
Abstract
Background
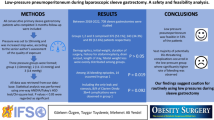
Our purpose was to evaluate the perioperative safety of laparoscopic-assisted distal gastrectomy (LADG) in elderly patients with clinical stage I gastric cancer.
Methods
From 527 consecutive patients who underwent distal gastrectomy for gastric cancer from 2000 to 2011, 38 elderly patients (aged 75 years or older) with clinical stage I disease who underwent LADG were compared with 28 elderly patients who underwent open distal gastrectomy (ODG) and with 41 nonelderly patients (younger than aged 65 years) who underwent LADG. Intraoperative cardiopulmonary changes following pneumoperitoneum and surgical outcomes were analyzed.
Results
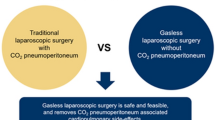
A significant elevation in mean blood pressure (MAP) (by 44 %) and slight increase in heart rate (HR) (by 13 %) were observed 5 min after the beginning of pneumoperitoneum in the elderly LADG group, although they tended to remain stable since 30 min. The elevation of end-tidal CO2 (ETCO2) in the elderly LADG group remained at 8 % and did not differ from that in the nonelderly LADG group who were 20.5 years (median) younger, whereas percutaneous oxygen saturation (SpO2) did not worsen. Compared with the elderly ODG group, the elderly LADG group did not increase intraoperative cardiopulmonary impairment or complication, had lower incidence of postoperative medical complication (7.9 vs. 32.1 %, p = 0.012) and shortened postoperative recovery course (25 vs. 15 days, p < 0.001). Pneumoperitoneum did not necessarily impair cardiopulmonary dynamics or prognosis for elderly patients with declining cardiopulmonary function.
Conclusions
Cardiopulmonary impairment caused by pneumoperitoneum was not critical but transitory. LADG led to superior perioperative course for elderly patients with early gastric cancer.

Similar content being viewed by others

References
Siegel R, Naishadham D, Jemal A. Global cancer statistics. Cancer J Clin. 2013;63:11–30.
Japanese Gastric Cancer Association. Gastric Cancer treated in 2005 in Japan. http://www.jgca.jp/.
Damhuis RA, Tilanus HW. The influence of age on resection rates and postoperative mortality in 2773 patients with gastric cancer. Eur J Cancer. 1995;31A:928–31.
Kitamura K, Sugimachi K, Saku M. Evaluation of surgical treatment for patients with gastric cancer who are over 80 years of age. Hepatogastroenterology. 1999;46:2074–80.
Japan Society for Endoscopic Surgery. 11th Nationwide Survey of Endoscopic Surgery in Japan. J Jpn Soc Endosc Surg. 2012;17:571–694.
Kitano S, Shiraishi N, Fujii K, et al. A randomized controlled trial comparing open vs laparoscopy-assisted distal gastrectomy for the treatment of early gastric cancer: an interim report. Surgery. 2002;131:S306–11.
Kim HH, Hyung WJ, Cho GS, et al. Morbidity and mortality of laparoscopic gastrectomy versus open gastrectomy for gastric cancer: an interim report- a phase III multicenter, prospective, randomized trial (KLASS trial). Ann Surg. 2010;251:417–20.
Takiguchi S, Fujiwara Y, Yamasaki M, et al. Laparoscopy-assisted distal gastrectomy versus open distal gastrectomy. A prospective randomized single-blind study. World J Surg. 2013;37:2379–86.
Kunisaki C, Makino H, Takagawa R, et al. Efficacy of laparoscopy-assisted distal gastrectomy for gastric cancer in the elderly. Surg Endosc. 2009;23:377–83.
Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011;14:101–12.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–13.
Japanese Gastric Cancer Association. Japanese gastric cancer treatment guideline 2010 (ver. 3). Gastric Cancer. 2010;14:113–23.
Tokunaga M, Hiki N, Fukunaga T, Miki A, Ohyama S, Seto Y, Yamaguchi T. Does age matter in the indication for laparoscopy-assisted gastrectomy? J Gastrointest Surg. 2008;12:1502–7.
Cho GS, Kim W, Kim HH, Ryu SW, Kim MC, Ryu SY. Multicentre study of the safety of laparoscopic subtotal gastrectomy for gastric cancer in the elderly. Br J Surg. 2009;96:1437–42.
Sharma KC, Brandstetter RD, Brensilver JM, Jung LD. Cardiopulmonary physiology and pathophysiology as a consequence of laparoscopic surgery. Chest. 1996;110:810–5.
Schulze S, Lyng KM, Bugge K, et al. Cardiovascular and respiratory changes and convalescence in laparoscopic colonic surgery. Arch Surg. 1999; 134:1112–8.
Harris SN, Ballantyne GH, Luther MA, Perrino AC. Alterations of cardiovascular performance during laparoscopic colectomy: a combined hemodynamic and echocardiographic analysis. Anesth Analg. 1996;83:482–7.
Galizia G, Prizio G, Lieto E, et al. Hemodynamic and pulmonary changes during open, carbon dioxide pneumoperitoneum, and abdominal wall-lifting cholecystectomy: a prospective, randomized study. Surg Endosc. 2001;15:477–83.
Senagore AJ, Whalley D, Delancy CP, Mekhail N, Duepree HJ, Fazio VW. Epidural anesthesia–analgesia shortens length of stay after laparoscopic colectomy for benign pathology. Surgery. 2001;129:672–6.
Disclosure
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Suzuki, S., Nakamura, T., Imanishi, T. et al. Carbon Dioxide Pneumoperitoneum Led to No Severe Morbidities for the Elderly During Laparoscopic-Assisted Distal Gastrectomy. Ann Surg Oncol 22, 1548–1554 (2015). https://doi.org/10.1245/s10434-014-4182-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-014-4182-8