
Abstract
Background
Radiotherapy (RT) may be omitted for elderly (age >70 years) breast cancer patients with favorable disease [stage I and estrogen receptor (ER)-positive with endocrine therapy]. This study sought to develop a nomogram to predict the survival benefit of RT in elderly patients with stage I & ER-negative or stage II/III (regardless of ER status) disease.
Methods
We used surveillance, epidemiology and end results data to identify 9,079 patients (age ≥70 years) with stage I & ER-negative or stage II/III (regardless of ER status) disease who received breast-conserving surgery between 1990 and 2005. Cancer-specific survival (CSS) was estimated using Kaplan–Meier analysis. Competing-risk regression was used to determine the effect of predictors on CSS. A nomogram was then developed and validated using bootstrapped technique.
Results
With a median follow-up of 83 months, the overall 10- and 15-year CSS were 82.1 and 75.8 %, respectively. RT was significantly associated with improved CSS in the multivariate analysis. A nomogram was developed for the prediction of 10-year CSS and showed a bootstrapped-corrected area under the curve value of 0.679. RT did not deliver any survival benefit to patients with predicted CSS >90 %. In addition, RT significantly increased the 10-year CSS by 3.6 and 10.1 % in patients with predicted CSS from 0.80 to 0.90 and <0.80, respectively.
Conclusions
This nomogram is a useful tool to predict the 10-year CSS in patients with stage I and ER-negative or stage II/III (regardless of ER status) disease. The benefit of RT varied among patients with different predicted CSS.

Similar content being viewed by others


References
Fyles AW, McCready DR, Manchul LA, et al. Tamoxifen with or without breast irradiation in women 50 years of age or older with early breast cancer. N Engl J Med. 2004;351(10):963–70.
Hughes KS, Schnaper LA, Berry D, et al. Lumpectomy plus tamoxifen with or without irradiation in women 70 years of age or older with early breast cancer. N Engl J Med. 2004;351(10):971–7.
Hughes KS, Schnaper LA, Bellon JR, et al. Lumpectomy plus tamoxifen with or without irradiation in women age 70 years or older with early breast cancer: long-term follow-up of CALGB 9343. J Clin Oncol. 2013;31(19):2382–7.
Dignam JJ, Kocherginsky MN. Choice and interpretation of statistical tests used when competing risks are present. J Clin Oncol. 2008;26(24):4027–34.
Bezuhly M, Temple C, Sigurdson LJ, Davis RB, Flowerdew G, Cook EF Jr. Immediate postmastectomy reconstruction is associated with improved breast cancer-specific survival: evidence and new challenges from the Surveillance, Epidemiology, and End Results database. Cancer. 2009;115(20):4648–54.
EBCTCG EBCTaCG. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10 801 women in 17 randomised trials. Lancet. 2011;378(9804):1707–16.
Pötter R, Gnant M, Kwasny W, et al. Lumpectomy plus tamoxifen or anastrozole with or without whole breast irradiation in women with favorable early breast cancer. Int J Radiat Oncol Biol Phys. 2007;68(2):334–40.
Luu C, Goldstein L, Goldner B, Schoellhammer HF, Chen SL. Trends in radiotherapy after breast-conserving surgery in elderly patients with early-stage breast cancer. Ann Surg Oncol. 2013;20(10):3266–73.
Albert JM, Liu DD, Shen Y, et al. Nomogram to predict the benefit of radiation for older patients with breast cancer treated with conservative surgery. J Clin Oncol. 2012;30(23):2837–43.
Fisher B, Jeong JH, Anderson S, Bryant J, Fisher ER, Wolmark N. Twenty-five-year follow-up of a randomized trial comparing radical mastectomy, total mastectomy, and total mastectomy followed by irradiation. N Engl J Med. 2002;347(8):567–75.
Fisher B, Anderson SJ. The breast cancer alternative hypothesis: is there evidence to justify replacing it? J Clin Oncol. 2010;28(3):366–74.
Albert JM, Pan I-W, Shih Y-CT, et al. Effectiveness of radiation for prevention of mastectomy in older breast cancer patients treated with conservative surgery. Cancer. 2012;118(19):4642–51.
Sen S, Wang SY, Soulos PR, et al. Examining the cost-effectiveness of radiation therapy among older women with favorable-risk breast cancer. J Natl Cancer Inst. 2014;106(3):dju008.
Jagsi R, Abrahamse P, Morrow M, et al. Patterns and correlates of adjuvant radiotherapy receipt after lumpectomy and after mastectomy for breast cancer. J Clin Oncol. 2010;28(14):2396–403.
Overgaard M, Jensen MB, Overgaard J, et al. Postoperative radiotherapy in high-risk postmenopausal breast-cancer patients given adjuvant tamoxifen: Danish Breast Cancer Cooperative Group DBCG 82c randomised trial. Lancet. 1999;353(9165):1641–8.
Acknowledgment
We thank Caiyun Liao, MD, for extensive discussion about the statistical analysis. This study was supported by grants from the National Natural Science Foundation of China (81402201/H1622).
Conflict of interests
The authors have no conflict of interests to disclose.
Author information
Authors and Affiliations
Corresponding authors
Electronic supplementary material
Below is the link to the electronic supplementary material.
10434_2015_4393_MOESM3_ESM.pdf
Survival benefit of RT on cumulative CSS in patients with T1 disease (3a), pN0 disease (3b), Stage I disease (3c), or ER (+) disease (3d). Unadjusted Cox regression was used. Cumulative incidence function of patients who received or did not receive RT is shown in patients with T1 disease (3e), pN0 disease (3f), Stage I disease (3 g), or ER (+) disease (3 h). Competing risk analysis was used. RT radiotherapy; HR hazard ratio; CI confidence interval; CSS cancer-specific survival; SHR subhazard ratio (PDF 223 kb)
10434_2015_4393_MOESM4_ESM.pdf
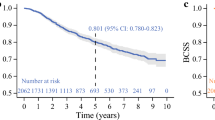
Internal validation of the nomogram. (a) ROC analysis (AUC = 0.687) and (b) calibration plots. A Hosmer-Lemeshow test P value of 0.99 indicated a high level of agreement between the predicted and actual probability values. (c) Cumulative CSS by the nomogram and (d) cumulative CSS by AJCC stage. AJCC American Joint Committee on Cancer; AUC area under the curve; CSS cancer-specific survival; ROC receiver-operator curve (PDF 108 kb)
10434_2015_4393_MOESM5_ESM.pdf
Patient population was classified as low- (P css ≥ 0.90; a and d), intermediate- (0.80 P css < 0.90; b and e), and high-risk (P css < 0.80; c and f) subgroups based on the predicted CSS. The survival benefits of RT on CSS are shown in a, b, and c. The cumulative incidence function for improvements according to the benefit of RT is shown in e, f, and g. CSS cancer-specific survival; RT radiotherapy (PDF 155 kb)
Rights and permissions
About this article

Cite this article
Chen, K., Su, F. & Jacobs, L.K. A Nomogram to Predict the Benefit of Radiation Therapy After Breast-Conserving Surgery in Elderly Patients with Stage I & ER-Negative, or Stage II/III Disease. Ann Surg Oncol 22, 3497–3503 (2015). https://doi.org/10.1245/s10434-015-4393-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-015-4393-7