Sentinel node biopsy should not be recommended for patients with thick melanoma. Rev Col Bras Cir. 2013;40:127–9.
Gershenwald JE, Mansfield PF, Lee JE, Ross MI. Role for lymphatic mapping and sentinel lymph node biopsy in patients with thick (≥4 mm) primary melanoma. Ann Surg Oncol. 2000;7:160–5.
Ferrone CR, Panageas KS, Busam K, Brady MS, Coit DG. Multivariate prognostic model for patients with thick cutaneous melanoma: importance of sentinel lymph node status. Ann Surg Oncol. 2002;9:637–45.
Faries MB, Thompson JF, Cochran A, et al. The impact on morbidity and length of stay of early versus delayed complete lymphadenectomy in melanoma: results of the Multicenter Selective Lymphadenectomy Trial (I). Ann Surg Oncol. 2010;17:3324–9.
Morton DL, Wen DR, Wong JH, et al. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surg. 1992;127:392–9.
Ross MI, Reintgen D, Balch CM. Selective lymphadenectomy: emerging role for lymphatic mapping and sentinel node biopsy in the management of early-stage melanoma. Semin Surg Oncol. 1993;9:219–23.
Gyorki DE, Sanelli A, Herschtal A, et al. Sentinel lymph node biopsy in T4 melanoma: an important risk-stratification tool. Ann Surg Oncol. 2015;23:579–84.
Yamamoto M, Fisher KJ, Wong JY, et al. Sentinel lymph node biopsy is indicated for patients with thick clinically lymph node-negative melanoma. Cancer. 2015;121:1628–36.
Carlson GW, Murray DR, Hestley A, Staley CA, Lyles RH, Cohen C. Sentinel lymph node mapping for thick (≥4 mm) melanoma: should we be doing it? Ann Surg Oncol. 2003;10:408–15.
Gajdos C, Griffith KA, Wong SL, et al. Is there a benefit to sentinel lymph node biopsy in patients with T4 melanoma? Cancer. 2009;115:5752–60.
Goppner D, Ulrich J, Pokrywka A, Peters B, Gollnick H, Leverkus M. Sentinel lymph node biopsy status is a key parameter to stratify the prognostic heterogeneity of malignant melanoma in high-risk tumors >4.0 mm. Dermatology. 2011;222:59–66.
Gutzmer R, Satzger I, Thoms KM, et al. Sentinel lymph node status is the most important prognostic factor for thick (≥4 mm) melanomas. JDDG J Deutsch Dermatol Ges. 2008;6:198–203.
Thompson JF, Shaw HM. The prognosis of patients with thick primary melanomas: is regional lymph node status relevant, and does removing positive regional nodes influence outcome? Ann Surg Oncol. 2002;9:719–22.
Rughani MG, Swan MC, Adams TS, et al. Sentinel node status predicts survival in thick melanomas: the Oxford perspective. Eur J Surg Oncol. 2012;38:936–42.
Pasquali S, Haydu LE, Scolyer RA, et al. The importance of adequate primary tumor excision margins and sentinel node biopsy in achieving optimal locoregional control for patients with thick primary melanomas. Ann Surg. 2013;258:152–7.
Mozzillo N, Pennacchioli E, Gandini S, et al. Sentinel node biopsy in thin and thick melanoma. Ann Surg Oncol. 2013;20:2780–6.
Fujisawa Y, Otsuka F, Japanese Melanoma Study Group. The benefit of a sentinel lymph node biopsy and adjuvant therapy in thick (>4 mm) melanoma: multicenter, retrospective study of 291 Japanese patients. Melanoma Res. 2012;22:362–7.
Scoggins CR, Bowen AL, Martin RC II, et al. Prognostic information from sentinel lymph node biopsy in patients with thick melanoma. Arch Surg. 2010;145:622–7.
Acknowledgment
This project was supported in part by the Ohse Foundation Research Award, Yale University School of Medicine.
Conflict of Interest
An immediate family member of Stephan Ariyan (son) owns stock and is an employee of Pfizer. An immediate family member of Bonnie Gould Rothberg (husband) owns stock and is director of science at Butterfly Networks Inc., LAM Therapeutics, Quantum Si, and Hyperfine Technologies. There are no other conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bello, D.M., Han, G., Jackson, L. et al. The Prognostic Significance of Sentinel Lymph Node Status for Patients with Thick Melanoma. Ann Surg Oncol 23 (Suppl 5), 938–945 (2016). https://doi.org/10.1245/s10434-016-5502-y
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5502-y