
Abstract
Background
Malignant obstruction in right-sided colon (MORC) has traditionally been treated by emergency resection with primary anastomosis. The aim of this study was to evaluate short-term postoperative and long-term oncologic outcomes according to the surgical approach adopted for MORC.
Methods
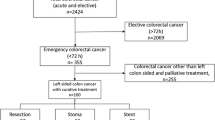
A total of 1785 patients who underwent curative surgery for stage II or III colon cancer in seven hospitals were reviewed retrospectively. Seventy-four of 1785 patients had MORC. We compared the postoperative outcome and long-term oncologic outcome between the emergency surgery (ES) group (49 patients) and the bridge to surgery (BS) group (25 patients) for 74 patients with MORC.
Results
There were no differences in the length of the distal and proximal resection margin (p = 0.820 and p = 0.620) or the number of metastatic lymph nodes (p = 0.221). There were no differences in flatus passage (p = 0.242), start of diet (p = 0.336), hospital stay (p = 0.444), or postoperative morbidity (p = 0.762). The 5-year overall survival rates were 73.2 % in the ES group and 90.7 % in the BS group (p = 0.172). Moreover, the 5-year disease-free survival rates were 71.9 % in the ES group and 76.2 % in the BS group (p = 0.929).
Conclusions
On the basis of the above results, the postoperative course of the ES group was similar to that of the BS group. In addition, the long-term oncologic outcome of the BS group was similar or slightly better than that of the ES group. BS after colonic stent may be an alternative option for MORC.

Similar content being viewed by others


References
Ohman U. Prognosis in patients with obstructing colorectal carcinoma. Am J Surg. 1982;143:742–7.
Setti Carraro PG, Segala M, Cesana B, Tiberio G. Obstructing colonic cancer: failure and survival patterns over a ten-year follow-up after one-stage curative surgery. Dis Colon Rectum. 2001;44:243–50.
Carty N, Corder AP. Which surgeons avoid a stoma in treating left-sided colonic obstruction? Results of a postal questionnaire. Ann Coll Surg Engl. 1992;74:391–4.
Fielding LP, Wells BW. Survival after primary and staged resection for large bowel obstruction caused by cancer. Br J Surg. 1974;61:16–8.
Phillips RKS, Hittinger R, Fry JS, Fielding LP. Malignant large bowel obstruction. Br J Surg. 1985;72:296–302.
Repici A, Adler DG, Gibbs CM, et al. Stenting of the proximal colon in patients with malignant large bowel obstruction: techniques and outcomes. Gastrointest Endosc. 2007;66:940–4.
Tekkis PP, Kinsman R, Thompson MR, Stamatakis JD. The Association of Coloproctology of Great Britain and Ireland study of large bowel obstruction caused by colorectal cancer. Ann Surg. 2004;240:76–81.
Hsu TC. Comparison of one-stage resection and anastomosis of acute complete obstruction of left and right colon. Am J Surg. 2005;189:384–7.
Campbell KL, Hussey JK, Eremin O. Expandable metal stent application in obstructing carcinoma of the proximal colon: report of a case. Dis Colon Rectum. 1997;40:1391–3.
Balague C, Targarona EM, Sainz S, et al. Minimally invasive treatment for obstructive tumors of the left colon: endoluminal self-expanding metal stent and laparoscopic colectomy: preliminary results. Dig Surg. 2004;21:282–6.
Cho YK, Kim SW, Lee BI, et al. Clinical outcome of self-expandable metal stent placement in the management of malignant proximal colon obstruction. Gut Liver. 2011;5:165–70.
Stimac D. Colonic stents for the palliation of malignant colonic obstruction. Dig Dis. 2008;26:336–41.
Bhardwaj R, Parker MC. Palliative therapy of colorectal carcinoma: stent or surgery? Colorectal Dis. 2003;5:518–21.
Maruthachalam K, Lash GE, Shenton BK, Horgan AF. Tumour cell dissemination following endoscopic stent insertion. Br J Surg. 2007;94:1151–4.
Steinert EM, Schwartz RH, Singh NJ. At low precursor frequencies, the T-cell response to chronic self-antigen results in anergy without deletion. Eur J Immunol. 2012;42:2875–80.
Sabbagh C, Chatelain D, Trouillet N, et al. Does use of a metallic colon stent as a bridge to surgery modify the pathology data in patients with colonic obstruction? A case-matched study. Surg Endosc. 2013;27:3622–31.
Kim HJ, Choi GS, Park JS, et al. Higher rate of perineural invasion in stent-laparoscopic approach in comparison to emergent open resection for obstructing left-sided colon cancer. Int J Colorectal Dis. 2013;28:407–14.
Saida Y, Sumiyama Y, Nagao J, Uramatsu M. Long-term prognosis of preoperative “bridge to surgery” expandable metallic stent insertion for obstructive colorectal cancer: comparison with emergency operation. Dis Colon Rectum. 2003;46(10 suppl):S44–9.
Kim JS, Hur H, Min BS, et al. Oncologic outcomes of self-expanding metallic stent insertion as a bridge to surgery in the management of left-sided colon cancer obstruction: comparison with nonobstructing elective surgery. World J Surg. 2009;33:1281–6.
Choi JM, Lee C, Han YM, et al. Long-term oncologic outcomes of endoscopic stenting as a bridge to surgery for malignant colonic obstruction: comparison with emergency surgery. Surg Endosc. 2014;28:2649–55.
Sabbagh C, Browet F, Diouf M, et al. Is stenting as a “bridge to surgery” an oncologically safe strategy for the management of acute, left-sided, malignant, colonic obstruction? A comparative study with a propensity score analysis. Ann Surg. 2013;258:107–15.
Acknowledgment
We thank Jae Im Lee, Byoung-Jo Choi, Ji-Hoon Kim, and other colleagues who helped with data collection in the colorectal division of the Surgery Department from The Catholic University of Korea.
Disclosure
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kye, BH., Lee, Y.S., Cho, HM. et al. Comparison of Long-Term Outcomes Between Emergency Surgery and Bridge to Surgery for Malignant Obstruction in Right-Sided Colon Cancer: A Multicenter Retrospective Study. Ann Surg Oncol 23, 1867–1874 (2016). https://doi.org/10.1245/s10434-015-5053-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-015-5053-7